Introduction
The World Congress on Lung Cancer (WCLC), the largest gathering worldwide dedicated to lung cancer and other thoracic malignancies, took place from September 9 to 12, 2023, in Singapore. Organized by the International Association for the Study of Lung Cancer (IASLC), the congress not only presented ground-breaking research and practice-changing trial results but also offered many opportunities for attendees to connect and collaborate with fellow scientists and clinicians from all over the world with the common goal of fighting thoracic cancer.
In this review I will share some of the highlights from WCLC 2023, primarily focusing on targeted therapy. Numerous phase I and phase II study results were shown in the emerging field of antibody-drug conjugates (ADCs). Furthermore, there were also some data presented that shed light on the therapeutic options in the very challenging field of small cell lung cancer (SCLC). Concerning mesothelioma, the results of one very intrepid study harboring probably a fundamental impact in current treatment algorithms were shown.
Novel therapies in SCLC
The combination of immuno-oncology (IO) therapy with anti-angiogenic agents is a promising strategy for lung cancer treatment. Immune checkpoint inhibitors (ICIs) directed against programmed cell death-1 (PD-1) receptor or its ligand (PD-L1) have been shown to induce persistent tumor remission in many types of advanced cancers.1,2 Angiogenesis plays a crucial role in the development of solid tumors. Vascular endothelial growth factor (VEGF) is not only an important angiogenic factor but also an immunomodulator of the tumor microenvironment. The addition of anti-angiogenic drugs, such as monoclonal antibodies (mAb) and tyrosine kinase inhibitors (TKIs) targeting pro-angiogenic molecular pathways, may significantly improve the efficacy of IO therapy.3,4
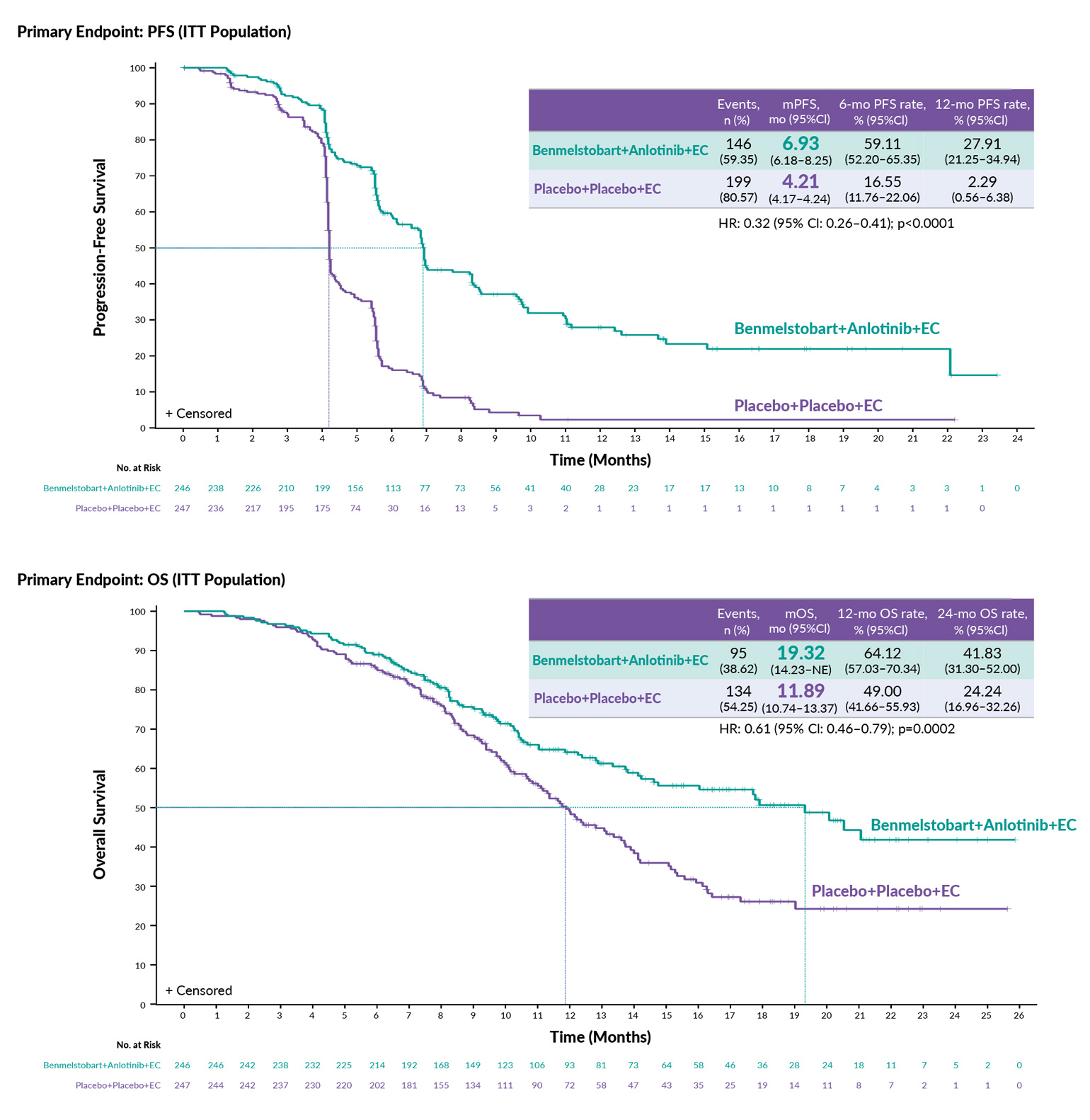
At WCLC 2023, Prof. Ying Cheng presented the data on the combination of an oral anti-vascular, multi-targeting tyrosine kinase inhibitor anlotinib and anti-PD-L1 mAb benmelstobart with carboplatin and etoposide for the first-line treatment of extensive-stage SCLC (ES-SCLC).5 In this phase III study conducted in China, 738 patients were randomized in a 1:1 ratio to receive either 4 cycles of carboplatin and etoposide chemotherapy plus placebo or chemotherapy plus anlotinib and benmelstobart