Introduction
Ovarian cancer (OC) remains a significant challenge in oncology, necessitating continuous research and the development of innovative treatment approaches to improve clinical outcomes. Among these, poly (ADP-ribose) polymerase (PARP) inhibitors have emerged as a promising therapeutic option.1–3 This review provides an overview of PARP inhibitor-based treatments in OC, incorporating the latest findings presented at the 2023 ASCO annual meeting.
PARP inhibitors: Mechanism of action and clinical applications
The PARP enzymes have many functions in the cell, including the regulation of transcription, apoptosis and the DNA damage response.2 PARP inhibitors exploit the synthetic lethality concept, targeting cancer cells with defective homologous recombination DNA repair pathways, including those harboring BRCA1/2 mutations. By inhibiting PARP enzymes, PARP inhibitors prevent cancer cells from repairing DNA damage, leading to their selective death. Over the past decade, PARP inhibitors, including olaparib, niraparib and rucaparib, have demonstrated significant efficacy in the treatment of OC.1,3 They have shown remarkable benefits as maintenance therapy in patients with recurrent, platinum-sensitive disease, prolonging progression-free survival (PFS). Moreover, PARP inhibitors have also exhibited promising results as a first-line treatment in advanced OC patients, either as monotherapy or in combination with chemotherapy.
PARP inhibitors for ovarian cancer: Key findings from ASCO 2023
DUO-O: Combining PARP inhibitors with immune checkpoint inhibitors
ASCO 2023 presented exciting updates on the use of PARP inhibitors in OC treatment. Among novel therapeutic strategies are attempts to combine a PARP inhibitor with immune checkpoint inhibitors (ICIs) in patients with advanced OC. The DUO-O trial demonstrated that the addition of anti-programmed death-ligand 1 (PD-L1) ICI durvalumab and maintenance olaparib to the standard of care (SoC) prolongs PFS in advanced OC.
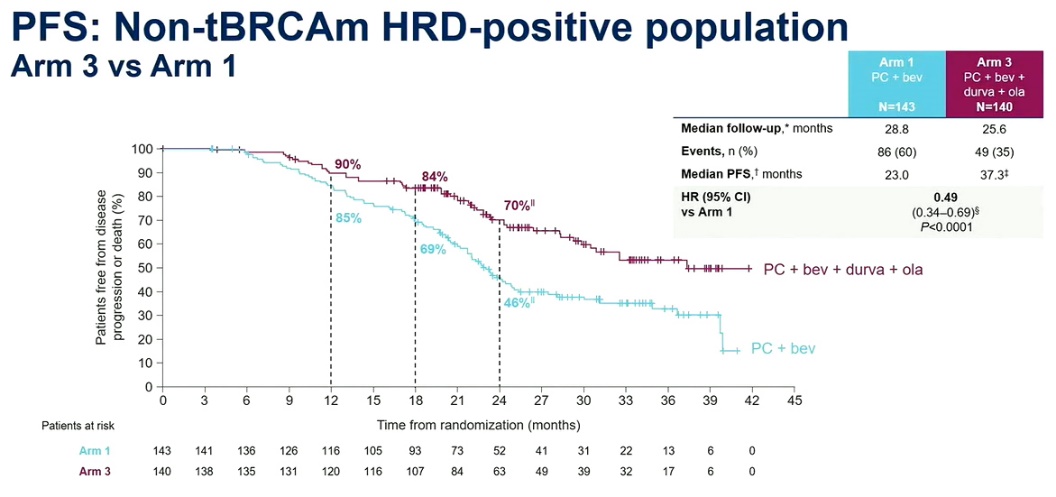
DUO-O is an international, phase III, randomized clinical trial that evaluated the addition of durvalumab to the SoC upfront chemotherapy with paclitaxel/carboplatin (P/C) plus bevacizumab, followed by maintenance bevacizumab plus durvalumab and olaparib in patients with advanced OC without BRCA mutations.4,5 The study enrolled 1,130 patients with newly diagnosed stage III or IV high-grade epithelial tumors negative for BRCA mutations, regardless of homologous recombination deficiency (HRD) status. Patients were randomized 1:1:1 to three treatment arms: Arm 1 (n=378), Arm 2 (n=374) and Arm 3 (n=378). All patients received SoC, followed by maintenance bevacizumab for up to 15 months. In addition, patients in Arms 2 and 3 received durvalumab during the chemotherapy phase. In the maintenance phase, patients in Arm 2 received durvalumab for 24 months and patients in Arm 3 received durvalumab and olaparib for 24 months. The primary endpoint was PFS in Arm 3 versus Arm 1 in the non-BRCA-mutated, HRD-positive population and the intent-to-treat (ITT) population. The key secondary endpoints were PFS in Arm 2 versus Arm 1, overall survival (OS) and safety.
