Introduction
A decade after the SHARP trial established the multikinase inhibitor sorafenib as a systemic therapy for patients with hepatocellular carcinoma (HCC) in Barcelona Clinic Liver Cancer (BCLC) stage C,1 the REFLECT trial showed the non-inferiority of lenvatinib, another multikinase inhibitor, to sorafenib in this patient population in 2018.2 Since then, five systemic treatments have demonstrated efficacy in phase III clinical trials: regorafenib as a second-line therapy, cabozantinib as a second- and third-line therapy, ramucirumab for patients with alpha-fetoprotein (AFP) above 400 ng/ml and, more recently, two immuno-oncology combinations, atezolizumab plus bevacizumab and tremelimumab plus durvalumab, both in the first-line setting. All these therapies are approved in Switzerland for the treatment of patients with unresectable HCC. This progress in available therapeutic options may present challenges for physicians treating patients with HCC.
Transitioning HCC patients in BCLC stage B to systemic therapies
According to the current ESMO guidelines, HCC patients in BCLC stage C are suitable for systemic therapies.3 Eligible patients in BCLC stage B are commonly treated with local therapies, such as transarterial chemoembolization (TACE). However, if the tumor burden exceeds the capacity of local treatments, this patient group should be considered for systemic therapies. TACE is frequently overused in patients with HCC BCLC stage B,4 which can result in liver function deterioration.5 There is a well-known heterogeneity in the BCLC stage B and substages have been proposed to better reflect the variability.6 Masatoshi Kudo (2018) conceptualized the limits of TACE in terms of tumor burden, suggesting that TACE is not indicated for patients with more than 7 lesions or lesions larger than 6 cm.7 These patients should be evaluated for systemic therapies and recent studies highlighted lenvatinib as a promising alternative to TACE.
In a Japanese real-world retrospective study, 171 patients refractory to TACE were treated with either lenvatinib, sorafenib or TACE.8 Notably, those receiving lenvatinib had significantly longer progression-free survival (PFS) than those continuing with TACE (median, 5.8 months vs 2.8 months; HR: 0.23 [95% CI: 0.15−0.36]; p<0.001). Similar results were reported from a proof-of-concept study on 642 consecutive patients with HCC beyond the up-to-seven criteria who were initially treated with lenvatinib or conventional TACE.9 The lenvatinib group versus the TACE group demonstrated significantly prolonged both overall survival (OS) (median, 37.9 months vs 21.3 months; HR: 0.48 [95% CI: 0.16−0.79]; p<0.01) and PFS (16.0 months vs 3.0 months; HR: 0.19 [95% CI: 0.10−0.35]; p<0.001). Notably, in the phase III REFLECT trial, patients in HCC BCLC stage B versus BCLC stage C had improved clinical outcomes, including OS, PFS and objective response rate (ORR), irrespective of therapy received (lenvatinib or sorafenib).2
Promising results were also reported with immune checkpoint inhibitors (ICIs),10,11 which have raised the possibility of achieving complete response and curative conversion in patients with unresectable HCC.12 According to the 2022 update of BCLC strategy for prognosis prediction and treatment recommendation, patients with BCLC stage B with extensive bilobar liver involvement should be considered for systemic therapy, including durvalumab plus tremelimumab and atezolizumab plus bevacizumab in the first-line setting to avoid liver function deterioration associated with TACE and ensure access to more effective systemic treatments.13
Immunotherapy for patients with advanced HCC
The combination of atezolizumab, an ICI that targets programmed cell death ligand 1 (PD-L1), and bevacizumab, a monoclonal antibody against vascular endothelial growth factor (VEGF), is currently indicated for the treatment of patients with unresectable or metastatic HCC who have not received prior systemic therapy.14 In the IMbrave150 study, treatment with atezolizumab plus bevacizumab led to significantly prolonged OS, with a median OS of 19.2 months versus 13.4 with sorafenib in the updated analysis at a median follow-up of 15.6 months (HR: 0.66 [95% CI: 0.52−0.85]; descriptive p<0.001).11,15 This combination also offers a better quality of life (QoL) to patients than sorafenib, a treatment that is often associated with fatigue and gastrointestinal side effects.
