Introduction: Ovarian Cancer Diagnostics and Therapy
Ovarian cancer remains a global health challenge due to its often asymptomatic nature in its early stages, leading to delayed diagnosis, advanced stage and limited treatment options upon presentation. This malignancy ranks as the eighth most common cancer in women worldwide and is associated with high mortality rates due to late-stage diagnosis, aggressive behavior and a tendency to recur even after successful initial treatment.1 In Switzerland, approximately 700 patients are diagnosed each year and still 60–70% of patients will have relapsed disease within five years.2 The most common subtype is high-grade serous ovarian cancer with a high rate of homologous repair deficiency (HRD) gene alterations in 50% of cases.3 Clinical care for patients with ovarian cancers in Switzerland is organized in clinical networks and cancer centers and in the future, surgery is only allowed in larger hospitals with special regulations including case numbers and physician’s certification. Traditional therapeutic strategies encompass surgical intervention, platinum-based chemotherapy and targeted therapies, but the advent of PARP inhibitors has revolutionized ovarian cancer treatment and management.
Subtypes of Ovarian Cancer and Their Mutational Landscape with implications to PARP Inhibitors
Ovarian cancer comprises a heterogeneous group of malignancies, each with distinct histopathological and molecular characteristics.3 The major subtypes include epithelial ovarian cancer (EOC). In addition, non-epithelial ovarian cancer including germ cell tumors (GCTs) and sex cord-stromal tumors (SCSTs) can occur. Among these, EOC is the most common and can be further categorized into serous, endometrioid, clear cell and mucinous subtypes. The mutational landscape of ovarian cancer highlights the diverse genetic alterations driving tumorigenesis.4 High-grade serous ovarian cancer, the most aggressive EOC subtype, frequently harbors mutations in TP53, along with alterations in BRCA1/2, PTEN and homologous recombination genes. Endometrioid ovarian cancer is often characterized by PTEN and ARID1A mutations, while clear cell ovarian cancer frequently displays mutations in ARID1A, PIK3CA and PPP2R1A. Mucinous ovarian tumors are less common and often harbor KRAS and TP53 mutations. Germ cell and sex cord-stromal tumors exhibit distinct mutational profiles, with GCTs occasionally involving mutations in the KIT and KRAS genes. These diverse mutational landscapes underscore the importance of tailored therapeutic approaches for different ovarian cancer subtypes, reflecting the complex interplay between genetic alterations and disease behavior.
Homologous Recombination Deficiency (HRD) Testing in Ovarian Cancer
HRD is a crucial biomarker in ovarian cancer that defines treatment decisions, particularly in the context of PARP inhibitor therapy.5,6 HRD refers to impaired DNA repair mechanisms, often caused by mutations in genes involved in homologous recombination repair. Various HRD tests are used to assess the genomic instability associated with this deficiency.7 The Myriad HRD test evaluates three distinct genomic features: loss of heterozygosity, telomeric allelic imbalance, and large-scale state transitions.8 All three scores are highly correlated with BRCA1/2 mutations and are associated with sensitivity to platinum agents. The HRD score is calculated as the sum of the three individual scores.9–12 The FoundationOne CDx test identifies genomic alterations, including somatic BRCA1/2 mutations and genomic LoH, to determine HRD status.13 Additionally, the HRDetect algorithm analyzes large-scale genomic data to predict HRD status, considering mutational patterns associated with defective homologous recombination.14 Accurate HRD testing is crucial for identifying patients who are likely to benefit from PARP inhibitor therapy and for guiding personalized treatment strategies in ovarian cancer management.
