Introduction
Endometrial cancer is the most common gynecologic malignancy in developed countries and the fifth leading cause of death among cancer patients worldwide.1 It affects mainly postmenopausal women, with most cases occurring between 65 and 75 years and a median age of onset of 69 years. In Europe, endometrial cancer ranks as the fourth highest among all cancers in women and has an incidence of 12.9−20.2 per 100,000.2,3 The mortality rate is low at 2.0−2.7 per 100,000, mainly due to early detection because of notable early symptoms such as irregular vaginal bleeding. In Switzerland, an estimated 950 new cases and 200 deaths due to endometrial cancer are reported every year.4 Most endometrial cancer cases are sporadic, with around 10% considered hereditary.5
The majority of endometrial cancers present at an early stage and are successfully treated with surgery alone. While early-stage endometrial cancer has an excellent prognosis, advanced and recurrent disease is associated with poor survival outcomes. More specifically, 5-year overall survival (OS) rate is more than 80% for patients with stage I endometrial cancer, which is diagnosed in nearly 70% of cases.6–8 Among those with stage IV disease (around 16% of patients at diagnosis), the estimated 5-year OS rate is below 17%. Notably, mortality rates among patients with endometrial cancer have increased on average by 1.9% per year from 1971 to 2014, which is associated with increased incidence of obesity.9
Approximately 2−5% of all cases of endometrial cancer are thought to be due to Lynch syndrome, also referred to as hereditary nonpolyposis colorectal cancer (HNPCC) syndrome, an autosomal-dominant inherited cancer susceptibility syndrome.10 Lynch syndrome is linked to germline mutation in one of the DNA mismatch repair (MMR) genes (MLH1, MSH2, MSH6 and PMS2) or deletion of the stop codon of EPCAM. Impaired MMR leads to the accumulation of DNA replication errors at microsatellite regions, also known as microsatellite instability (MSI), which is a molecular abnormality associated with the development of many cancers. Depending on the mutated gene, the lifetime cumulative risk of endometrial cancer is between 27% and 70% for women with Lynch syndrome.
Known risk factors for the development of endometrial cancer include obesity, diabetes, polycystic ovary syndrome and hypertension.5,11 Obesity is the strongest risk factor for endometrial cancer in Europe and the United States, with more than 50% of cases attributable to increased body mass index (BMI).12 Data showed that women with a normal BMI have a 3% lifetime risk for endometrial cancer, but each 5 kg/m2 increase in the BMI was associated with more than 50% increase in the risk for the disease.13 Obesity (BMI ≥40) is associated with a 6.25-fold increased risk of death.14 Another important risk factor for endometrial cancer is exposure to tamoxifen. Studies showed that tamoxifen doubles the risk for endometrial cancer, with up to four times the risk with longer tamoxifen treatment (≥5 years).15,16 Protective factors against endometrial cancer are parity and oral contraceptive use.17 Oral contraceptives reduce the risk of endometrial cancer by 30−40%. Longer use of oral contraceptives is associated with reduced risk for endometrial cancer, with risk reduction persisting for more than three decades after cessation.
Survival outcomes are dismal for patients with advanced/recurrent disease, with 5-year OS rates of 20−25%.5 Standard of care systemic therapy for unresectable recurrent/metastatic disease in the frontline setting is typically a platinum-based chemotherapy regimen such as carboplatin plus paclitaxel. However, data from the phase III GOG-209 study showed that response rates with chemotherapy are only around 50%, with a median progression-free survival (PFS) and OS of 13 months and 37 months, respectively.18 Treatment options with chemotherapy beyond the first line are limited with no standard of care identified.5 In an advanced setting, therapy with immune checkpoint inhibitors (ICIs), both alone and in combination with chemotherapy or targeted agents, has been explored, with promising results reported from clinical trials. These studies are described in detail below.
Molecular classification
Based on The Cancer Genome Atlas (TCGA), endometrial cancers are classified into four distinct molecular groups: DNA polymerase epsilon (POLE)-ultramutated (>100 mutations/megabase [mut/Mb]), MSI hypermutated (MSI-H) (10−100 mut/Mb; deficiency in MMR responsible for this phenotype), somatic copy-number high (with frequent pathogenic variants in TP53) and copy-number low (frequent abnormalities in phosphoinositide 3-kinase [PI3K] and WNT signaling pathways; also defined as microsatellite stability [MSS]).19 Each of these distinct molecular subtypes is associated with different prognostic significance, with POLE-ultramutated having an excellent prognosis and MSI-H and copy-number low having intermediate and stage-dependent prognosis, while endometrial tumors harboring TP53 abnormalities are associated with poor prognosis.