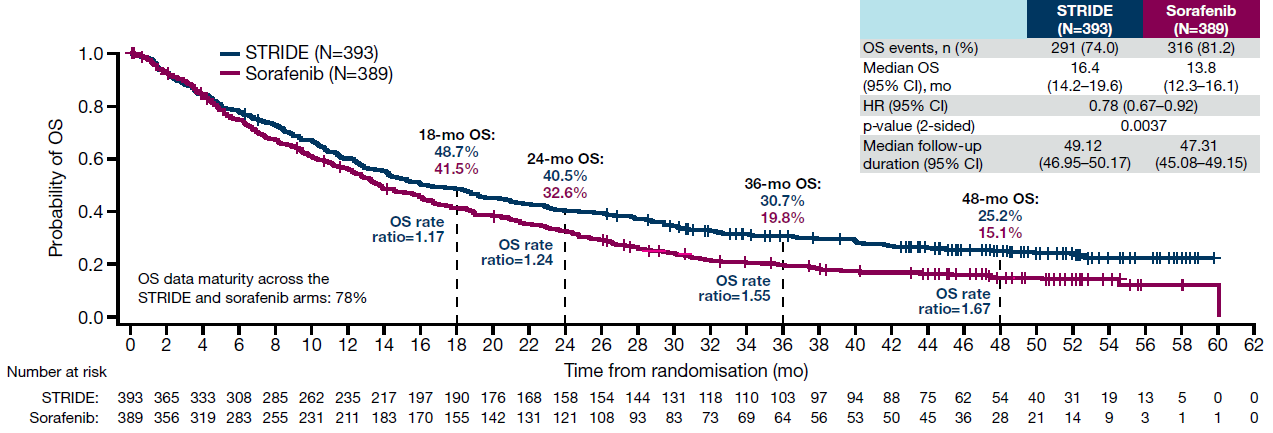
The anti-CTLA-4 antibody tremelimumab in combination with the anti-PD-L1 antibody durvalumab is another promising first-line therapeutic option that is authorized in Switzerland for the treatment of patients with unresectable HCC.16 The approval was based on findings from the phase III HIMALAYA trial demonstrating that the STRIDE (single tremelimumab regular interval durvalumab) regimen significantly improved the median OS versus sorafenib (16.43 months vs 13.77 months; HR: 0.78 [96.02% CI: 0.65−0.93]; p=0.0035) (Figure 1).10 Consistent with the primary analysis, the 4-year follow-up showed the OS hazard ratio of 0.78 (95% CI: 0.67−0.92), with an estimated 36-month OS rate of 30.7% and 48-month OS rate of 25.2% with STRIDE.17 No significant PFS difference was observed between the two treatment arms.10 In terms of safety, the STRIDE regimen was not associated with meaningful liver toxicity and demonstrated no treatment-related gastrointestinal or esophageal varices hemorrhage events. Results from an analysis assessing patient-reported outcomes (PROs) further showed that treatment with STRIDE delayed worsening of patient-reported QoL, functioning and disease-related symptoms.18
_for_stride_versus_sorafenib_in_the_4-year_updated_analysis_of_hi.png)
While rarely seen with sorafenib, immuno-oncology can induce tumor regression or disappearance, which can potentially lead to downstaging and liver transplantation.19,20 However, immuno-oncology is associated with a multitude of immune-mediated side effects, also severe ones, and is contraindicated in patients with immunological conditions such as auto-immune diseases and transplantation. Furthermore, the required eradication of varices prior to frontline bevacizumab to avoid bleeding events can delay the treatment. As a result, alternative immuno-oncology therapy with tremelimumab plus durvalumab (STRIDE) may be favored in such situations.
Other therapeutic options demonstrating efficacy in phase III trials are sintilimab plus bevacizumab (ORIENT-32 trial),21 tislelizumab (RATIONALE 301 trial)22 and camrelizumab plus rivoceranib (SHR-1210-III-310 trial).23 These regimens have not yet been approved in Switzerland. A recently published press release on positive high-level results from the EMERALD-1 phase III trial reports a statistically significant and clinically meaningful improvement in PFS with durvalumab in combination with transarterial chemoembolization (TACE) and bevacizumab versus TACE alone in patients with HCC eligible for embolization.24
Predictive biomarkers of response
The lack of predictive markers represents a major limitation in selecting the optimal treatment for patients with HCC and tools to personalized systemic treatment of patients with HCC are urgently needed. A simple score incorporating serum levels of AFP and the C-reactive protein (CRP) (CRAFITY) can help in identifying HCC patients with a favorable response to ICIs.25 Data further show that the occurrence of immune-related adverse events is a potential prognostic biomarker for response to ICIs, with patients with more severe events having a better prognosis.26 Additionally, the elevated levels of antibodies against atezolizumab are associated with reduced response rates and worse survival outcomes with atezolizumab plus bevacizumab in patients with HCC.27 However, their determination is not performed in clinical practice.
