Introduction
Older adults comprise a highly heterogeneous population where the transition from a state of robust health to frailty is influenced by a multitude of factors.1–4 The deterioration of the health status is characterized by a progressive rise in the incidence of comorbidities, sometimes resulting in an increased intake of drugs. Concurrently, a decline in overall functional capacity and the reserve capacity of various organ systems collectively elevate the risk of treatment-related toxicities in older patients. There is an ongoing effort globally, as well as in Switzerland, aimed at bringing the field of geriatric oncology forward in conventional healthcare centers and establishing comprehensive practices serving the needs of older cancer patients.5,6 A GA is defined as a multi-dimensional, interdisciplinary diagnostic process focused on determining the medical, psychological and functional capability of a frail older person in order to develop a coordinated, integrated plan for treatment.7,8 The guidelines of the American Society of Clinical Oncology (ASCO) and the International Society of Geriatric Oncology (SIOG) for practical assessment and management of vulnerabilities in older patients receiving chemotherapy recommend evaluating the following health-related domains during GA: functional status, comorbidity, cognition, mental health status, fatigue, social status and support, nutrition, mobility and presence of geriatric syndromes,9–11 with each of the domains being assessed using specific tools and questionnaires. At the joint session organized by the European Society for Medical Oncology (ESMO) and the SIOG at the annual ESMO 2023 congress, Prof. Laura Biganzoli, the Co-Chair of the ESMO/SIOG Cancer in the Elderly Working Group, presented an overview of the recent data supporting the integration of GA into routine geriatric oncology care, as well as discussed the updated recommendations for the practical assessment and management of vulnerabilities in older patients receiving systemic cancer therapies.12 This paper summarizes the data from selected recent studies including those discussed at the ESMO/SIOG joint session that evaluated the benefits of GA and GA-driven interventions on clinical outcomes of geriatric patients with cancer.
Effects of GA on the treatment course
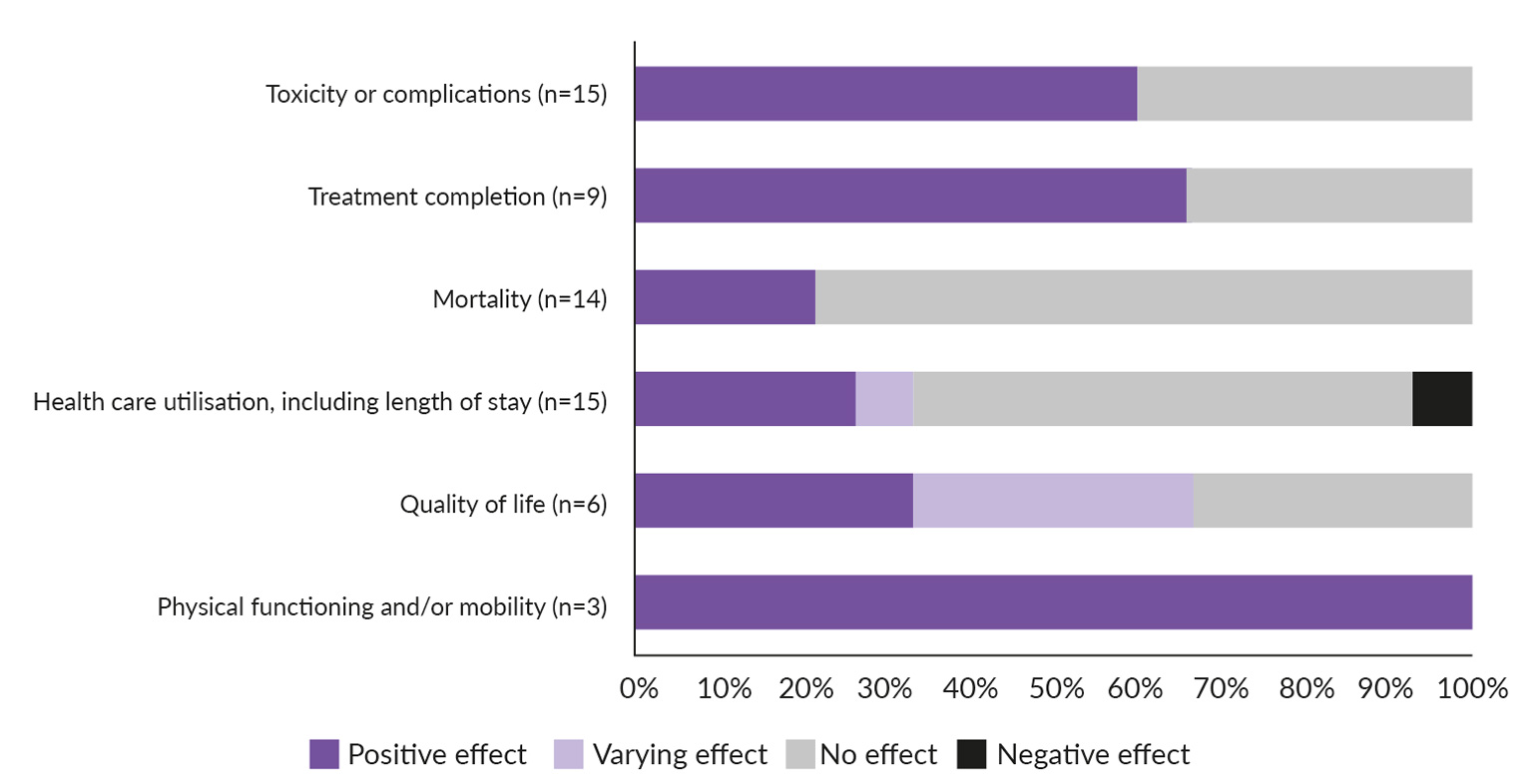
A recent systematic review analyzed available data on the effect of GA on oncologic treatment decisions, the implementation of non-oncologic interventions, patient-doctor communication and treatment outcomes in older patients with cancer.13 In total, 65 publications from 61 studies have been included in the analysis. The study demonstrated that, after GA, the oncologic treatment plan was modified in a median of 31% of patients, with the highest change rates observed in studies utilizing a multidisciplinary team evaluation approach. Non-oncologic interventions were recommended in over 70% of patients when an intervention plan or specialized expertise was available. Importantly, the implementation of GA resulted in