A groundbreaking advancement in the realm of ovarian cancer diagnostics has emerged with the advent of a novel form of HRD testing, including the pioneering test developed by the Geneva Group.15 This innovative approach harnesses cutting-edge techniques to evaluate the genetic landscape of ovarian tumors, enabling clinicians to garner crucial insights into the disease progression and potential therapeutic strategies. The Geneva Group’s HRD testing methodology analyzes intricate patterns of genomic instability and homologous recombination deficiency, offering a comprehensive understanding of the tumor’s vulnerabilities and genetic makeup. The test used 469 samples from the PAOLA-1 study that examined the role of bevacizumab plus/minus olaparib in first-line maintenance ovarian cancer patients. The new HRD assay was using the TCGA Atlas genes as part of the ENGOT HRD European initiative. Results were compared with the Myriad myChoice Genomic Instability Score (GIS) with respect to the progression-free survival (PFS) in the bevacizumab plus/minus olaparib cohort. The new test was able to predict more precise HRD samples and demonstrated a lower failure rate in the nLST-positive samples. In BRCAwt samples the test yields a new subpopulation of patients with a better 1-year PFS of 85% but a poor 2-year PFS of 30% for patients on bevacizumab plus olaparib. The authors conclude that the test is more precise and has a lower failure rate in separating patients with HRD-proficient (HRP) and HRD-deficient tumors. Another advantage is the easy implementation of the test into routine practice in every molecular laboratory.
These data empower oncologists to make more informed decisions regarding personalized treatment options, such as targeted therapies or precision medicine interventions, thereby significantly enhancing the prospects for improved patient outcomes. As the Geneva Group’s technique gains momentum, it holds the promise to revolutionize ovarian cancer management by ushering in an era of tailored therapies that address the unique genetic characteristics of each patient’s tumor, ultimately advancing the fight against this disease.
PARP Inhibitors: Mechanism of Action and Rationale
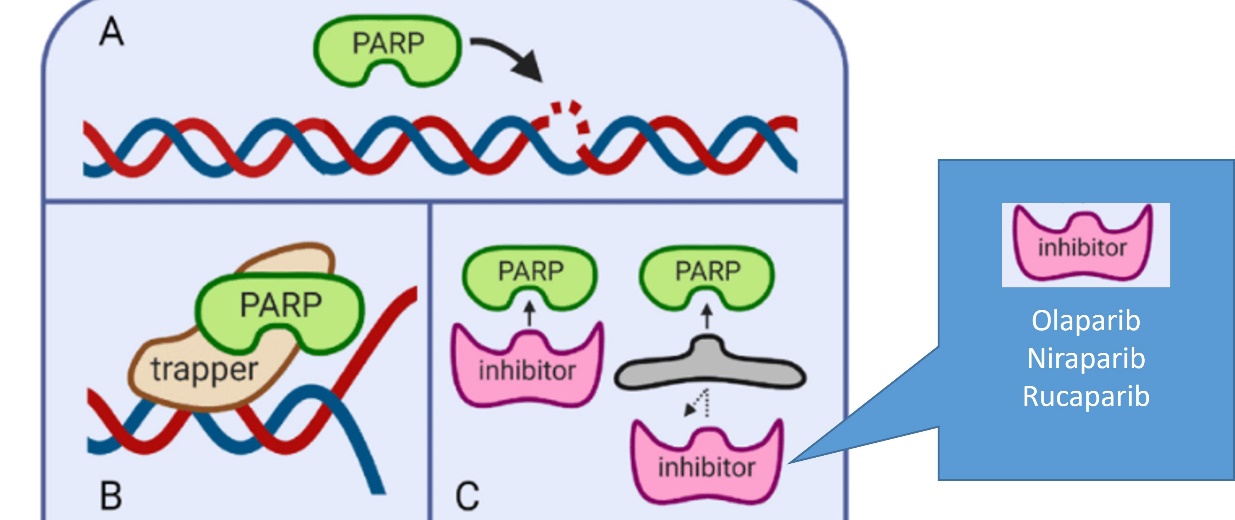
PARP is a critical enzyme involved in DNA repair, primarily in the base excision repair pathway.16 PARP inhibitors represent a novel therapeutic approach that exploits synthetic lethality, a phenomenon wherein the inhibition of two separate DNA repair pathways leads to the accumulation of DNA damage, culminating in cell death (Figure 1).17 This concept is particularly pertinent in the context of ovarian cancer, where patients with mutations in the BRCA1 or BRCA2 genes have compromised homologous recombination DNA repair mechanisms, making them highly susceptible to the effects of PARP inhibition.

