

DLBCL: treatment options and challenges
DLBCL is the most prevalent subtype of non-Hodgkin lymphoma (NHL) in Western countries.1 According to a pooled analysis of tumor registries from 17 Swiss cantons, DLBCL constituted 30% of NHL cases over 30 years.2 DLBCL is characterized by high morphological, molecular and clinico-pathological heterogeneity,3,4 as well as by an aggressive progression course, with a median survival of less than one year if left untreated.5 Despite recent advances in treatment strategies, managing DLBCL remains challenging. The introduction of monoclonal antibodies into chemotherapy regimens has greatly improved clinical outcomes for DLBCL patients. Currently, the most commonly used initial treatment option is a combination of cyclophosphamide, doxorubicin, vincristine and prednisone with the CD20-targeting monoclonal antibody rituximab (R-CHOP). Alternatively, the addition of an antibody-drug conjugate polatuzumab vedotin in a Pola-R-CHP regimen has shown superior progression-free survival (PFS) and is a valid first-line option for patients with DLBCL.6 Other alternatives include an intensified etoposide-containing scheme (R-CHOEP) or a related regimen (R-Dose adjusted EPOCH).4,7,8 Yet, up to 40% of patients will experience treatment failure or relapse.9 For patients with relapsed or refractory disease, the long-time standard of care has been second-line chemoimmunotherapy followed by autologous hematopoietic stem-cell transplantation (HSCT). However, many patients were ineligible for HSCT due to comorbidities or have disease refractory to second-line chemoimmunotherapy. Moreover, long-term disease-free survival (DFS) was only about 50% for those who undergo HSCT. Patients refractory to or relapsing after second-line therapy face a very poor prognosis.4,8,10 Therefore, there is an ongoing effort to improve treatment outcomes using novel emerging options, such as antibody-drug conjugates, immunomodulatory agents, bispecific antibodies and CAR T-cell therapies.8
Unique aspects of DLBCL therapy in older patients
Treating older and very old patients with DLBCL poses a particularly difficult challenge. More than 50% of DLBCL cases occur in individuals over 60 years of age, with the median age of diagnosis being 70 years old.7 Age has been identified as an important predictor of survival in DLBCL patients.11–13 Moreover, treatment is frequently linked to increased toxicity and reduced efficacy, especially in older males aged ≥80 years, who display particularly inferior outcomes.14 Geriatric patients usually have reduced tolerance to chemotherapy due to limited bone marrow reserves, altered drug metabolism, the presence of comorbidities, and impaired physical and cognitive functions.7 The outcomes of HSCT in older patients with DLBCL are similar to the younger individuals; however, the minority of patients older than 65 years are eligible for HSCT due to the lack of tolerability of chemotherapy.15,16 As the global population continues to age, oncologists will increasingly face the challenge of managing older DLBCL patients while carefully balancing treatment efficacy and tolerability in the context of comorbidities and age-related organ dysfunction. Therefore, there is a need for alternative options to improve clinical outcomes in this constantly growing difficult-to-treat older population.
CAR T-cell therapy for DLBCL
The emergence of CAR T-cell therapies has changed the treatment landscape for hematologic malignancies including DLBCL.17–21 The generation of CAR T-cells involves ex vivo cell modification to express a CAR in addition to T cell receptors (TCR), allowing for specific targeting of tumor antigens and counteracting cancer immune evasion mechanisms. The second-generation CAR constructs are composed of a specificity-conferring extracellular antibody single chain variable fragment (scFv), a hinge region transmembrane domain, intracellular costimulatory domains (usually CD28 or 4-1BB) and a TCR CD3ζ signaling chain.22 The later generations also express additional costimulatory signaling domains, cytokines, chemokines, or suicide genes to enhance the efficacy and safety of the treatment.22,23 The second-generation CAR T-cell products discussed in this paper belong to an autologous CAR T-cell therapy targeting CD19 antigen which - as a pan B-cell marker - is thus also expressed on mature B-cell lymphoma as well as B-cell acute lymphoblastic leukemia cells.