Each molecular subgroup is also characterized by different histological and clinical features.8,20
Treatment options for advanced and refractory endometrial cancer
Tumors with dMMR/MSI have been identified in approximately 30% of patients with primary endometrial cancer and 13−30% of patients with recurrent endometrial cancer.19,21 Around 90% of dMMR tumors are of endometrioid histological type.22,23 They present specific characteristics, including significant intra-tumor lymphocytic infiltrate, the presence of undifferentiated and low-grade tumor contingents and increased frequency of lymph vascular space invasion.22–24 A meta-analysis also showed that lymph node involvement (stage IIIC) is more common in dMMR than low-copy number tumors (10% vs >5%).23 dMMR tumors are associated with other poor prognostic factors such as high grade, high FIGO stage and increased risk for relapse compared with low-copy number tumors.22
The dMMR/MSI-H subtype is considered highly immunogenic with overexpressed immune-related biomarkers. In detail, endometrial cancer cells can modulate the inherent immune response by activating programmed cell death protein 1 (PD-1) signaling pathway, an immune checkpoint and a significant target for cancer immunotherapy, via overexpression of programmed death-ligand (PD-L) 1 and PD-L2. PD-L1 and PD-L2 are ligands for the PD-1 receptor which is expressed on activated CD4+ and CD8+ tumor-infiltrating lymphocytes (TILs).25 Upon binding of these ligands to PD-1, the T cells are inactivated in the tumor environment and undergo apoptosis. This pathway is one of the main targets of anti-PD-1/PD-L1 immunotherapy which yields high response rates in PD-L1-positive tumors.26 In general, immune checkpoints and their ligands are highly expressed in endometrial cancer, but their expression levels vary according to tumor grade, histology or mutation status. PD-1 and PD-L1 expression levels range from 40% to 80% in endometrioid, 23% to 69% in clear cell and 10% to 68% in serous subtypes, respectively, which is the highest level among gynecologic cancers. When stratified by molecular subtypes, PD-L1 expression is increased in POLE-ultramutated and MSI-H tumors compared with MSS tumors.27,28 These two subtypes are also associated with high neoantigen loads and an increased number of CD3+ and CD8+ TILs, resulting in upregulation of the PD-1/PD-L1 pathway.27,29 Notably, the presence of TILs is an independent prognostic factor associated with favorable tumor prognosis and responses to therapy.30
Given the described immune dysregulation in endometrial cancer, immunotherapy based on ICIs, both as monotherapy and in combination with chemotherapy or targeted agents, has emerged as a promising approach to enhance the immune response in this disease entity.
Immune checkpoint inhibitors after progression to platinum-based chemotherapy
KEYNOTE-158: Pembrolizumab as monotherapy
Pembrolizumab is a humanized monoclonal anti-PD-1 antibody that has demonstrated encouraging clinical activity in patients with dMMR/MSI-H endometrial cancer.31–34 As monotherapy, pembrolizumab (200 mg intravenously every 3 weeks for 35 cycles) was assessed in the open-label, multicohort, phase II KEYNOTE-158 study in adult patients with multiple types of advanced solid tumors, including endometrial cancer irrespective of dMMR/MSI-H status (cohort D) and previously treated advanced solid dMMR/MSI-H non-colorectal cancer tumors including endometrial cancer (cohort K).31 Among 79 patients with dMMR/MSI-H endometrial cancer, the primary endpoint of objective response rate (ORR) was 48%, including a complete response (CR) of 14% and a partial response (PR) of 34%; the median duration of response (DoR) was not reached. The ORR was 53% among the 38 patients who had received <2 lines of prior therapy. The median PFS was 13.1 months, with PFS rates of 51% at 1 year, 41% at 2 years and 37% at 3 and 4 years. The median OS was not reached and the OS rates were 69% at 1 year, 64% at 2 years and 60% at 3 and 4 years. In terms of safety, 76% of patients experienced treatment-related adverse events (TRAEs), with a grade 3−4 event reported in 12% of patients. Immune-mediated AEs or infusion reactions occurred in 28% of patients (grade 3−4: 7%). Based on these results, Swissmedic approved pembrolizumab as monotherapy for the treatment of dMMR/MSI-H endometrial cancer.35
GARNET: Dostarlimab as monotherapy
Dostarlimab is another anti-PD-1 humanized monoclonal antibody that has been investigated in advanced or recurrent endometrial cancer. The single-arm, phase I GARNET trial assessed intravenous dostarlimab (500 mg every 3 weeks for 4 cycles, followed by 1,000 mg every 6 weeks until disease progression) in patients with dMMR/MSI-H disease and those with proficient (p)MMR/MSS disease.36 At median follow-ups of 16.3 months for the dMMR/MSI-H cohort (n=129) and 11.5 months for the pMMR/MSS cohort (n=161), the ORR was 43.5% (CR rate: 10.2%; PR rate: 33.3%) and 14.1% (CR rate: 1.9%; PR rate: 12.2%), respectively. The median time to response was 11.9 weeks and 12.1 weeks, respectively, with a median DoR not reached in either cohort among the responders. In the combined cohorts, three-quarters of TRAEs were grade 1–2, most commonly fatigue (17.6%), diarrhea (13.8%) and nausea (13.8%). Grade ≥3 TRAEs occurred in 16.6% of patients and 5.5% discontinued dostarlimab due to TRAEs. In Switzerland, dostarlimab is currently indicated as monotherapy for the treatment of adult patients with recurrent or advanced dMMR/MSI-H endometrial cancer that progressed during or after a prior platinum-containing regimen.37
Immune checkpoint inhibitors in combination with tyrosine kinase inhibitors
Although the introduction of ICIs has revolutionized the treatment of many types of cancer, along with endometrial, management strategies have continued to develop, especially by combining ICIs with targeted agents.38 These include tyrosine kinase inhibitors (TKIs) which are small molecules designed to modulate the activity of growth factor receptors that regulate tumor cell proliferation and survival, further reducing immune suppression and eliciting therapeutic responses.