BRCA mutations have emerged as pivotal factors in the landscape of ovarian cancer, significantly shaping our understanding of the disease’s genetics, prognosis and treatment strategies.18 These mutations, particularly in the BRCA1 and BRCA2 genes, are known to be associated with an increased susceptibility to ovarian and breast cancers. Individuals carrying these mutations have a higher lifetime risk of developing ovarian cancer, and their detection often influences the course of treatment. BRCA mutations affect the mechanisms responsible for DNA repair, leading to genomic instability and an increased likelihood of accumulating genetic alterations.18 This contributes to the development and progression of ovarian cancer, often resulting in more aggressive tumors. Moreover, the identification of BRCA mutations has not only provided insights into the underlying biology of ovarian cancer but also paved the way for targeted therapies.
PARP inhibitors, a class of drugs that exploit the defective DNA repair mechanisms caused by BRCA mutations, have revolutionized ovarian cancer treatment.17 These inhibitors specifically target cancer cells with BRCA mutations, impairing their ability to repair DNA damage and thereby inducing cell death. This approach offers a more precise and effective therapeutic option for patients with BRCA-mutated ovarian cancer, improving response rates and PFS and demonstrating a trend towards prolonged overall survival (OS).
As our understanding of the interplay between BRCA mutations and ovarian cancer continues to evolve, ongoing research aims to unravel additional genetic interactions and mechanisms that influence disease progression. This knowledge not only enhances risk assessment and early detection but also holds the promise of expanding the arsenal of tailored therapies for patients, ushering in a new era of precision medicine in ovarian cancer management.
PARP Inhibitors: Clinical Landscape and Efficacy
Several PARP inhibitors, including olaparib, niraparib and rucaparib, have undergone extensive clinical evaluation for ovarian cancer treatment and are also in clinical practice or development for women with breast cancer.
Olaparib
Olaparib, the first PARP inhibitor to secure FDA approval for ovarian cancer, has demonstrated remarkable efficacy in clinical trials. A phase II, double-blind, placebo-controlled Study 19 trial evaluated olaparib (400 mg twice daily) in relapsed platinum-sensible high-grade ovarian cancer.19–21 In total, 265 patients with a partial response (PR) or complete response (CR) and at least two lines of platinum-based chemotherapy were randomized 1:1 to the maintenance therapy with olaparib or placebo. The median PFS was 8.4 versus 4.8 months (HR for progression or death: 0.35 [95% CI: 0.25–0.49]; p<0.001). All patients with olaparib maintenance had a better outcome regardless of subgroup. The most common side effects included nausea, vomitus, fatigue and anemia. In a long-term follow-up published in 2018, olaparib maintenance was ongoing in 24% of patients over 2 years and 11% over 6 years.22 A numeric OS benefit was observed with olaparib versus placebo maintenance (HR: 0.73 [95% CI: 0.55–0.95]; p=0.02138) irrespective of germline BRCA1/2 mutations, although the predefined threshold for statistical significance was not met. A post-hoc analysis of the BRCA status of patients enrolled to Study 19 demonstrated the highest benefit in terms of PFS for patients with a BRCA mutation treated with olaparib maintenance, with a PFS of 11.2 versus 4.3 months for olaparib versus placebo maintenance (HR: 0.18 [0.10–0.31]; p<0.0001).20 There was also a significant PFS benefit for patients with BRCAwt status, with a PFS of 7.4 versus 5.5 months for olaparib versus placebo maintenance (HR: 0.54 [95% CI: 0.34–0.85]; p=0.0075).
The pivotal phase III SOLO-1 trial evaluated olaparib as maintenance therapy in patients with BRCA-mutated advanced ovarian cancer who had achieved CR or PR to platinum-based chemotherapy. The results were striking, with a median PFS of 56.0 months in the olaparib group compared to 13.8 months in the placebo group (HR: 0.33 [95% CI: 0.25–0.43]).23 This impressive extension in PFS underscores the potential of PARP inhibitors to significantly delay disease progression.
The SOLO-2 study represents a pivotal milestone in the field of ovarian cancer treatment, particularly in the context of patients with BRCA mutations.24 Olaparib was evaluated in this landmark clinical trial to assess its efficacy and safety as a maintenance therapy for women with recurrent ovarian cancer and BRCA1/2 mutations. The trial enrolled patients who had responded to platinum-based chemotherapy and then received olaparib as a maintenance therapy. The primary endpoint of the study was PFS.