lower rates of toxicity and treatment-related complications, especially when GA outcomes were considered at the decision-making stage (Figure 1). Furthermore, GA increased treatment completion rates, enhanced physical functioning, as well as facilitated discussions about goals of care and improved communication between patients and caregivers. These data show that GA has the potential to reshape oncologic treatment plans and improve clinical and patient-centered outcomes.
_on_the_course_of_treatment_and_outcomes_in_older_pati.jpg)
An important aspect of GA that can significantly impact the treatment plan is the engagement of patients in conversations about their health and QoL.14 This encompasses not only therapeutic options, prognosis and potential side effects, but also the individual goals and aspirations of patients for the future. To facilitate shared decision-making (SDM) in cancer care, a structured approach should be adopted that goes beyond mere explanations of cancer survival statistics, enabling clinicians to select an effective communication strategy that can be utilized to share information with patients in a timely manner, reduce anxiety and align with the patient’s personal preferences and most important life goals. Furthermore, it is crucial to consider patient frailty, cognitive impairment and emotional responses when making treatment decisions. To address the challenges of implementing SDM in clinical practice, the involvement of multidisciplinary teams of physicians and caregivers, including palliative care experts and psychologists, is essential to develop individualized strategies to manage the disease according to the patient’s unique needs.14–16
Geriatric assessment and management of cancer treatment toxicity
One of the primary goals of geriatric oncology care is to minimize the toxicity of cancer treatments. A recent systematic review and meta-analysis evaluated the impact of comprehensive GA in older cancer patients on treatment outcomes, including toxicity, based on 19 full-text articles representing 17 randomized controlled trials (RCTs).17 The analysis demonstrated no difference in the risk of mortality, hospitalizations, early treatment discontinuations, initial dose reductions and subsequent dose reductions between comprehensive GA assessment and the usual care. However, comprehensive GA was associated with a statistically significant decrease in the risk of treatment toxicity (relative risk [RR]: 0.78 [95% CI: 0.70–0.86]) indicating its potential to optimize treatment strategies in this population. Yet, it is important to note that GA benefits are evident when GA outcomes are considered before treatment selection at the decision-making stage. A recent randomized 5C study found no difference in QoL, survival, changes in the treatment plan, unplanned hospitalizations or emergency department visits and treatment toxicity when GA was administered on or after treatment initiation per patient request18 suggesting that the implementation of GA early in the treatment course is crucial to lowering the toxicity risk.