KEYNOTE-775: Lenvatinib plus pembrolizumab
Proficient MMR endometrial cancer, which represents more than 70% of all endometrial cancers,21 is less immunogenic and achieves worse clinical response to single-agent pembrolizumab compared with dMMR/MSI-H disease.33,34 Lenvatinib, a multitargeted TKI of vascular endothelial growth factor receptors (VEGFR) 1−3, fibroblast growth factor receptors (FGFR) 1−4, platelet-derived growth factor receptor (PDGFR) α, RET and KIT, was investigated in combination with pembrolizumab in women with advanced, recurrent or metastatic endometrial cancer in the multicenter, open-label, phase III KEYNOTE-775 trial.39 This study enrolled 827 adult women (pMMR, n=697; dMMR, n=130) with any histologic subtype, except carcinosarcoma and sarcoma, whose disease progressed after platinum-based chemotherapy. Patients underwent 1:1 randomization to receive either lenvatinib (20 mg orally once daily) plus pembrolizumab (200 mg intravenously every 3 weeks) (n=411) or physician’s choice chemotherapy (doxorubicin or paclitaxel) (n=416).
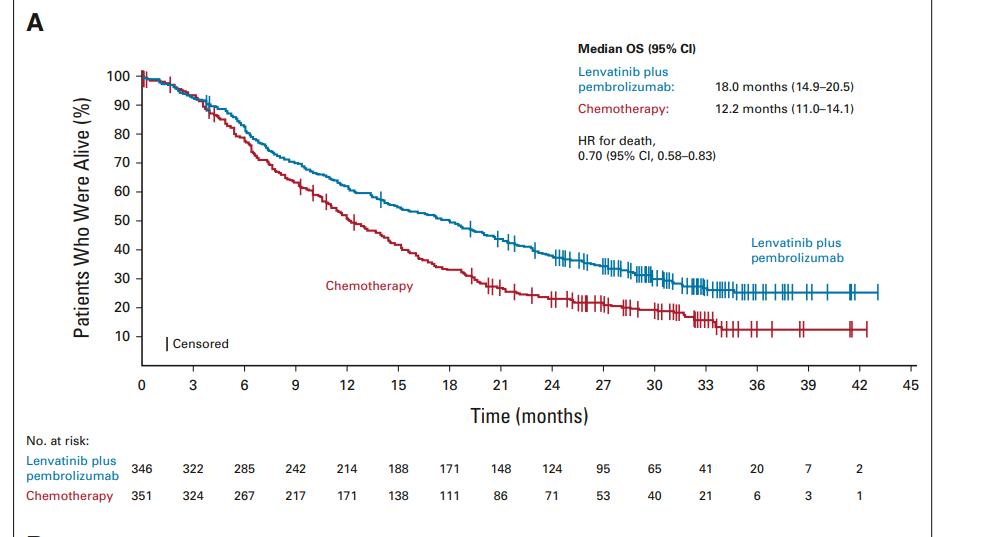
In the updated analysis at median follow-ups of 18.7 months in the lenvatinib plus pembrolizumab arm and 12.2 months in the chemotherapy arm, the median PFS in the pMMR population was 6.7 months versus 3.8 months, respectively (HR: 0.60 [95% CI: 0.50−0.72]).40 Similar PFS was observed in the overall population (HR: 0.56 [95% CI: 0.48−0.66]). The final prespecified OS analysis also showed improved OS among patients receiving lenvatinib plus pembrolizumab versus chemotherapy, with a median OS of 18.0 months versus 12.2 months in the pMMR population (HR: 0.70 [95% CI: 0.58−0.83]) (Figure 1) and 18.7 months versus 11.9 months in the overall population (HR: 0.65 [95% CI: 0.55−0.77]). Among patients with pMMR disease, ORR also favored lenvatinib plus pembrolizumab over chemotherapy, with ORR rates of 32.4% versus 15.1% (CR rate: 5.8% vs 2.6%) and a median DoR of 9.3 months versus 5.7 months, respectively. Comparable results were reported for the overall population. Notably, clinically meaningful improvements across efficacy endpoints were also observed with lenvatinib plus pembrolizumab in the dMMR population.39
_results_in_the_proficient_mismatch_repair_(pm.png)
Regarding safety, nearly all patients experienced any-grade treatment-emergent adverse events (TEAEs), most commonly hypertension (64.0%) with lenvatinib plus pembrolizumab and anemia (48.7%) with chemotherapy. In the updated analysis, grade ≥3 TEAEs occurred in 90.1% of patients receiving lenvatinib plus pembrolizumab and 73.7% of patients receiving chemotherapy (grade 5: 6.4% vs 5.2%).40 Following the positive results from KEYNOTE-775, lenvatinib in combination with pembrolizumab is indicated for the treatment of adult patients with advanced endometrial cancer without dMMR/MSI-H who have disease progression after prior platinum-based therapy and for whom curative surgery or radiation is not appropriate.41