Axicabtagene ciloleucel (axi-cel; Yescarta®),24 which incorporates CD28 costimulatory domain, is approved by regulatory agencies, including Swissmedic, to treat patients with DLBCL who are refractory to frontline chemotherapy or relapse within 12 months of the completion of frontline chemotherapy, as well as in the third-line setting or later.24 In the pivotal, single-arm, phase II ZUMA-1 trial,25 axi-cel demonstrated durable responses in patients after ≥2 prior lines of therapy and were considered chemotherapy-refractory based on progression on the previous treatment line or relapse within <12 months after autologous HSCT. A recently published 5-year follow-up of the study26 reported sustained efficacy of axi-cel, with an objective response rate (ORR) of 83%, overall survival (OS) rate of 42.6% and disease-specific survival of 51%. In the phase III ZUMA-7 trial,27 axi-cel in the second-line setting demonstrated significantly longer event-free survival (EFS), PFS and OS over the standard of care (SoC) in DLBCL, with OS benefits observed in 74% of patients with primary refractory disease and other high-risk features.28,29
Tisagenlecleucel (tisa-cel, Kymriah®)30 is a CAR T-cell product incorporating a 4-1BB costimulatory domain. In the pivotal phase II JULIET study,31 tisa-cel produced high rates of durable responses in patients with relapsed/refractory DLBCL after ≥2 prior lines of therapy. The ORR was 53%, including 45% of complete response (CR) rates at a long-term (40.3 months) follow-up.32 Lisocabtagene maraleucel (liso-cel; Breyanzi®),33 also incorporates a 4-1BB costimulatory domain in the CAR construct; however, in contrast to the other two products, the manufacturing of liso-cel involves separate selection, transduction and expansion of autologous CD4+ and CD8+ cells, allowing for consistent dosing of CD4+ and CD8+ CAR T-cells in each patient.34 The phase III TRANSFORM study showed improved EFS and PFS rates for liso-cel over SoC as second-line treatment in patients with early relapsed or refractory LBCL, with 18-month OS rates of 73% for liso-cel versus 54% for SoC.35
Although these studies had certain limitations, such as the lack of examination of CD19 expression on progressive tumors, determination of CAR T cells expansion in blood at progression, ex vivo evaluation of CAR T-cell function at progression, or elucidation of resistance mechanisms associated with tumor size or inflammation,29 CAR T-cell immunotherapy is evolving as a new SoC for the first relapse within 12 months of first-line treatment of refractory DLBCL or refractory disease.17,18,20,21
CAR T-cell therapy in the geriatric population: Study results
While representing a promising strategy for the management of hematologic malignancies, CAR T-cell therapy is associated with significant toxicity. These include cytokine release syndrome (CRS), which can lead to hypotension, hypoxia, organ injury and delirium, neurologic toxicity such as immune effector cell associated neurologic syndrome (ICANS), immune effector cell-associated hematotoxicity, hypogammaglobulinemia and infections.36–38 Although the feasibility of aggressive regimens in older patients has been proved,7,15,16 there may be a preconceived opinion among physicians that this vulnerable group is not fit or will not gain substantial benefits from intensive treatments.39 However, is this concern justified in the case of CAR T-cell products? Recent studies show that age per se is not the contraindication of the therapy. On the contrary, the treatment outcomes were as effective or even better in patients aged 65 or above as in younger subjects.29,40,41 The results of several recent studies which included analysis of CAR T-cell therapy outcomes in older patients are discussed in detail below. The main features of these studies are summarized in Table 1.