including maintenance with both experimental substances. The median progression-free survival (PFS) in the intention-to-treat (ITT) population was 6.93 versus 4.21 months (p<0.0001) (Figure 1). The median overall survival (OS) was 19.32 months in the experimental group versus 11.89 months in the control group (p=0.0002) (Figure 1), with a median duration of response (DoR) of 5.75 months versus 3.09 months, respectively (p<0.0001). The objective response rate (ORR) was 81.3% versus 66.8%. The combination regimen showed a tolerable safety profile but specific multi-kinase-inhibitor side effects, such as hypertension of any grade (31.1% vs 7.3%) and palmoplantar erythrodysaesthesia (11.4% vs 1.2%), were more common in the group receiving chemotherapy plus benmelstobart and anlotinib versus chemotherapy plus placebo. More treatment-related deaths were reported in the experimental arm (4.5% vs 1.6%), unfortunately without any details on the causes.
In summary, the study demonstrated a significant survival benefit in the experimental arm, suggesting a potential synergistic immunomodulatory effect of anti-vascular and IO therapies. However, there are many caveats in this study, such as an inappropriately designed control arm and the inclusion of 20% of never-smokers in the ITT population, indicating possible variations in tumor biology and confounding direct translation of the data. Only a randomized trial with platinum-etoposide-PD-(L)1-inihibitor as the control arm can prove the additional benefit over the current standard of care (SoC). Currently, anlotinib is not available in Europe.
_and_overall_survival_(os)_in_patients_with_small_cell_.jpg)
Data of the CeLEBrATE study which also investigated the principle of combining anti-vascular and IO therapies was presented at the mini-oral session on SCLC by Prof. Giuseppe Lamberti from Bologna.6 This multicenter, single-arm, phase II study enrolled 53 patients who received carboplatin, etoposide, anti-PD-L1 monoclonal antibody atezolizumab and anti-VEGF monoclonal antibody bevacizumab. At the median follow-up of 19.1 months, the study reported a median OS of 12.7 months, with a 1-year OS of 61.8% and ORR of 67.9%. The study met its predefined endpoints – but those are very similar to those with carboplatin-etoposide-atezolizumab only in an indirect comparison with the IMpower133 study (median OS: 12.3 months, ORR: 64.4%).