Phase II study: Cabozantinib plus nivolumab
Data further showed that adding cabozantinib, a multitargeted TKI with potent activity against hepatocyte growth factor receptor (MET), VEGFR 2, RET and AXL, to nivolumab, a PD-1 ICI antibody, results in significantly improved clinical outcomes in heavily pretreated advanced, recurrent or metastatic endometrial cancer. In a translational randomized phase II trial, patients underwent 2:1 randomization to receive either cabozantinib (40 mg/day) plus nivolumab (intravenously 240 mg on days 1 and 15 of 28-day cycles) or single-agent nivolumab.42 At a median follow-up of 15.9 months, the median PFS was 5.3 months with combination therapy versus 1.9 months with nivolumab alone (log-rank test p=0.09). The ORR was 25% with the cabozantinib-containing regimen and 11% with nivolumab alone, resulting in overall clinical benefit rates of 69% versus 22%, respectively (p<0.001). OS data were immature at the data cut-off and showed a median OS of 13.0 months and 7.9 months, respectively. In an exploratory cohort of patients previously treated with immunotherapy (n=20), ICI rechallenge with cabozantinib plus nivolumab resulted in an ORR of 25%. As expected, TRAEs were more common with combination therapy and most frequently included diarrhea, liver enzyme elevations, fatigue and hypertension, mainly of grade 1−2. Serious TRAEs were reported in 31% of patients treated with cabozantinib plus nivolumab.
Immune checkpoint inhibitors in combination with chemotherapy in the first-line treatment
Research demonstrated that cytotoxic chemotherapy may have immune-stimulating effects, such as disruption of immunosuppressive pathways and enhanced cytotoxic T-cell response.43 Combining ICIs with chemotherapy may result in additive or synergistic clinical activity44 and several studies reported benefits with this combination regimen in different types of cancer.45–49
RUBY: Dostarlimab plus chemotherapy
The safety and efficacy of dostarlimab in combination with carboplatin and paclitaxel versus placebo plus carboplatin and paclitaxel were tested in adult women with primary advanced or recurrent (FIGO stage III/IV) endometrial cancer in the phase III, double-blind ENGOT-EN-6-NSGO/GOG-3031/RUBY trial.50 Here, 494 patients were randomly assigned in a 1:1 ratio to receive either dostarlimab (500 mg) (n=245) or placebo (n=249) plus carboplatin and paclitaxel every three weeks for the first six cycles, followed by maintenance dostarlimab (1,000 mg) or placebo for up to three years. The median follow-up was 24.8 months in the dMMR/MSI-H population (n=118) and 25.4 months in the overall population.