Conducted by AstraZeneca, the SOLO-2 study demonstrated groundbreaking results. Patients receiving olaparib experienced a significant extension in PFS compared to those on a placebo (19.1 months vs 5.5 months, HR: 0.30 [95% CI: 0.22–0.41]; p<0.0001).24 This finding underscored the potential of olaparib to effectively target the specific vulnerabilities caused by BRCA mutations, further validating the concept of personalized medicine in cancer treatment. The success of the SOLO-2 trial led to the approval of olaparib by regulatory agencies for the maintenance treatment of BRCA-mutated ovarian cancer patients who had achieved a response to platinum-based chemotherapy. This development marked a significant advancement in the treatment landscape, offering patients a targeted therapy that addresses the underlying genetic basis of their cancer.
Based on these results, olaparib is also approved in Switzerland for the treatment of newly diagnosed ovarian cancer as maintenance therapy in patients with BRCA-mutated advanced (FIGO stage III and IV) high-grade serous ovarian cancer following first-line (neo)adjuvant platinum-containing chemotherapy in the presence of complete or partial remission.25 Of note, before starting treatment with olaparib, it must be confirmed that the patient has a BRCA mutation (detected in the tumor tissue or the germline).
The SOLO-2 study and the subsequent approval of olaparib not only emphasized the potential of PARP inhibitors as a therapeutic approach but also highlighted the importance of genomic profiling and personalized medicine in tailoring treatments to individual patients. These study findings continue to impact clinical practice, shaping the way we approach the treatment of ovarian cancer and contributing to improved outcomes for patients with BRCA mutations.
The PAOLA-1 study has emerged as a pivotal investigation in the realm of ovarian cancer treatment, shedding light on the potential of olaparib as a targeted therapy.26,27 This groundbreaking clinical trial evaluated the efficacy of combining olaparib with an anti-angiogenic agent bevacizumab as a maintenance treatment for patients with newly diagnosed advanced ovarian cancer who had responded to platinum-based chemotherapy. The study aimed to explore whether this combination therapy could extend PFS and OS in this patient population.
The results of the PAOLA-1 trial are highly promising. The combination of olaparib and bevacizumab as maintenance therapy demonstrated a substantial improvement in PFS versus placebo plus bevacizumab (22.1 months vs 16.6 months, HR: 0.59 [95% CI: 0.49–0.72]; p<0.001),27 as well as in OS, with 5-year OS rates of 65.5% versus 48.4% (HR: 0.62 [95% CI: 0.45–0.85]).26 The significantly better survival rates in the combination therapy group highlight the synergistic effect of targeting both DNA repair mechanisms and tumor vasculature. Importantly, the improvement in OS indicated that the combination therapy not only delayed disease progression but also translated into extended survival benefits for patients.
These remarkable outcomes from the PAOLA-1 study have not only expanded the therapeutic armamentarium for ovarian cancer but also underscored the potential of combining targeted agents to optimize treatment outcomes. The robust improvement in both PFS and OS underscores the significance of this approach in improving the overall prognosis for patients with advanced ovarian cancer. This research represents a significant stride towards tailoring therapies to the genetic and molecular characteristics of individual patients, ushering in a new era of precision medicine in the management of ovarian cancer.
Olaparib in combination with bevacizumab has also been approved by the Swissmedic as maintenance therapy in patients with advanced (FIGO stage III and IV) high-grade serous ovarian cancer in the presence of complete or partial remission following first-line platinum-taxane chemotherapy combined with bevacizumab and whose ovarian cancer has a BRCA mutation or other HRD with genomic instability.25 Before starting treatment with olaparib, it must be confirmed that the patient has either a BRCA mutation or another HRD with genomic instability. Detection of HRD with genomic instability must be done using a validated test method.