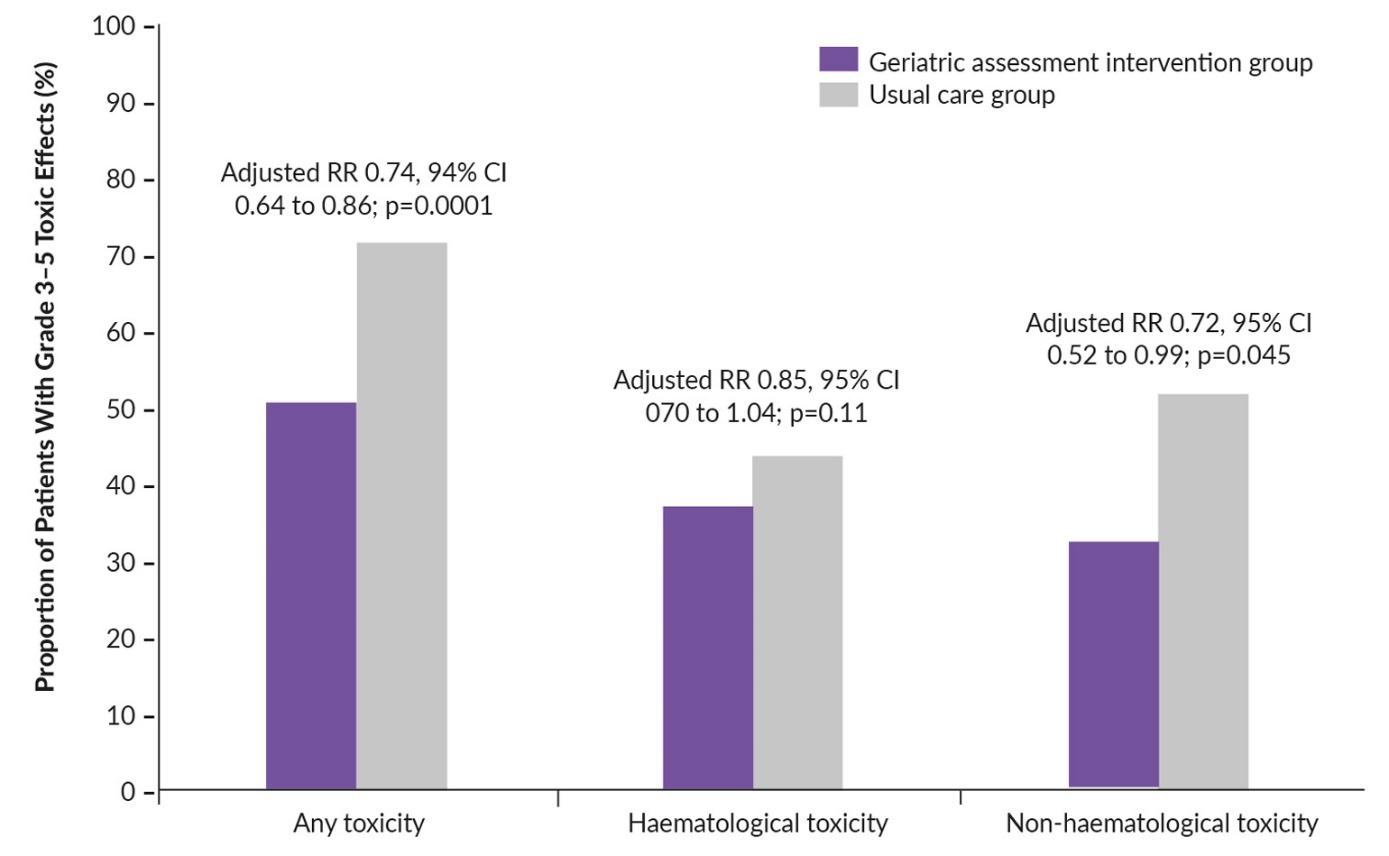
Two recent trials that evaluated the potential of GA interventions to decrease serious toxic effects in older patients with advanced cancer receiving high-risk treatments such as chemotherapy are described in detail below. The cluster-randomized GAP70+ trial19 enrolled 718 patients aged ≥70 years with incurable solid tumors or lymphoma and at least one impaired GA domain other than polypharmacy who were starting a new chemotherapy regimen or another treatment with similar toxicity risks. In total, 40 community oncology practice clusters in the USA were randomly assigned at a 1:1 ratio to the GA intervention or usual care. In the intervention arm, oncologists were provided with a tailored GA summary and management recommendations, including cancer treatment considerations, before the start of the treatment. In the study population, the most represented tumor types were gastrointestinal cancer (34.2%), lung cancer (25.1%) and genitourinary cancer (15.2%); 87.5% of patients had stage IV metastatic disease and 88.2% received chemotherapy as the new cancer treatment. The baseline demographic characteristics and the mean number of GA domain impairments were not significantly different between the study arms. The primary endpoint was the proportion of patients who had grade ≥3 toxicity within the first 3 months of the treatment assessed by a clinician according to the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE), version 4. Other endpoints included survival rates at 6 months, treatment decisions, functional and physical decline and patient-reported toxicities.