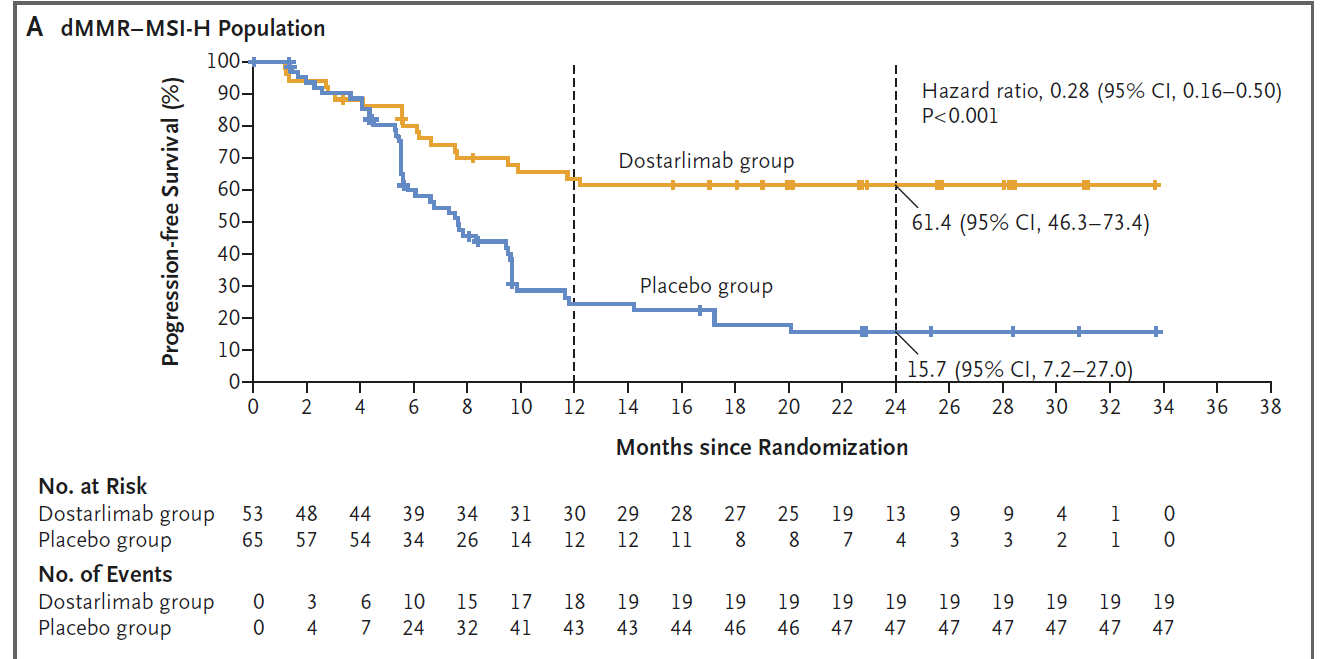
Results of the interim analysis showed that dostarlimab plus carboplatin and paclitaxel significantly improved the primary endpoint of PFS, with a substantial benefit in the dMMR/MSI-H population.50 In this subset, the 24-month PFS rate was 61.4% with dostarlimab and 15.7% with placebo, translating into a 72% reduced risk of progression or death with dostarlimab (HR: 0.28 [95% CI: 0.16−0.50]; p<0.001) (Figure 2 and Table 1). In the overall population, the PFS rate at 24 months was also significantly improved in the dostarlimab versus placebo arms (36.1% vs 18.1%; HR: 0.64 [95% CI: 0.51−0.80]; p<0.001). This PFS benefit with dostarlimab in both the dMMR/MSI-H population and overall was preserved across most subgroups, except for stage III disease and no disease at baseline. In terms of the co-primary endpoint of OS, the 24-month OS rate was 83.3% with dostarlimab and 58.7% with placebo (HR: 0.30 [95% CI: 0.13−0.70]) among patients with dMMR/MSI-H tumors. In the overall population, OS was also improved with dostarlimab versus placebo (24-month OS rate, 71.3% vs 56.0%; HR: 0.64 [95% CI: 0.46−0.87]) although the results did not reach the prespecified significance level. Data further demonstrated that in pMMR/MSS patients (n=376), the PFS rate at 24 months was 28.4% in the dostarlimab group and 18.8% in the placebo group (HR: 0.76 [95% CI: 0.59−0.98]) and the 24-month OS rate was 67.7% and 55.1%, respectively (HR: 0.73 [95% CI: 0.52−1.02]).
.png)
Regarding safety, the most common AEs were nausea (dostarlimab: 53.9% vs placebo: 45.9%), alopecia (53.5% vs 50.0%) and fatigue (51.9% vs 54.5%).50 Dostarlimab versus placebo was associated with increased incidences of grade ≥3 AEs (70.5% vs 59.8%) and serious AEs (37.8% vs 27.6%).
NRG-GY018: Pembrolizumab plus chemotherapy
The benefit of adding pembrolizumab to standard first-line chemotherapy of paclitaxel plus carboplatin in advanced, metastatic or recurrent endometrial cancer was assessed in the double-blind, phase III NRG-GY018 trial.51 Here, 816 adult women with newly diagnosed stage III/IVA disease (dMMR: n=225; pMMR: n=591) were randomized 1:1 to receive either pembrolizumab or placebo plus paclitaxel and carboplatin for 6 cycles, followed by pembrolizumab or placebo for up to 14 cycles. In the 12-month analysis in the dMMR cohort, the PFS rate was 74% with pembrolizumab and 38% with placebo, with a median PFS not reached and 7.6 months, respectively (HR: 0.30 [95% CI: 0.19−0.48]; p<0.001) (Table 1). Furthermore, at a median follow-up of 7.9 months in the pMMR cohort, the median PFS was 13.1 months in the pembrolizumab arm and 8.7 months in the placebo arm (HR: 0.54 [95% CI: 0.41−0.71]; p<0.001). Subgroup analyses further demonstrated that PFS in both the dMMR and pMMR cohorts favor pembrolizumab-based therapy across most prespecified subgroups. In terms of safety, any-grade AEs occurred in nearly all patients and most commonly included fatigue, peripheral sensory neuropathy and anemia. Similar frequencies of grade 3−4 AEs were identified in the dMMR and pMMR cohorts.