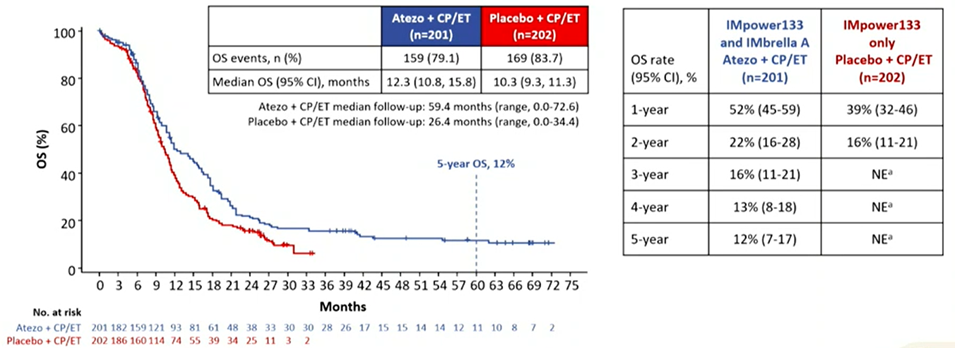
While the addition of anlotinib and benmelstobart to chemotherapy yielded a surprising survival benefit, the efficacy outcomes of the single-arm CeLEBrATE trial were underwhelming compared to our SoC. In the phase III IMpower133 trial, adding atezolizumab to carboplatin plus etoposide led to significantly longer OS and PFS in patients with previously untreated ES-SCLC. At WCLC 2023, Prof. Steven V. Liu from Washington presented the 5-year OS data of the phase IV single-arm IMbrella A study, which was an extension of results from IMpower133.7 Patients in the experimental arm (n=201) received carboplatin plus etoposide and atezolizumab and were followed for up to 5 years. OS rates were 16%, 13% and 12% after 3, 4 and 5 years, respectively (Figure 2). Compared to the historical 5-year OS of 2% for ES-SCLC before chemotherapy plus IO therapy became the SoC, these results confirm a durable benefit from atezolizumab in a subset of patients with ES-SCLC.
_outcomes.png)
There is an ongoing effort to further improve the treatment of SCLC. Among the emerging treatment targets is the inhibitory Notch ligand Delta-like-Ligand 3 (DLL3), a protein that is present on the Golgi apparatus of normal cells and is highly expressed on the cell surface of SCLC and neuroendocrine carcinomas.8 At WCLC 2023, Prof. Martin Wernke from Dresden University of Technology presented data from a phase I study on BI 764532,9 a novel DLL3/CD3 IgG-like T-cell engager that functions similarly to its competitor drug tarlatamab10 by redirecting the patient’s T-cells to lyse DLL3-expressing tumor cells. This first-in-human dose escalation study included patients with DLL-3-positive advanced SCLC, large-cell neuroendocrine carcinoma (LCNEC) or extrapulmonary neuroendocrine carcinoma (epNEC) with disease progression after at least one prior therapy, had adequate organ function and Eastern Cooperative Oncology Group performance status (ECOG PS) of 0−1.9 The median treatment duration was 43 days. With the dosage of <90 µg/kg, the disease control rate (DCR) was 39% in patients with SCLC (n=54) and 6 out of 9 patients (66%) in the LCNEC group had at least stable disease as best response. Even higher DCRs were observed with a dosage of ≥90 µg/kg: 51% for SCLC (n=39) and 100% for LCNEC (n=5). Drug discontinuations due to treatment-related adverse events (TRAEs) occurred in 6% of all patients. Cytokine release syndrome (CRS) was reported in 48% of patients, with most events occurring during the first infusion. These TRAEs were primarily grades 1−2 and considered manageable. Further upcoming data from studies evaluating this drug target are highly anticipated.