ZUMA-1
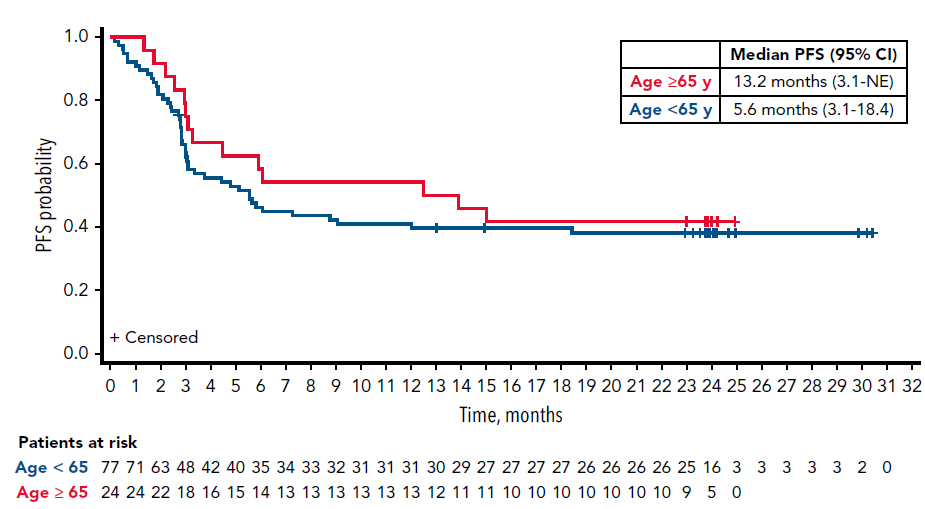
Neelapu and colleagues (2020) performed a post hoc subgroup analysis of 2-year results from the phase I/II ZUMA-1 trial in patients with aggressive B-cell NHL, the majority of which had relapsed or refractory DLBCL.42 The patients were divided into two subgroups according to age (≥65 years and <65 years old) that were matched with respect to disease stage, tumor burden and number of prior therapy lines. One dose of axi-cel was administered after a conditioning regimen of cyclophosphamide and fludarabine, and the patients were followed up for a minimum of 24 months from the axi-cel infusion. The analysis revealed nearly identical outcomes in both age subgroups, with a slight tendency in favor of the older cohort. ORR were 92% and 81% for patients aged ≥65 and <65 years, respectively, with a higher proportion of patients in the older group reaching CR as the best response (75% vs 53%). The median duration of response (DOR) was 12.0 months versus 8.1 months and the median PFS was 13.2 months versus 5.6 months in ≥65 and <65-year-old groups, respectively (Figure 1). The 24-month OS rates were 54% in the older cohort and 49% in the younger group.
_by_age_group_in_zuma-1_patients_treated_with_axicabtagene_.jpg)
Notably, the incidence of grade ≥3 CRS was similar and relatively low between the two age groups (7% vs 12% for ≥65 years vs <65 years, respectively). The most common grade ≥3 AEs were cytopenias, which also occurred at similar rates in patients ≥65 and <65 years old. However, the rates of grade ≥3 neurologic events were higher in the older age cohort as compared to younger patients (44% vs 28%, respectively), with encephalopathy being the most common neurologic AE in both groups (30% vs 21%). Grade ≥3 infections were reported in 19% and 31% of patients ≥65 and <65 years of age, respectively.42 These findings are consistent with the previous pooled age-based evaluation of CRS and neurotoxicity incidence in 214 patients with LBCL enrolled in clinical trials of tisa-cel and axi-cel.49
ZUMA-7
In a preplanned subgroup analysis of the phase III ZUMA-7 trial,28,29 EFS, safety and patient-reported outcomes (PROs) were evaluated over SoC (chemoimmunotherapy followed by high-dose chemotherapy with autologous HSCT) in the subgroup of patients aged ≥65 years.43 Patients were randomized to receive axi-cel (n=51) or SoC (n=58). Baseline characteristics were generally balanced between the treatment arms, although more patients in the axi-cel arm had disease with high-risk features. Overall, 70% of patients had primary refractory disease.
The study demonstrated improved efficacy of axi-cel in older patients compared with SoC.43 At a median follow-up of 24.3 months, the median EFS was longer with axi-cel versus SoC (21.5 vs 2.5 months; HR: 0.276; p<0.0001) (Figure 2A). ORR was 88% (including 75 % CRs) versus 52% (including 33% CRs) with axi-cel versus SoC, respectively (Figure 2B). OS evaluated as a preplanned interim analysis was longer in the axi-cel versus the SoC arm (HR: 0.517 [95% CI: 0.277–0.964]), with OS at 2 years being 64% and 51%, respectively.
_(a)_and_best_response_rates_(b)_in_patients_aged_65_years_in_th.jpeg)
The rates of grade ≥3 AEs were numerically higher in patients aged ≥65 years compared with the overall study population.43 In the older subgroup, grade ≥3 AEs were reported in 94% of patients treated with axi-cel versus 82% in the SoC arm, with the most common grade ≥3 AE being neutropenia (80% vs 44%). CRS occurred in 98% of axi-cel-treated older patients (grade ≥3, 8%; no grade 5 events reported). In the quality of life (QoL) analysis, the mean change in PRO scores from baseline to days 100 and 150 evaluated in 88 patients by the EORTC QLQ-C30 Global Health, Physical Functioning and EQ-5D-5L visual analog scale was better in the axi-cel group (n=46) than in the SoC group (n=42) (p<0.05). In summary, axi-cel demonstrated improved efficacy, PROs and a manageable safety profile in older patients with relapsed or refractory LBCL.