AtTEnd: Atezolizumab plus chemotherapy
In a phase Ia study, atezolizumab, an anti-PD-L1 antibody, demonstrated a favorable safety profile in patients with recurrent endometrial cancer, with durable clinical benefit in some patients, particularly those with higher PD-L1 expression.52 Based on these data, the multicenter, phase III, double-blind, randomized AtTEnd trial was designed to evaluate whether adding atezolizumab to carboplatin and paclitaxel, followed by maintenance atezolizumab or placebo, results in improved clinical outcomes in women with newly diagnosed advanced (stage III/IV) or recurrent endometrial cancer and measurable disease.53 In this study, 551 patients underwent 2:1 randomization to receive paclitaxel and carboplatin plus either atezolizumab (1,200 mg) (n=360) or placebo (n=189), followed by maintenance atezolizumab (1,200 mg) (n=356) or placebo (n=185) until disease progression.54 In the dMMR population, the results are consistent with the ones reported in the previous trials median PFS in the atezolizumab group was not reached versus 6.9 months in the placebo group at a median follow-up of 26.2 months, with 12-month PFS rates of 62.7% versus 23.3% and 24-month PFS rates of 50.4% and 16.0% (HR: 0.36 [95% CI: 0.23−0.57]; p=0.0005) (Table 1). PFS also favored atezolizumab in the all-comer population; the median PFS was 10.1 months compared with 8.9 months with placebo (HR: 0.74 [95% CI: 0.61−0.91]; p=0.0219). The 12-month PFS rates were 44.9% with atezolizumab versus 28.8% with placebo, while the 24-month PFS rates were 28.1% versus 17.0%, respectively. In an interim OS analysis with 43% data maturity, the median OS was 38.7 months among patients receiving atezolizumab and 30.2 months among patients receiving placebo, with 12-month OS rates of 80.1% versus 74.9% and 24-month OS rates of 62.2% versus 58.0%, respectively (HR: 0.82 [95% CI: 0.63−1.07]; p=0.0483 [significance not reached]). Clinical improvements in all comers were mainly due to the large effect observed in the dMMR population as PFS and OS benefit with atezolizumab versus placebo was reported in the pMMR population (Table 1). The safety profile of atezolizumab plus chemotherapy was manageable and consistent with expected toxicities.
DUO-E trial: Exploring PARP inhibition
Among novel treatment strategies for advanced or recurrent endometrial cancer, the combination of ICIs and poly(ADP-ribose) polymerase (PARP) inhibitors has been investigated in endometrial cancer. PARP inhibitors, including olaparib, rucaparib, niraparib and talazoparib, are currently approved in Switzerland for the treatment of a subset of patients with ovarian cancer and metastatic breast cancer. These PARP inhibitors target defective DNA repair which leads to accumulation of DNA damage and double-strand DNA breaks (DSBs).55,56 While the antitumor activity of ICIs is mainly based on the immune system stimulation which results in activation and infiltration of T cells, chronic PARP inhibition leads to sustained DNA damage that promotes several cellular mechanisms, such as increasing genomic instability, immune pathway activation and PD-L1 expression on cancer cells, which might promote responsiveness to ICIs.57
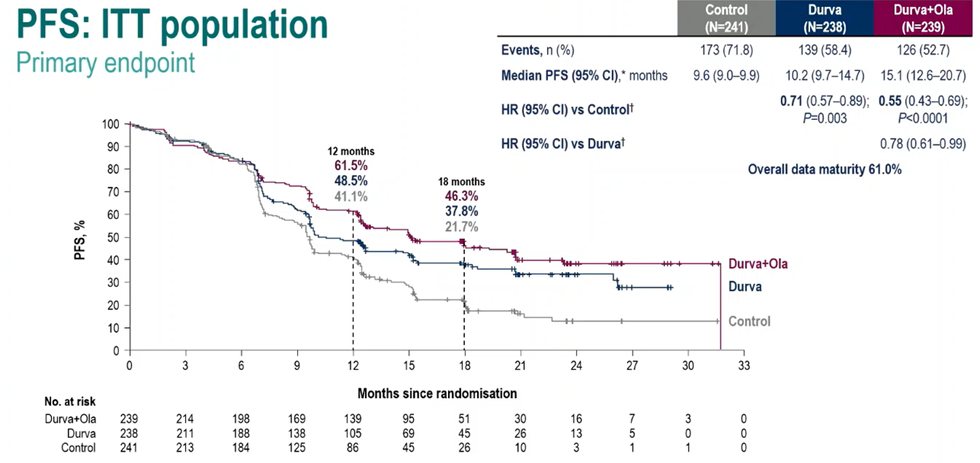
Very recently, the first results were reported from the double-blind, phase III DUO-E trial demonstrating that durvalumab, a PD-L1 inhibitor, plus platinum-based chemotherapy followed by maintenance durvalumab monotherapy or in combination with olaparib significantly prolongs PFS versus chemotherapy alone in patients with newly diagnosed recurrent or advanced (stage III/IV) endometrial cancer.58 In this three-arm study, adult women were randomly assigned 1:1:1 to receive carboplatin and paclitaxel plus placebo followed by maintenance placebo (control arm); durvalumab (1,120 mg once every 3 weeks) followed by maintenance durvalumab (1,500 mg every 4 weeks) plus placebo (durvalumab arm); or durvalumab followed by