Antibody-drug conjugates for NSCLC therapy
Among the key topics discussed at the congress was the expanding field of antibody-drug conjugates (ADCs) in non-small cell lung cancer (NSCLC). ADCs represent a rapidly growing class of targeted drugs that comprise a monoclonal antibody directed against a tumor-specific antigen chemically linked to a cytotoxic agent.11,12
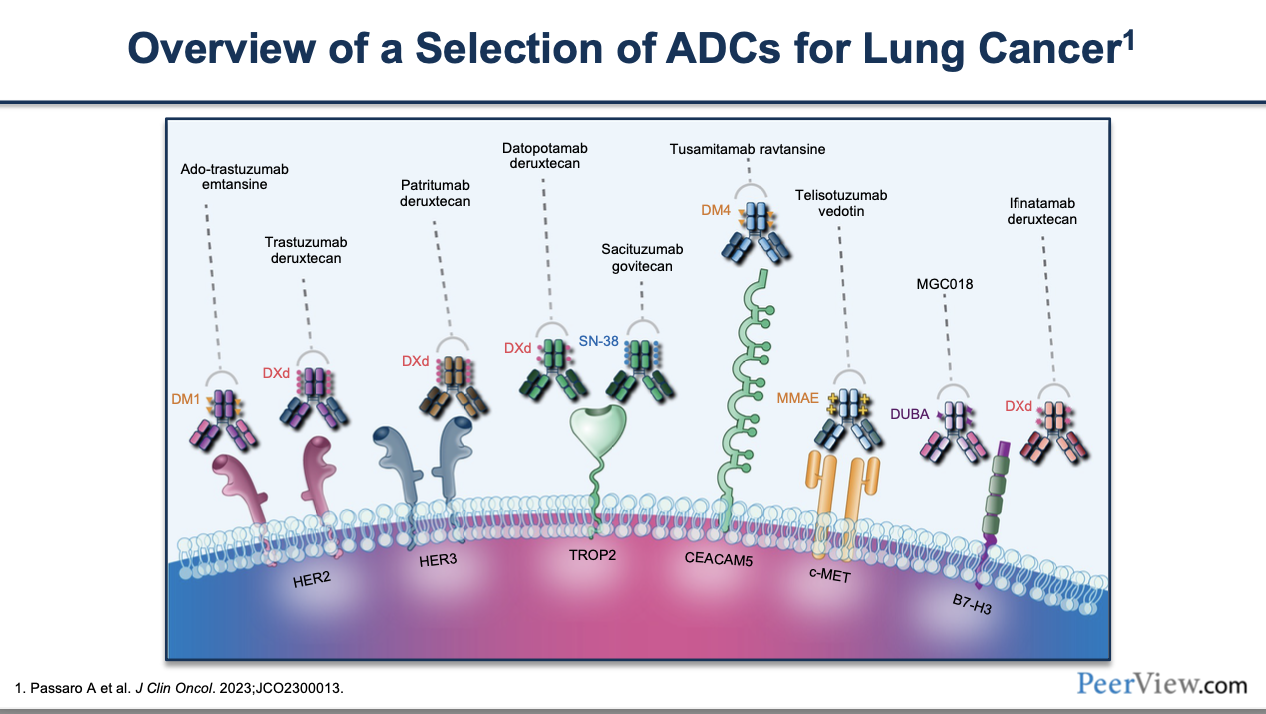
Numerous ongoing studies are currently investigating ADCs that target various molecules predominantly expressed on tumor cells. Among the promising antigen targets for NSCLC with the most advanced development are trophoblast cell surface antigen-2 (Trop-2), c-Met, CAECAM5, HER2, HER3 and B7-H3 (Figure 3).13
_in_lung_cancer_therapy.png)
EVOKE-02 is an ongoing, global, open-label, multicohort phase II study that evaluates the Trop-2-targeted ADC sacituzumab govitecan (SG) in combination with pembrolizumab with or without a platinum agent as first-line treatment for NSCLC.14 Trop-2 is a transmembrane glycoprotein that is upregulated in many cancer types, making it a potent therapeutic target for ADCs.15 SG has demonstrated significant survival benefits compared to chemotherapy in metastatic breast cancer16 and urothelial cancer.17 At WCLC 2023, Prof. Byoung Chul Cho from South Korea presented the preliminary results of EVOKE-02 on SG in combination with pembrolizumab in two cohorts of patients with previously untreated stage IV NSCLC without actionable genomic alterations (AGA).14
Patients were stratified according to PD-L1 expression: cohort A with high PD-L1 (≥50%) (n=30) and cohort B with low PD-L1 (<50%) (n=60).14 The study demonstrated encouraging antitumor activity across both subgroups. ORR was 69% and 44% in high and low PD-L1 cohorts, respectively. Mean DoR was not yet reached in either group. The safety profile was manageable, with grade ≥3 TRAEs reported in 38% of patients, most of them being related to the chemotherapy component of the regimen. Treatment discontinuation due to TRAEs occurred in 18% of patients. The phase III EVOKE-03 study comparing SG plus pembrolizumab versus pembrolizumab monotherapy in patients with high PD-L1 expression is ongoing.