The Center for Medicare & Medicaid Services database study
While randomized controlled trials remain the gold standard in the evaluation of CAR T-cell therapy outcomes, valuable additional information can also be obtained through real-world evidence (RWE) studies. Chihara et al. (2023) utilized the Center for Medicare & Medicaid Services database to report the RWE of CAR T-cell therapy efficacy and costs in older patients with DLBCL.44 The database encompassed records of over 70,000 patients who received treatment through Medicare fee-for-service plans and were diagnosed with DLBCL between April 2016 and December 2020. Within this population, 551 older individuals (aged ≥65 years) who underwent CAR T-cell therapy as the third line and beyond were included in the study. Overall, the analysis demonstrated favorable outcomes, with a median EFS following CAR T-cell infusion of 7.2 months. Importantly, the efficacy of the treatment was lower in the older subgroup (age ≥75), with 12-month EFS estimates of 34% compared to 43% and 52% in patients aged 65−69 years and 70−74 years, respectively (p=0.002). The median OS was 17.1 months, with no significant difference between the older and younger arms.
The GLA/DRST study
A multicenter retrospective RWE study performed in Germany confirmed the benefits of CAR T-cell products in older patients and demonstrated that the therapy outcome improved with increasing age.45,46 The study was performed under the auspices of the Working Group Hematopoietic Cell Therapy of the German Lymphoma Alliance (GLA) using the data collected by the German Registry for Stem Cell Transplantation (Deutsches Register für Stammzelltransplantation, DRST).45 The population included 356 patients (aged ≥18 years) who were enlisted at the DRST and received treatment with either axi-cel (n=173) or tisa-cel (n=183) for LBCL between November 2018 and April 2021 at 21 German centers. The main endpoints were ORR, CR, OS, PFS, non-relapse mortality (NRM), toxicities, as well as the impact of bridging therapies on the clinical outcome. The median age was 60 years; 39.3% of patients were aged ≥65 years. In the overall population, 71% of patients had received ≥3 treatment lines (including 20% with ≥5 treatment lines) before the start of bridging therapy or lymphodepletion. Prior autologous (n=108) or allogeneic (n=13) HSCT had been performed in 34% of the patients; 76% had disease refractory to chemotherapy.
A follow-up analysis of the study focused on comparing subgroups of patients aged <65 years and ≥65 years.46 With a median follow-up of 11 months, patients aged ≥65 years exhibited superior response rates versus the younger group, with ORR of 69% versus 58% and CR rate of 43% versus 31%, respectively. The response benefits in older patients were observed for both CAR T-cell products but were more pronounced with axi-cel. The ORR was 89% and 70% in older and younger patients, respectively, for axi-cel (p=0.0073) versus 61% and 50% for tisa-cel (p=0.16). CR rates were 56% and 35% with axi-cel (p=0.0094) versus 37% and 29% with tisa-cel (p=0.33) in patients aged ≥65 years and <65 years, respectively. Accordingly, higher response rates in the older group translated into significantly better 12-month PFS rates (36% versus 26% for patients aged ≥65 years versus <65 years, respectively), with PFS benefits being more pronounced with axi-cel (Figure 3A, B). The OS of patients was not significantly different between the products (Figure 3C).
_t-cell_therapies_in_older_patients_treated_wit.jpg)
In terms of toxicity, the incidence of high-grade CRS was similar in older and younger patients. However, the ≥65-year-old group showed a tendency towards a higher incidence of high-grade neurotoxicity AEs and non-relapse mortality (NRM, 9% vs 3% in patients <65 years; HR: 2.25 [95% CI: 0.93–5.43]), with infections being the main cause of NRM in both age groups. Tisa-cel was associated with a lower incidence of overall (but not high-grade) CRS, overall and high-grade ICANS and 12-month NRM (3.5% vs 10.4% for axi-cel). Yet, it was noted that a relatively short median follow-up time, as well as the differences in clinical practice such as patient selection, performance status and toxicity management, may lead to a bias in the interpretation of the OS and NRM data.