maintenance durvalumab plus olaparib (300 mg twice daily) (durvalumab plus olaparib arm). The trial met both primary endpoints of PFS. Compared with the control treatment (median PFS, 9.6 months), both treatment with durvalumab (median PFS, 10.2 months; HR: 0.71 [95% CI: 0.57−0.89]; p=0.003) and treatment with durvalumab plus olaparib (median PFS, 15.1 months; HR: 0.55 [95% CI: 0.43−0.69]; p<0.001) led to a significant reduction in the risk of disease progression or death (Figure 3). This PFS benefit with durvalumab and durvalumab plus olaparib versus control treatment was preserved across key prespecified subgroups, including homologous recombination repair (HRR) genes mutations (Table 1) and PD-L1 expression status. In the dMMR population, the addition of olaparib resulted in similar PFS compared to the durvalumab arm. Interestingly, in the pMMR subgroup patients in the durvalumab plus olaparib arm achieved the higher mPFS. In an interim analysis, the secondary endpoint of OS favored the two investigational arms at overall data maturity of 27.7%, but statistical significance was not reached at the data cut-off (durvalumab vs control, HR: 0.77 [95% CI: 0.56−1.07]; p=0.120; durvalumab plus olaparib vs control, HR: 0.59 [95% CI: 0.42−0.83]; p=0.003). Safety profiles of the treatment arms were generally consistent with those previously reported of individual agents. The overall incidence of grade ≥3 TEAEs was 56.4% in the control arm, 54.9% in the durvalumab arm and 67.2% in the durvalumab plus olaparib arm.
_in_the_intention-to-tre.png)
Future directions
Despite these encouraging data from clinical trials with immunotherapy, survival outcomes in patients with metastatic endometrial cancer remain poor and new treatment strategies have been extensively explored. There are several ongoing clinical studies and results are eagerly awaited. Here, a brief overview of the current trials is provided.
Ongoing clinical trials
RUBY part 2: Dostarlimab plus chemotherapy with niraparib maintenance
The combination of PARP inhibitor and immunotherapy has also been investigated in part 2 of the RUBY trial which aimed to evaluate the efficacy and safety of dostarlimab plus carboplatin and paclitaxel followed by dostarlimab plus niraparib in around 270 women with advanced (stage III/IV) or recurrent endometrial cancer.50,59 Of note, part 1 of RUBY demonstrated a statistically significant and clinically meaningful improvement in PFS with dostarlimab plus carboplatin and paclitaxel in the dMMR/MSI-H and the overall population versus placebo plus chemotherapy.42
LEAP-01: Frontline lenvatinib plus pembrolizumab
As discussed above, lenvatinib plus pembrolizumab yielded sustained clinical benefit versus chemotherapy in patients with previously treated advanced endometrial cancer who had measurable or radiographically apparent disease.39,40 This combination is now being further assessed in patients with newly diagnosed advanced (stage III/IV) or recurrent endometrial cancer previously not treated with systemic therapy.60 In the phase III, open-label ENGOT-en9/LEAP-001 trial, approximately 875 women will undergo 1:1 randomization to receive pembrolizumab plus lenvatinib or paclitaxel plus carboplatin. The co-primary endpoints are PFS and OS.
DOMENICA and KEYNOTE-C93: Frontline single-agent immune checkpoint inhibitors for dMMR/MSI-H
Although the standard treatment for advanced endometrial cancer is platinum-based combination chemotherapy, patients are often frail with coexisting morbidities which can significantly impact chemotherapy-related adverse outcomes. A chemotherapy-free regimen based on single-agent dostarlimab has been currently investigated in the open-label, phase III DOMENICA trial in patients with advanced or metastatic dMMR/MSI-H endometrial cancer.61 In this study, 142 women will be randomized 1:1 to receive either dostarlimab (500−1,000 mg for up to 24 months) or carboplatin plus paclitaxel and the primary endpoint is PFS.