The study yielded positive results showing the advantages of comprehensive GA in terms of overall toxicity rates (RR: 0.74 [95% CI: 0.64–0.86]; p=0.0001).19 The prevalence of grade ≥3 toxicity over 3 months in the GA intervention arm was 51% compared with 71% in the usual care arm (Figure 2). The benefits of GA intervention were especially prominent in the case of non-hematological toxicity (32% vs 52% with GA intervention vs usual care, respectively).

The randomized Geriatric Assessment–Driven Intervention (GAIN) trial evaluated the effects of GA-driven interventions on the incidence of chemotherapy-related toxic effects in 605 patients (aged ≥65 years) with solid tumors at all stages who were starting a new chemotherapy regimen.20 All patients received a baseline GA and then were randomized 2:1 to a GA-driven intervention plus standard of care (SoC) or SoC only. In the intervention arm, GA was reviewed by a multidisciplinary team who provided recommendations for interventions. Patients were followed up until chemotherapy completion or 6 months after initiation. The cancer types in the study population included gastrointestinal (33.4%), breast (22.5%), lung (16.0%), genitourinary (15.0%), gynecologic (8.9%) and other (4.1%) tumors. In total, 71.4% of patients had stage IV disease. The primary endpoint was the rate of grade ≥3 toxicity and secondary endpoints included advance directive completion, unplanned hospitalizations, emergency room visits and average length of hospital stay. Similarly to the GAP70+ trial, GAIN demonstrated the benefits of GA plus SoC over SoC only for reducing overall toxicity rates (50.5% vs 60.4%, p=0.02), as well as for the incidence rates of hematological (11.3% vs 19.3%, p=0.003) and non-hematological (18.1% vs 26.2%, p=0.008) toxicity.
In summary, both studies showed that GA interventions can significantly reduce the risk of severe toxicity, indicating that their implementation into oncology clinical practice should be considered as SoC among older adults receiving chemotherapy.
Towards updated treatment guidelines on GA in older patients with cancer
The accumulating evidence of the GA benefits suggested a need for change in clinical practice and prompted an update of the ASCO guidelines for the assessment and management of vulnerabilities in older cancer patients. In order to unequivocally demonstrate the efficacy of GA interventions and define relevant intervention strategies, a panel of ASCO experts conducted a systematic review to identify relevant publications between January 2016 and December 2022.21 To be eligible for the analysis, the publications should have included a study population of ≥100 patients (aged ≥65 years) across study arms; evaluated GA interventions (GA-guided management, GA-driven or -based intervention, GA integrated into oncology care, GA with or without tailored follow-up); performed comparisons of GA versus SoC or usual care; and evaluated relevant clinical outcomes including mortality, overall survival (OS), chemotherapy completion without dose reductions or delays, treatment-related toxicity, patient satisfaction with communication about aging-related concerns, health-related QoL and functional and nutritional status.
A total of 26 publications met the eligibility criteria and formed the evidentiary basis for the update, including primary reports of RCTs, reports of secondary analyses of data from the primary RCTs, systematic reviews and meta-analyses, reports of clinician surveys and systematic and narrative literature reviews.21 Apart from the above-mentioned GAP70+ and GAIN trials, results of the following RCTs have been taken into consideration: GERICO22 which evaluated the effect of GA intervention in frail older patients with colorectal cancer on chemotherapy completion and adherence to cancer treatment; Tailored GA follow-up23 that assessed adherence to cancer treatment in older patients with head and neck, lung, upper gastrointestinal tract or colorectal cancer; COACH24 assessing patient satisfaction with intervention in the older population with advanced solid tumors or lymphoma; 5Cl25 and INTEGeRATE26 trials evaluating QoL in patients with solid tumors, lymphoma or myeloma; EGeSOR27 and HEME28 which had functional outcomes and OS as primary endpoints in older patients with head and neck cancer and hematologic malignancies, respectively.