Importantly, the study identified the absence of response to bridging therapy rather than its use as a predictor of negative treatment outcome, suggesting that the lesser impact of bridging in the ≥65-year-old group is due to a poor 12-month PFS rate (16%) of younger patients who did not respond to bridging therapy.46
Improvements in CAR T-cell therapy outcomes over time: the UK RWE study
CAR T-cell therapy outcomes may depend on a variety of factors such as patient selection or toxicity management and may change over time due to the novel data prompting changes in treatment protocols and enrollment criteria, as well as improved experience of oncologists and caregivers. A recent study aimed to assess how clinical outcomes of CAR T-cell therapy developed over time in the UK.47
The study enrolled 726 patients with relapsed or refractory LBCL after ≥3 prior treatment lines who were approved for treatment with axi-cel or tisa-cel between December 2018 and June 2022 across 12 UK centers.47 Based on the time of approval, the patients were divided into two subgroups: Era 1 (December 2018-2019, n=236) and Era 2 (January 2020-June 2022, n=490). Patients in Era 2 were older compared with those in Era 1 (median age 62 vs 58 years, respectively, p<0.001). The Era 2 subgroup was also less likely to be considered for HSCT and had a higher International Prognostic Index (IPI) score at the time of diagnosis. The majority of patients received axi-cel (83% vs 71% in Era 2 vs Era 1), while tisa-cel was given mainly to older patients (36% in patients aged >65 years compared with 15% in the younger subgroup), with the difference becoming more pronounced over time (9% vs 27% of patients aged ≤65 years in Era 2 vs Era 1). The median follow-up was 22.3 months.
Overall, the study demonstrated favorable survival outcomes and a significant improvement in efficacy over time.47 The probability of receiving CAR T-cell therapy was higher in Era 2 (83%) compared with Era 1 (73%). Significant changes in the bridging therapy were observed, with increased use of polatuzumab vedotin-based bridging and fewer bridging failures in Era 2. The best ORR of 80% (including CR rates of 63%) versus 67% (including 42% of CRs) were reported for Era 2 versus Era 1, respectively. At 1 year, PFS was 50% versus 32% and OS was 60% versus 40% in the Era 2 versus Era 1 subgroups. Importantly, PFS was also specifically improved in the cohort of patients aged >70 years (49% vs 17% for Era 2 vs Era 1). PFS benefits were observed for both CAR T-cell products, with axi-cel therapy being associated with better PFS outcomes: 1-year PFS was 51% versus 35% with axi-cel and 41% versus 24% with tisa-cel in Era 2 versus Era 1, respectively.
The incidence of grade ≥3 ICANS was higher for axi-cel versus tisa-cel (18% vs 5%, p<0.001), but high-grade CRS rates were similar for the two products (6% vs 6%, p=0.83).47 No reduction in ICANS rates was observed over time in either cohort, while high-grade CRS reduced over time for all patients (grade ≥3, 4% in Era 2 vs 9% in Era 1, p=0.01) and patients treated with axi-cel in particular (grade ≥3, 4% in Era 2 vs 10% in Era 1, p=0.012). Since no differences in patient selection criteria were reported for the Era 1 and Era 2 subgroups, bridging therapy protocols and better toxicity management were identified as the main drivers of improvements in CAR T-cell therapy outcomes. There was higher utilization of tocilizumab (76% vs 61%, p=0.002) and corticosteroids (46% vs 34%, p=0.03) in Era 2 versus Era 1 due to earlier initiation of treatment: the use of tocilizumab for grade 1 CRS was 59% versus 21% and the use of corticosteroids for grade 1 ICANS was 61% versus 17% in Era 2 versus Era 1.
PILOT
The open-label phase II PILOT study evaluated the efficacy and safety of liso-cel in patients with relapsed/refractory LBCL after 1 prior line of therapy who were not intended for HSCT.50 The analysis included 61 infused patients (median age 74 years) who received liso-cel, among them 46% aged ≥75 years. Overall, 33% of patients had double- or triple-hit disease and 54% had refractory disease. At a median follow-up of 18.2 months,48 the study met its primary endpoint with an ORR of 80.3% including 54.1% CRs. The 18-month PFS and OS rates were 42.9% and 59.0%, respectively.48,51 With respect to toxicity, 37.7% of patients developed CRS (grade 3, 1.6%; no grade 4–5) and 31.1% had neurological events (grade 3, 4.9%; no grade 4–5). Given relatively low overall rates of AEs including ICANS, liso-cel may represent an attractive treatment option for older patients.