Pembrolizumab is another ICI that is being investigated as monotherapy in patients with treatment-naive advanced dMMR/MSI-H endometrial cancer. Following the promising results from the KEYNOTE-158 study in patients with previously treated, advanced dMMR/MSI-H endometrial cancer,31 the phase III KEYNOTE-C93/GOG-3064/ENGOT-en15 trial was designed to further evaluate single-agent pembrolizumab in the frontline setting.62 In this study, approximately 350 patients will be randomized 1:1 to receive either pembrolizumab for up to two years or carboplatin plus paclitaxel for six cycles. Co-primary endpoints are PFS per RECIST v1.1 and OS.
RAINBO: Molecular class-directed adjuvant treatment strategies
Molecular classification of endometrial cancer provides a basis for more effective and safer treatment strategies for patients with endometrial cancer.63 Despite improved prognostication and decisions on adjuvant treatment over the past few years, several challenges remain, such as a high risk of recurrence and death and a lack of data from prospective clinical trials.64 To improve clinical outcomes and reduce the toxicity of unwarranted therapies in women with endometrial cancer, different adjuvant treatment strategies for each of the four molecular classes are currently under investigation in the RAINBO program. RAINBO is a platform of four international clinical trials: (i) p53abn-RED for women with invasive stage I–III p53abn endometrial cancer (adjuvant chemoradiation followed by olaparib for 2 years vs adjuvant chemoradiation alone); (ii) MMRd-GREEN for women with stage II (with lymphovascular space invasion [LVSI]) or stage III dMMR endometrial cancer (adjuvant radiotherapy with concurrent and adjuvant durvalumab for 1 year vs radiotherapy alone); (iii) NSMP-ORANGE is a treatment de-escalation trial for women with estrogen receptor-positive stage II (with LVSI) or stage III no specific molecular profile (NSMP) endometrial cancer (radiotherapy followed by progestin for 2 years vs adjuvant chemoradiation); (iv) POLEmut-BLUE trial to investigate the safety of de-escalation of adjuvant therapy in women with stage I–III POLE-mutated endometrial cancer (no adjuvant therapy for lower-risk disease and no adjuvant therapy or radiotherapy alone for higher-risk disease). The primary endpoints are recurrence-free survival at 3 years in the p53abn-RED (sample size, n=554), MMRd-GREEN (n=316) and NSMP-ORANGE (n=600) trials and pelvic recurrence at 3 years in the POLEmut-BLUE trial (n=145).
KEYNOTE-B21: pembrolizumab plus adjuvant chemotherapy with or without radiotherapy
The ENGOT-en11/GOG-3053/KEYNOTE-B21 is a phase III, randomized, double-blind study comparing pembrolizumab or placebo in combination with adjuvant chemotherapy with or without radiotherapy in patients with newly diagnosed, high-risk (stage I/II non-endometrioid, stage III/IVa, p53 abnormality) endometrial cancer after surgery with curative intent.65 Dual primary endpoints are disease-free survival and OS. Enrollment began in December 2020 and is currently ongoing.
Conclusion
A platinum-based chemotherapy regimen such as carboplatin plus paclitaxel has long been the standard systemic treatment for women with advanced or recurrent endometrial cancer. Advances in immunotherapy have reshaped the treatment landscape for these patients with traditionally limited therapeutic options. Single-agent anti-PD-1 regimens like pembrolizumab and dostarlimab are highly effective in patients with dMMR/MSI-H tumors, but their activity remains modest in less immunogenic molecular subtypes. Various combination strategies were shown to improve the efficacy of ICIs in women with advanced or recurrent endometrial cancer. Adding targeted therapies, such as TKIs lenvatinib or cabozantinib, or platinum-containing chemotherapy to immunotherapeutic drugs can increase tumor immunogenicity and reduce immune suppression in the tumor, further improving clinical responses. A novel treatment approach in the advanced/recurrent setting is combining ICIs with PARP inhibitors which demonstrated encouraging antitumor activity in this patient population. In the first-line treatment, ongoing clinical studies are currently investigating ICIs as single agents and in combination with a TKI. Altogether, findings from clinical trials showed that immunotherapy has a significant potential in the treatment of endometrial cancer. The key challenges, however, are selecting an optimal patient population based on biomarkers of response and identifying a combination regimen with improved efficacy and a favorable safety profile.
Conflict of interest
Ilaria Colombo has received travel grants from Tesaro, Janssen, AstraZeneca and GSK, honoraria for consultancy or expert opinion from AstraZeneca, GSK, Novartis, MSD and BionTech, as well as institutional grants for clinical trials as Principal Investigator from MSD, Bayer, Vivesto, Incyte, Astra Zeneca and Orion. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way. Other authors have declared that the manuscript was written in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
All authors have declared that no financial support was received from any organization for the submitted work.
Author contributions
All authors contributed to and approved the final manuscript.