Surgery for prostate cancer: approaches and limitations
Prostate cancer is the leading form of cancer among males, impacting around 28% of the male population, with the likelihood of developing this disease increasing significantly after the age of 60.1 The incidence of prostate cancer has been greatly influenced by the global growth of the aging population. With longer life expectancy, the prevalence of prostate cancer has surged worldwide, resulting in an annual rise in diagnosed cases. In Switzerland, approximately 20% of the population is aged 65 or above. This aging population poses challenges for healthcare systems in terms of providing adequate screening, diagnosis, and treatment options for prostate cancer.
Radical prostatectomy is a commonly recommended treatment for localized prostate cancer.2 The procedure can be performed using traditional open surgery or minimally invasive techniques like laparoscopy/robotics. Minimal invasive surgery is widely utilized in clinical practice due to its numerous patient benefits, including reduced blood loss, shorter hospital stays, faster recovery times, and potentially less postoperative pain. However, the choice between open and minimal invasive surgery for prostate cancer treatment is a subject of debate among healthcare professionals. One of the limitations that can impede the implementation of laparoscopy/robotics into clinical practice is the experience and training of surgeons. The learning curve for laparoscopic techniques can be steep, and it may require significant time for surgeons to become proficient in this approach.
Current challenges in education of urology residents
Several recent studies revealed a concerningly low level of basic laparoscopic skills among urology residents. The results of the European Basic Laparoscopic Urological Skills (E-BLUS) examination3 demonstrate that, while the quality of performance is generally good, most residents do not meet the validated time criteria set by the E-BLUS examination. Overall, 65% of the participants did not have access to a skills lab in their hospital, 61% lacked opportunities for laparoscopic training, and 61% admitted to not receiving basic laparoscopic skills training in the four weeks preceding the examination. Low surgical exposure of European residents to major procedures was associated with overall poor satisfaction with surgical training and low professional confidence.4 Current US graduates of urology residency programs also express a perceived lack of confidence in major procedures that are commonly encountered in general urologic practice; accordingly, almost three-fourths of US graduates are now pursuing postgraduate fellowship training.5 A study on training and working conditions of urological doctors in further training in Germany show that for 45% of respondents, interventions are certified without having performed them. Only 28% carry out all the interventions required by the Further Education Regulations (Weiterbildungsordnung, WBO) themselves, and 27% do not completely fulfill the catalog of operations. 64% of the participants surveyed are dissatisfied with the type and frequency of their operational assignments.6
There is an urgent need to enhance the laparoscopic proficiency of urology residents. The recommended measures include the establishment of a standardized curriculum with specific requirements for teaching and structured surgical exposure across Europe; a thorough assessment of the timing and setting of the examinations to determine their suitability and effectiveness; and the launch of a regular laparoscopic training program/fellowship in laparoscopy. Various methods and modules should be implemented in the program including procedure observation, mentorship and fellowship programs, e-learning, and simulation-based training.3–7
Innovative technologies in prostate cancer surgery
The preference for endoscopic “keyhole” or minimally invasive procedures over open surgeries, even when performed by highly qualified specialists, remains a subject of debate. Minimally invasive interventions are deemed superior by many clinicians and proposed as the first-line surgical treatment for various conditions, including laparoscopic radical prostatectomy for localized prostate cancer.8 However, the supporting data from retrospective studies are limited, and the level of criticism is growing louder. Conflicting evidence has been reported regarding the benefits of minimally invasive procedures, among them robot-assisted approaches, in prostate cancer treatment.9,10
Robot-assisted minimally invasive surgery is one of the rapidly evolving innovative clinical techniques. Robotic operations using the da Vinci Surgical System have gained widespread acceptance and are now being implemented in many clinics in Switzerland. This advanced technology provides surgeons with enhanced precision, dexterity, and visualization during the intervention and therefore holds a significant promise across a spectrum of surgical procedures, encompassing prostatectomy, hysterectomy, cardiac valve repair, and colorectal surgery. Yet, the first randomized controlled study that compared oncological, functional, and surgical outcomes of robot-assisted laparoscopic prostatectomy (RALP) versus open radical retropubic prostatectomy (ORP) yielded similar functional outcomes at 24 months.11 In another study involving highly trained surgeons for both procedures no statistically significant difference regarding oncological outcome between ORP versus RALP was demonstrated.12 A modest advantage for RALP for surgical outcomes such as blood loss, transfusion rates and time to catheter removal was observed, most likely attributable to its minimally invasive nature and better educational capabilities. These data indicate that a well-trained surgeon remains the most important factor in achieving favorable results. Accordingly, current Guidelines of the European Association of Urology (EAU)13 state that no active treatment modality (open, laparoscopic or robot-assisted surgery) has shown superiority in terms of overall- and prostate cancer-specific survival for clinically localized low/intermediate-risk disease. On the other hand, recent studies show that laparoscopic approaches may provide benefits to patients in terms of both oncological outcomes and quality of life. In a long-term follow-up study, prostate cancer–specific mortality was significantly lower in the RALP group at 8 years after surgery, with differences being mainly seen in high-risk patients.14 Furthermore, while urinary incontinence rates at 8 years were not different between RALP and ORP patients, the rate of erectile dysfunction tended to be lower with RALP, although not all differences reached statistical significance.14 Another study showed that RALP patients had less pain, shorter hospital stays and fewer post-surgical complications including deep venous thromboses and bladder neck contractures,15 thus supporting the continued use of robot-assisted surgery in prostate cancer.