Treatment strategies in mesothelioma
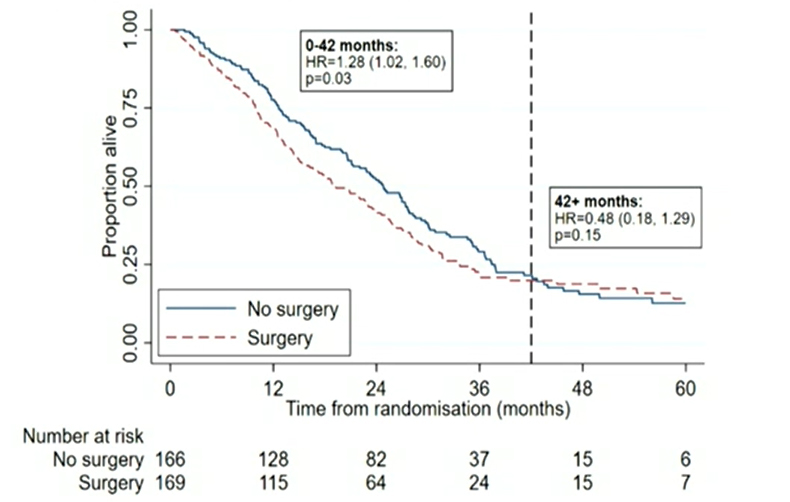
Last but not least, important data on treatment approaches to mesothelioma were presented at the presidential session of the congress by Prof. Eric Lim, a thoracic surgeon from London. The multicenter, randomized MARS 2 trial evaluated the effectiveness of (extended) pleurectomy decortication in patients with resectable malignant pleural mesothelioma (MPM).18 Overall, 335 patients received 2 cycles of carboplatin and pemetrexed induction and, when still considered resectable, were randomized in a 1:1 ratio to either extended pleural decortication followed by 4 more cycles of chemotherapy or only 4 more cycles of chemotherapy (Figure 4). The primary endpoint of this superiority trial was OS. Proportional hazards were not respected with a crossing of the OS curves at 42 months. In the first 42 months, the study demonstrated a 28% increase in the risk of death in the surgery plus chemotherapy group compared to chemotherapy alone (HR: 1.28 [95% CI: 1.02−1.60]; p=0.03), while there was no significant OS benefit in the few patients (15 per group) alive after 42 months (HR: 0.48 [95% CI: 0.18−1.29]; p=0.15). These outcomes did not differ when the epithelioid subgroup (86% of patients) was observed independently. At the same time, more TRAEs were observed in the group that underwent surgery. Furthermore, quality of life according to the EQ5D Score was worse in this patient group, along with higher overall treatment costs. The British group led by Prof. Eric Lim managed to design and run a randomized trial between surgical intervention and no surgical intervention. It cannot be highlighted enough what a success the timely completion of this trial with over 300 patients is. Despite minor caveats and criticisms that need clarification in the submitted publication, it changes the SoC in the treatment of patients with MPM to the extent that extended decortication pleurectomy should not generally be offered to patients with any type of MPM anymore. The discussion of the trial by Prof. Paula Ugalde, a thoracic surgeon from Brigham and Women’s Hospital in Boston, USA, led to intense reactions in the audience and on social media channels as she wrongly stated that the results of the trial were not significant and suggested that the lack of OS benefit with surgery was due to a lack of experience of half of the centers participating in this trial (the majority of which are accredited mesothelioma treatment centers). The reactions highlight that discussions around concepts of “less is more” in oncology are not always easy, a fact that certainly does not only apply to surgical trials. Upcoming discussions among thoracic surgeons will extensively address this topic.
_in_patients_with_resectable_mesothelioma_treated_with_ex.jpg)
Conclusion
Recent studies presented at WCLC 2023 underscore the potential of combining immuno-oncology therapies with anti-angiogenic agents in enhancing treatment outcomes for both SCLC and NSCLC, as well as affirm the potential of ADCs in NSCLC therapy. In mesothelioma treatment, we have a potentially practice-changing negative trial showing no benefit of extended pleurectomy. Together, these and other studies outline novel avenues for managing thoracic malignancies, thus offering new hope for patients.
Conflicts of interest
The author serves as a principal investigator for Daiichi Sankyo and GSK and has received advisory board payments from Servier, Astra Zeneca and Sanofi, as well as travel grants from several pharmaceutical companies. The funding entities and sponsors of Dr Kraus’s studies did not play a role in the development of the manuscript and did not influence its content in any way.
Funding
The author has declared that no financial support was received from any organization for the submitted work.
Author contributions
The author created and approved the final manuscript.