The underlying etiology of HCC might also influence response to treatment. In a remarkable publication, Heikenwälder et al. (2021) presented data showing that anti-programmed cell death protein 1 (PD-1) therapy for HCC is less efficacious in the presence of fatty liver disease compared with chronic viral infection in a mouse model.28 This effect was observed in a meta-analysis of three phase III trials assessing immuno-oncology for the treatment of HCC, including IMbrave150,11 CheckMate 45929 and KEYNOTE-240.30 More specifically, immunotherapy significantly improved survival versus the control treatment in patients with hepatitis B virus (HBV)- and hepatitis C virus (HCV)-related HCC (p=0.0008 and p=0.04), but not in patients with non-viral HCC (p=0.39). However, this trend was not seen with the combination of tremelimumab and durvalumab in a subgroup analysis of the HIMALAYA study, showing favorable OS outcomes with STRIDE versus sorafenib, regardless of etiology.10,31
In the absence of reliable predictive markers for personalized treatment, the response can be evaluated only after a few months of treatment initiation. Following frontline treatment with tremelimumab plus durvalumab or atezolizumab plus bevacizumab in eligible patients, subsequent lines of therapy may include sorafenib, lenvatinib, regorafenib, cabozantinib, or ramucirumab in patients with AFP ≥400 ng/ml.3,13,32 Of note, OS in the sorafenib group in the IMbrave150 trial11 was exceptional reaching 18.1 months (vs 17.0 months in the atezolizumab/bevacizumab group). The feasibility of reintroducing immuno-oncology after kinase inhibitor therapy can be considered.25
Effective sequential therapy strategies require well-managed underlying liver disease in patients with advanced HCC. Studies showed that preserved liver function, as assessed by the albumin-bilirubin (ALBI) score, is linked to prolonged survival and enables therapeutic sequencing.33 The control of chronic hepatitis B with nucleoside/nucleotide analogs is thus essential. While there is no indication to treat chronic hepatitis C in patients with HCC, eradication may be considered in case of remission. Complications of cirrhosis, particularly portal hypertension, should be prevented with the beta blocker carvedilol, implying multidisciplinary care involving liver specialists.
Conclusion
The treatment landscape of HCC has evolved significantly over the past 15 years. After establishing sorafenib as the standard systemic therapy for patients with advanced HCC in 2008, several other therapies have shown efficacy and safety in phase III clinical trials. These include kinase inhibitors lenvatinib, regorafenib and cabozantinib, as well as the monoclonal antibody ramucirumab and two immuno-oncology combinations atezolizumab plus bevacizumab and tremelimumab plus durvalumab, which are all approved in Switzerland for this indication. While the local therapy TACE is commonly used in patients with HCC BCLC stage B, its efficacy is limited with tumor burden and some patients may benefit from systemic therapies. Treatment with ICIs has also yielded encouraging results in this subgroup of HCC patients, potentially achieving complete responses and curative conversions. Personalized treatment remains challenging due to the lack of predictive markers, but data showed that the CRAFITY score incorporating AFP and CRP can predict response to ICIs. Other potential indicators of response include artificial intelligence-based pathology tumor assessment34 and the underlying etiology of HCC, with some evidence suggesting that immunotherapy is less effective in non-viral HCC.
Conflicts of interest
The author has declared the following competing interests. Advisory committees: Alentis, AstraZeneca, Bayer, Bristol-Myers Squibb, Enyo, Esai, Genfit, Intercept, Inventiva, Ipsen, Lilly, Madrigal, Merck, Novartis, Novo-Nordisk, Roche. Speaking and teaching: AstraZeneca, Bristol-Myers Squibb, ESAI, Intercept, Ipsen, Roche.
Funding
Preparation of this article was financially supported by AstraZeneca AG. AstraZeneca did not have any decision-making role in the development of the manuscript and did not influence its content in any way.
Author contributions
The author has created and approved the final manuscript.