The study demonstrated that GA and GA-guided management led to significantly less chemotherapy toxicity and better adherence to chemotherapy compared with SoC, as well as improved patient-centered outcomes, communications about aging concerns and completion of advanced directives.21 Importantly, the evidence for GA intervention benefits was greater in the most vulnerable patient groups. While these effects were the strongest for older adults receiving chemotherapy, the expert panel advised expanding GA interventions to any systemic therapy including targeted therapy or immunotherapy, based on early evidence of similar benefits. These conclusions were supported by a recent systematic review and meta-analysis of the data from six trials evaluating treatment toxicity in older cancer patients29 which demonstrated a statistically significant reduction of severe toxicity risk in the experimental arm of the studies that received some form of GA or at least an advice regarding GA-based intervention (risk ratio: 0.78 [95% CI: 0.70–0.86]). Together, these findings confirmed the benefits of GA when performed before decision-making and paved the way for updates in clinical guidelines for the treatment of older patients with cancer.
Updated ASCO guidelines and practical tools for assessment and management of vulnerabilities in older patients with cancer
Based on the analysis of the cumulative data,21 the expert panel concluded that it is essential to perform a GA for older adults with cancer to provide appropriate care when considering systemic therapy and issued a respective update in the ASCO Guidelines for the Practical Assessment and Management of Vulnerabilities in Older Cancer Patients Receiving Systemic Cancer Therapy. The update includes the following statements.
-
Recommendation 1.1. (Updated) All patients with cancer of age ≥65 years with GA-identified impairments should have a GA-guided management included in their care plan. GA management includes using GA results to 1) inform cancer treatment decision-making and 2) address impairments through appropriate interventions, counseling and/or referrals.
-
Amendment 1.1a. This includes older adults receiving systemic therapy, including chemotherapy, targeted therapy, or immunotherapy.
-
Recommendation 2.1. (Updated) A GA should include high-priority aging-related domains known to be associated with outcomes in older patients with cancer to include assessment of physical and cognitive function, emotional health, comorbid conditions, polypharmacy, nutrition and social support.21
While GA is clearly important for geriatric oncology care, there are certain obstacles leading to low rates of GA implementation in routine clinical practice. These include the lack of adequate resources in terms of qualified geriatricians and financial support, as well as insufficient knowledge and training among physicians. In order to broaden the application of GA, ASCO in collaboration with Cancer and Aging Research Group (CARG) and SIOG has made a proposal of a structured Practical Geriatric assessment (PGA) tool30 which contains suggested definitions of impairments, a scoring system, recommendations and information on the measures to be investigated in each domain, inter alia (Supplement 1. Reprinted with permission. © 2024 American Society for Clinical Oncology. All rights reserved).
Conclusions
Multidisciplinary management of cancer patients is essential for improvements in clinical outcomes and the quality of care. The cumulative data show that GA followed by GA-guided management provides significant benefits for older patients with cancer receiving systemic therapies in terms of reducing treatment toxicity, increasing treatment adherence, as well as improving communications about aging concerns and patient-centered outcomes. The evidence for GA interventions is the strongest in vulnerable patients and those receiving a chemotherapy-based regimen. The recent update in the ASCO Guidelines for the Practical Assessment and Management of Vulnerabilities in Older Cancer Patients Receiving Systemic Cancer Therapy aims to widespread GA and GA-guided interventions to advance the quality of oncology care in the geriatric population.
Conflict of interest
Marcus Vetter received honoraria for serving on advisory boards from AstraZeneca and GSK, honoraria for consultancy from GSK, Roche, Novartis, Exact Sciences, Pfizer, Stemline, AbbVie and ASC Oncology, and grant support from GSK. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way. Verene Dougoud has declared that the manuscript was written in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors have declared that no financial support was received from any organization for the submitted work.
Author contributions
All authors have contributed to and approved the final manuscript.