In an interim analysis, a highly significant increase in PFS in patients treated with durvalumab plus olaparib was observed compared to the SoC regimen.5 For HRD-positive patients, PFS was 37.3 months in the durvalumab plus olaparib arm versus 23.0 months for those in the SoC arm (HR: 0.49 [95% CI: 0.34–0.69]; p<0.0001) (Figure 1). In the ITT population, PFS was 24.2 months with olaparib compared to 19.3 months with SoC. No significant difference in PFS between the SoC arm and Arm 2 was found in the ITT, although numerical improvement in PFS was observed. Safety profiles were generally consistent with the known profiles of each individual agent. Serious treatment-related adverse events (TRAEs) were reported in 34% of patients in the SoC arm, 43% in the maintenance durvalumab arm and 39% in the durvalumab plus olaparib arm. The most frequent grade ≥3 TRAEs included neutropenia, anemia, leukopenia, hypertension and thrombocytopenia. In summary, the addition of upfront durvalumab and maintenance olaparib to SoC significantly improved PFS in patients with newly diagnosed advanced OC without BRCA mutations.
_in_homologous_recombination_deficiency_(hrd)-positive_.jpeg)
PRIME: PARP inhibitors as maintenance therapy in advanced ovarian cancer
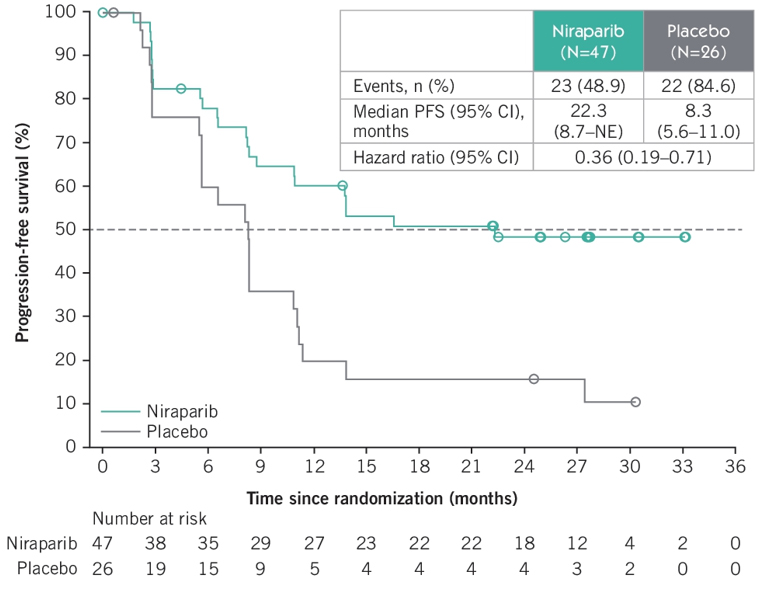
Encouraging results have also been reported at ASCO 2023 for another PARP inhibitor, niraparib. A post-hoc subgroup analysis of the PRIME study highlighted the benefits of using PARP inhibitors as maintenance therapy in newly diagnosed, advanced OC patients who had measurable residual disease.6,7 PRIME is a randomized, double-blind, placebo-controlled, phase III trial that enrolled 384 patients with newly diagnosed, stage III or IV OC who achieved a complete response (CR) or partial response (PR) after first-line platinum-based chemotherapy and received cytoreductive surgery. Patients were randomized at a 2:1 ratio to receive niraparib or placebo and stratified according to the status of germline BRCA mutations, HRD status, neoadjuvant chemotherapy and clinical response to first-line chemotherapy. The overall PFS median follow-up was 27.5 months. The analysis demonstrated that in the subgroup of patients with measurable residual disease (n=73) niraparib significantly extended PFS versus placebo (Figure 2), with a median PFS of 22.3 months versus 8.3 months, respectively (HR: 0.36 [95% CI: 0.19–0.71]). A confirmed objective response rate (ORR) of 57% was achieved with niraparib compared with 30.8% for placebo, regardless of the biomarker status. Importantly, patients who achieved further response during the maintenance phase tended to have much longer PFS compared to those without.