Niraparib
The phase III NOVA trial established niraparib as a formidable treatment option for patients with recurrent ovarian cancer who responded to platinum-based chemotherapy.28 This study included both BRCA-mutated and non-BRCA-mutated patients, making it a valuable contribution to the field. Niraparib maintenance therapy led to a median PFS of 21.0 months in the niraparib group compared to 5.5 months in the placebo group (HR: 0.27 [95% CI: 0.17–0.41]). Notably, patients across all subgroups, regardless of BRCA mutation status, benefited from niraparib treatment, affirming its broader efficacy. Based on these data, niraparib is currently approved by Swissmedic as maintenance therapy in patients with advanced (FIGO stage III to IV) high-grade serous ovarian, tubal or peritoneal carcinoma at high risk of recurrence and a BRCA mutation or other HRD with genomic instability in the presence of complete or partial remission after platinum-based first-line chemotherapy.29 Of note, following the publication of the final OS analysis of NOVA, there was a withdrawal of the FDA approval of maintenance niraparib for patients with recurrent platinum-sensitive ovarian cancer that is not gBRCA associated.30
In the phase III PRIMA trial, niraparib maintenance treatment significantly extended PFS compared with placebo in patients with newly diagnosed advanced ovarian cancer with CR or PR to first-line platinum-based chemotherapy. The median PFS was 24.5 versus 11.2 months (HR: 0.52 [95% CI: 0.40–0.68]) in the homologous recombination–deficient population and 13.8 versus 8.2 months (HR: 0.66 [95% CI: 0.56–0.79]) in the overall population with niraparib versus placebo, respectively.31
The PRIME study, which included a broader, more representative patient population compared with PRIMA by enrolling patients with stage III disease who achieved R0 resection at primary debulking surgery, also demonstrated prolonged PFS with niraparib maintenance versus placebo irrespective of postoperative residual disease or biomarker status.32
Niraparib is also indicated as maintenance therapy in adult patients with platinum-sensitive, recurrent primary epithelial serous high-grade (highly dedifferentiated) ovarian, tubal or peritoneal carcinoma who have had a complete or partial response to platinum-based chemotherapy. Before starting treatment, it must be confirmed that the patient has either a BRCA mutation or another HRD with genomic instability. Detection of HRD with genomic instability must be done using a validated test method.
Rucaparib
The phase III ARIEL3 trial evaluated rucaparib as a maintenance therapy in platinum-sensitive recurrent ovarian cancer patients.33 The study included patients with BRCA mutations, as well as those with high genomic LoH, representing a more encompassing patient population. In the BRCA-mutated subgroup, the median PFS in the rucaparib group was 16.6 months compared to 5.4 months in the placebo group (HR: 0.23 [95% CI: 0.16–0.34]; p<0.0001). Importantly, patients with high LoH but without a BRCA mutation also experienced significant benefit from rucaparib, with a median PFS of 13.6 months compared to 5.4 months in the placebo group (HR: 0.32 [95% CI: 0.24–0.42]; p<0.0001). The ATHENA-MONO trial also demonstrated efficacy of first-line maintenance rucaparib in patients with newly diagnosed stage III-IV high-grade ovarian cancer including those without BRCA1 or BRCA2 mutations or other evidence of HRD, or high-risk clinical characteristics such as residual disease. Median PFS with rucaparib versus placebo was 28.7 months versus 11.3 months in the HRD-positive population (HR: 0.47 [95% CI: 0.31–0.72]; p=0.0004), 20.2 months versus 9.2 months in the intent-to-treat population (HR: 0.52 [95% CI: 0.40–0.68]; p<0.0001) and 12.1 months versus 9.1 months in the HRD-negative population (HR: 0.65 [95% CI: 0.45–0.95]), respectively.34
Following these data, rucaparib received authorization by Swissmedic as maintenance therapy in adult patients with advanced, platinum-sensitive, recurrent, high-grade serous ovarian, fallopian tube or primary peritoneal carcinoma, following platinum-based chemotherapy in the presence of complete or partial remission.35
Combination Therapy: PARP Inhibitors plus Immunotherapy and Bevacizumab
The evolving landscape of ovarian cancer treatment includes promising strategies involving combination therapy. Immunotherapy, particularly immune checkpoint inhibitors (ICIs) like pembrolizumab, has shown potential in clinical trials when used in combination with PARP inhibitors. Early results from studies such as KEYNOTE-100 suggest enhanced response rates and extended survival in patients receiving the combination of pembrolizumab and PARP inhibitors.36 The study enrolled patients with advanced ovarian cancer who were stratified into two cohorts. Cohort A received ≤2 prior chemotherapy lines for recurrent disease and had a platinum-free or treatment-free interval (PFI/TFI) of ≥3 to 12 months, while cohort B received 3-5 prior chemotherapy lines and had a PFI/TFI of ≥3 months. In cohorts A and B, ORR was 8.1% (95% CI: 5.2–11.9) and 9.9% (95% CI: 4.6–17.9), respectively. Responses were durable and typically lasted ≥6 months. Median OS was 18.7 months overall, with a trend toward a longer OS in patients with higher programmed death-ligand 1 (PD-L1) expression.