Open questions and future directions
While recent studies clearly demonstrate substantial clinical benefits of CAR T-cells in older patients with DLBCL, there are many open questions which remain to be addressed. It is still not entirely clear why the increased efficacy of CAR T-cell treatments is often reported in the older population as compared with younger subgroups. As there is no evidence that older patients have less aggressive disease or a better T-cell function, it was hypothesized that the difference in outcomes may be explained by patient selection.46 The superior therapy effects in the older population remained stable after multivariable adjustment for confounders; however, additional confounding risk factors may exist that are not considered in the multivariate analyses. Furthermore, the shorter interval between diagnosis and treatment in the younger cohort suggested that a larger fraction of patients exhibited primary and early treatment failure, leading to the unfavorable selection in the study population.46 Therefore, the efficacy of CAR T-cell treatments in older patients might be comparable to that in the overall population; however, more studies are needed to unequivocally establish the outcomes of CAR T-cell therapy in different age groups.
Another important question pertains to patient selection and eligibility criteria for therapy. Apart from age, many other factors including the type of disease, the course of disease progression, performance status and organ function of patients and the presence of comorbidities may also contribute to the overall outcome of therapy. The current recommendations of the European Society of Blood and Marrow Transplantation (EBMT) and the European Hematology Association (EHA)52 provide only general guidance, and their applicability to specific individual cases remains limited in scope. Older patients may be considered eligible for CAR T-cell therapy but not for HSCT; however, recent studies demonstrate that CAR T-cell treatment can be safely performed in carefully selected older patients and patients with comorbidities who are not considered fit for autologous HSCT.53,54 On the other hand, CAR T-cell therapy is associated with a higher risk of severe toxicities, such as CRS and ICANS.37,55 Together, this indicates the need to identify clear risk factors and for novel strategies to evaluate patients with respect to potential severe CAR T-cell-specific toxicities and to determine which interventions may help to improve therapy outcomes in the older population, including transplant-ineligible patients. Bispecific antibodies,56 a novel class of off-the-shelf T-cell redirecting drugs, which demonstrate promising anti-tumor activity and less toxicity, are further complicating decision making, in particular in older patients.
The Comprehensive Geriatric Assessment (CGA), an interdisciplinary diagnostic process aimed at evaluating the medical, psychological and functional capability of a frail older person, is recognized as an essential step during decision-making process that helps to develop a coordinated plan for treatment. The current guidelines recommend performing a CGA for older adults with cancer to provide appropriate care when considering systemic therapy.57 While these recommendations were formulated mostly for patients receiving chemotherapy-based regimens, the experts advise extending them to any systemic therapy including cell-based treatments, based on early evidence of benefits.57 Another important aspect to be considered while making treatment decisions involves QoL, which is especially relevant in the case of older frail patients. Despite emerging data on PROs (see for instance the analysis of ZUMA-743 mentioned above) which will be considered by regulatory agencies during the evaluation of new applications, there is still a lack of studies focusing on health-related QoL in older patients with relapsed and refractory LBCL.
Conclusions
CAR T-cell therapy offers an effective solution for older patients with DLBCL, who otherwise face limited treatment alternatives, and should therefore be considered and provided to this specific patient population. While treatment-emerging AEs remain a concern, the overall safety profile of CAR T-cell products appears to be manageable and will likely improve with time. These promising results indicate that age alone should not be a limiting factor in the application of CAR T-cell therapy, which may prove beneficial even for more fragile patients. On the other hand, the potential risk of severe toxicities associated with CAR T-cell therapies, together with emerging novel efficient and less toxic drugs, such as bispecific antibodies, suggests the need for clear identification of risk factors to determine the optimal treatment strategy in older patients with cancer.
Conflict of interest
Frank Stenner serves on advisory boards for Roche, Novartis, Bristol-Myers Squibb and Gilead Sciences. Felicitas Hitz serves on advisory boards for Bristol-Myers Squibb, AbbVie and Takeda. These companies did not play a role in the development of the manuscript and did not influence its content in any way.
Funding
The authors have declared that no financial support was received from any organization for the submitted work.
Author contributions
Both authors contributed to and approved the final manuscript.