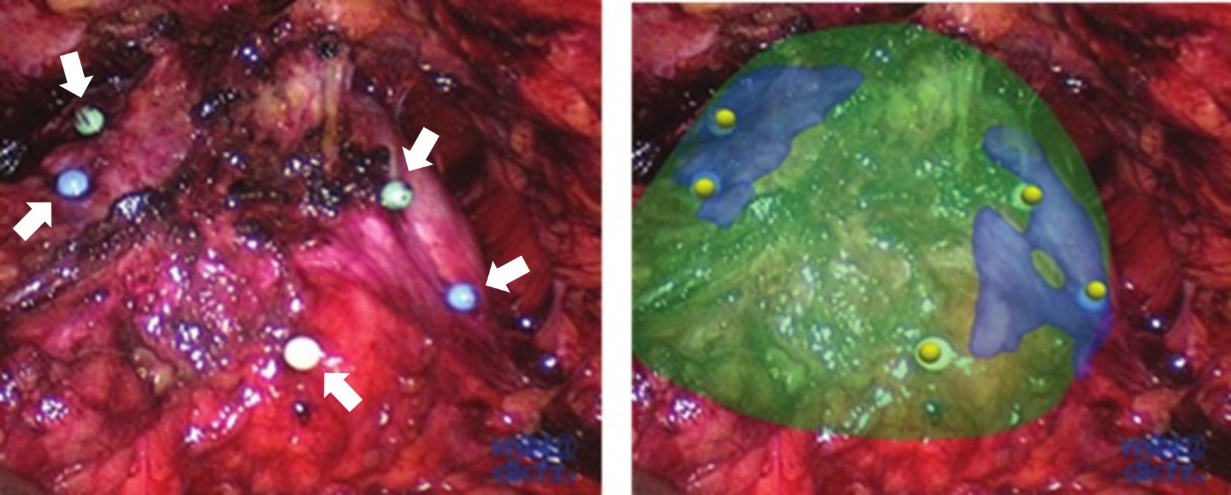
Augmented reality (AR) visualization is an emerging technology that has shown potential in various surgical specialties, including laparoscopic radical prostatectomy (Figure 1). It involves overlaying computer-generated images or information onto the surgeon’s view of the actual patient’s anatomy during the procedure. This helps to enhance visualization of critical structures, determine precise tumor localization, and track laparoscopic instruments, ultimately supporting surgeons in their working decisions, improving the precision and reducing the risk of inadvertent damage to surrounding structures. The first in-vivo human application of the AR navigation system that conveys virtual organ models generated from transrectal ultrasonography (TRUS) onto a real laparoscopic video has shown its technical feasibility and fundamental feasibility for radical prostatectomy.16 The system supported the surgeons as intended with an AR visualization in real time, and no complications occurred. Nonetheless, results obtained from a larger number of trials are needed to unequivocally demonstrate the benefit of the approach for the patient.
_visualization_during_laparoscopic_radical_prostatectomy.jpeg)
High-Intensity Focused Ultrasound (HIFU) and NanoKnife are among other innovative focal treatments for prostate cancer that offer less invasive alternatives to traditional surgical methods. HIFU utilizes precisely targeted ultrasound energy to destroy cancerous tissue within the prostate, effectively treating the disease while minimizing damage to surrounding healthy tissue.17 Clinical trials demonstrate that focal HIFU achieves excellent functional outcomes, is associated with a low risk of complications and can help preserve quality of life.18,19 NanoKnife, on the other hand, employs a minimally invasive approach involving the use of non-thermal irreversible electroporation to permanently damage tumor cell membrane.20 Both HIFU and NanoKnife, as well as other focal treatment approaches, have gained attention for their potential to reduce the side effects commonly associated with more aggressive prostate cancer treatments, such as surgery and radiation therapy.21
Last but not least, among the notable and innovative approaches to surgical management of prostate cancer is artificial intelligence (AI), computational models and algorithms that enable computers to simulate human cognitive processes, such as perception, understanding, problem-solving, and learning. AI has the potential to revolutionize healthcare by assisting with the analysis of medical images and real-time imaging data during surgery, making diagnostic and prognostic decisions based on medical records and research literature, guiding robot-assisted surgeries, and much more. However, does it make doctors obsolete? AI is already changing the labor market across industries and occupations worldwide; there are fears that it may lead to job displacement and create economic inequalities in certain industries. In a recent study, the effects of future computerization on labor market outcomes were explored for 702 occupations based on the task requirements related to creative intelligence, social intelligence, and fine perception and manipulation.22 Surgeons were demonstrated to be among the occupations with the lowest susceptibility to computerization, suggesting that AI is more suitable for repetitive and error-prone tasks and is not capable of replicating the full range of skills and expertise possessed by qualified specialists. Ultimately, the future of surgery is likely to involve a collaborative approach, where AI and human surgeons work together to achieve the best outcomes for patients.
Conclusions
-
There is an urgent need to enhance the laparoscopic proficiency of urology residents in Europe. This necessitates the improvement of educational methods in order to equip future urologists with the required skills and expertise in laparoscopic procedures.
-
The use of minimally invasive procedures in surgery is a topic of debate. Robot-assisted surgery, HIFU, NanoKnife, AR visualization and AI are emerging innovative technologies that show potential in surgical procedures, but more research is needed to determine their benefits. Despite advancements in technology, human surgeons are still irreplaceable, and a collaborative approach between AI and surgeons is likely to be the future of medicine.
Conflict of interest
Author has declared that the manuscript was written in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author has declared that no financial support was received from any organization for the submitted work.
Author contributions
The author has created and approved the final manuscript.