_in_patients_with_measurable_residual_disease_treated_w.jpg)
Among the most frequent grade ≥3 TRAEs were decreased platelet and neutrophil count (19.1% and 14.9%, respectively) and anemia (14.9%).6,7 In summary, maintenance therapy with niraparib was associated with high response rates and a significantly prolonged PFS compared with placebo in patients with newly diagnosed, advanced OC after surgery and platinum-based chemotherapy.
Ongoing research: Combinations with novel agents
There is growing interest in combining PARP inhibitors with other therapeutic agents to enhance efficacy.8 Potential synergistic partners for PARP inhibitors include immunotherapy agents, antiangiogenic drugs and other targeted therapies, inter alia. ASCO 2023 showcased ongoing research focusing on combinations of PARP inhibitors with novel agents characterized by improved pharmacokinetic profiles, increased potency and reduced adverse effects. Exactis-03 is a multicenter, phase I trial that aims to evaluate the combination of olaparib with an oral Bcl-2/Bcl-xL inhibitor navitoclax, which has demonstrated synergistic action in preclinical cancer models.9 The study enrolled patients with recurrent high-grade serous OC who have progressed ≥6 months since their last platinum-based chemotherapy. Prior treatment with a PARP inhibitor was allowed provided there was no progression on or ≤6 months since discontinuation of the therapy. The primary endpoint is the identification of the recommended phase II dose of olaparib combined with navitoclax. In parallel, tumor biopsies will be performed to evaluate senescence and apoptosis biomarkers and to create 3D organoids and ex vivo microdissected tumor models for functional assessment of drug response. Blood samples will be collected for pharmacokinetics and serial evaluation of plasma biomarkers.
A preclinical study by Foster et al. focused on a high-throughput screen of a set of FDA-approved drugs, clinical candidates and small-molecule probes to identify potential combination therapies to enhance the efficacy of PARP inhibition in OC.10 Among the compounds selected for final validation were CHK1/2 inhibitor AZD 7762, pan-CDK inhibitor dinaciclib, HSP90 inhibitor onalespib and topoisomerase 1 inhibitor SN-38. The analysis demonstrated a robust synergy of olaparib with AZD 7762 in both HRD and non-HRD ovarian cancer models.
Challenges and Future Directions
While PARP inhibitors have revolutionized OC treatment, many challenges still exist despite the significant benefits of the approach.11 Resistance to PARP inhibitors remains a concern, which stresses the need to understand the molecular mechanisms driving resistance and define strategies to predict which patients might develop it. Furthermore, while BRCA mutations are a known predictor of response to PARP inhibitors, the search is ongoing for other biomarkers that can help identify patients who would benefit the most from this therapy. Among other questions to be addressed are the potential long-term side effects, the optimal therapy duration, as well as cost-effectiveness and accessibility of the treatment. Nevertheless, PARP inhibitors represent a promising avenue in OC therapy, particularly given the unfavorable outcomes of other treatment strategies, such as immunotherapy. ICIs have gained prominence in clinical practice for managing several types of solid tumors; however, their efficacy in OC remains largely poor.12 For instance, in a recent phase III IMagyn050 trial, the addition of atezolizumab failed to improve the efficacy of platinum-based chemotherapy plus bevacizumab in patients with newly diagnosed stage III/IV OC.13 Further studies are needed to determine whether alternative drug combinations, including immunotherapy, PARP inhibitors and anti-angiogenic agents, can confer clinical benefits to OC patients.
Conclusion
PARP inhibitors have emerged as a groundbreaking treatment modality in OC, significantly impacting patient outcomes. The latest data presented at ASCO 2023 reinforce the effectiveness of PARP inhibitors as maintenance therapy and highlight the potential of combining them with ICIs for improved treatment responses. Ongoing research into novel agent combinations holds promise for further advancements. Despite challenges, PARP inhibitors have undoubtedly contributed to the paradigm shift in OC treatment and offer hope for improved survival and quality of life for patients with this devastating disease.
Conflicts of interest
Marcus Vetter received honoraria for serving on advisory boards from AstraZeneca and GSK, honoraria for consultancy from GSK, Roche, Novartis, Exact Sciences, Pfizer, Stemline, AbbVie and ASC Oncology, and grant support from GSK. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way. Yves van Roon has declared that the manuscript was written in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors have declared that no financial support was received from any organization for the submitted work.
Author contributions
All authors have contributed to and approved the final manuscript.