In contrast to pembrolizumab, the addition of an ICI atezolizumab to chemotherapy and niraparib failed to demonstrate statistically significant PFS benefits for patients with recurrent ovarian cancer in the ANITA trial, with a median PFS of 11.2 months compared with 10.1 months among patients treated with placebo in place of atezolizumab and no improvements in PFS regardless of PD-L1 status.37
Bevacizumab, a monoclonal antibody targeting vascular endothelial growth factor (VEGF), has also gained traction as a valuable addition to PARP inhibitor therapy. The combination of bevacizumab with PARP inhibitors has shown improved PFS and OS in recurrent ovarian cancer patients. As mentioned above, the phase III PAOLA-1 trial26,27 investigated the combination of olaparib and bevacizumab as a first-line maintenance therapy in advanced ovarian cancer patients with HRD. The study demonstrated a significant extension in PFS, reinforcing the potential of combining targeted therapies to enhance treatment outcomes.
The phase III DUO-O study evaluated the addition of an ICI durvalumab to the standard upfront chemotherapy with paclitaxel/carboplatin (P/C) plus bevacizumab, followed by maintenance bevacizumab plus durvalumab and olaparib in patients with advanced ovarian cancer without BRCA mutations.38 In an interim analysis, a highly significant increase in PFS in patients treated with durvalumab plus olaparib was observed compared to the standard of care (SoC) regimen. For HRD-positive patients, PFS was 37.3 months in the durvalumab plus olaparib arm versus 23.0 months for those in the SoC arm (HR: 0.49 [95% CI: 0.34–0.69]; p<0.0001). In the intention-to-treat population, PFS was 24.2 months with olaparib compared to 19.3 months with SoC (HR: 0.63 [95% CI: 0.52−0.76; p<0.0001).
New Treatment Options and Future Directions
Emerging therapies continue to enrich the ovarian cancer treatment arsenal. Beyond PARP inhibitors and combination strategies, newer approaches like antibody-drug conjugates (ADCs)39 and small molecule inhibitors targeting other DNA repair pathways40 are under investigation. ADCs like mirvetuximab soravtansine, which targets folate receptor alpha, have shown promise in clinical trials,41 demonstrating the potential for enhanced efficacy and reduced toxicities.
Conclusion
PARP inhibitors, along with the potential of combination therapies involving immunotherapy and anti-angiogenic agents, have catalyzed a paradigm shift in ovarian cancer treatment, introducing personalized therapeutic strategies based on genetic profiles. With the approvals of olaparib, niraparib and rucaparib, ovarian cancer patients now have access to tailored therapies that hold the promise of prolonged disease control and improved survival. As emerging treatment options join the armamentarium, the trajectory of ovarian cancer management is poised to witness further advancements in the quest for more effective and targeted therapeutic solutions. Ongoing research seeks to optimize the use of these agents through combination therapies, identification of predictive biomarkers, and understanding mechanisms of resistance. As our understanding of ovarian cancer biology deepens, PARP inhibitors continue to shine as a beacon of hope in the quest for more effective and targeted ovarian cancer treatment options.
Conflicts of interest
Marcus Vetter received honoraria for serving on advisory boards from AstraZeneca and GSK, honoraria for consultancy from GSK, Roche, Novartis, Exact Sciences, Pfizer, Stemline, AbbVie and ASC Oncology, and grant support from GSK. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way. Viola Heinzelmann has declared that the manuscript was written in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors have declared that no financial support was received from any organization for the submitted work.
Author contributions
All authors contributed to and approved the final manuscript.