Introduction
In Switzerland, approximately 6,300 women and 50 men are diagnosed with breast cancer (BC) every year.1 BC is a heterogeneous disease that can be divided into separate subtypes. The majority of BCs are human epidermal growth factor receptor 2 (HER2)-negative, and this subtype can be separated into hormone receptor (HR)-positive or triple-negative breast cancer (TNBC), which is rarer and accounts for approximately 10−15% of cases.2,3 Between 5% and 10% of HER2-negative patients harbor a germline mutation in one of the two breast cancer suppressor genes, BRCA1 or BRCA2.4 Among all BRCA1/2 mutation carriers, HER2-positivity is found in 10% for BRCA1-associated BC and 13% for BRCA2-associated BC.5,6 BRCA1 and BRCA2 are located on chromosomes 17 and 13, respectively, and encode for proteins that repair DNA damage and ensure cell integrity.2 Women with a germline BRCA1 or BRCA2 mutation (gBRCA1/2m) have a markedly increased risk of developing early-onset BC.7 The lifetime risk for women with a gBRCA1/2m caused by a BRCA1 or BRCA2 pathogenic variant is estimated to vary between 60‒85%.7–11 Therefore, testing BRCA1 and BRCA2 status in healthy individuals with a strong family burden plays an established predictive role in BC risk assessment.12
Among individuals already diagnosed with BC, gBRCA1/2 testing follows similar rules. To increase the probability of detecting a gBRCA1/2 mutation, testing is performed selectively by applying criteria such as subtype of BC, family history and age. This approach, however, can result in a significant number of BC patients with gBRCA pathogenic variants being missed due to restrictive testing criteria in current guidelines.12 In addition to establishing risk, determining BRCA1/2 status has a broader role in treatment decision-making. For example, detection of gBRCA1/2m in individuals already diagnosed with BC is clinically relevant to predict responsiveness to platinum-based chemotherapy in the metastatic setting, as well as to inhibitors of poly(ADP-ribose) polymerase (PARP), owing to the ability of these interventions to inhibit DNA repair pathways in early and advanced breast cancers.13 Notably, among existing PARP inhibitors (PARPi), currently, only olaparib was assessed in a phase III clinical trial in early BC and is approved in Switzerland among other countries for treating early high-risk BC patients with gBRCA1/2m.14,15
This review provides a summary of existing unmet needs/challenges as well as opportunities and possible solutions in preventive, surveillance and treatment strategies for individuals with gBRCA mutations in Switzerland.
Rationale for targeting BRCA1/2 and opportunities for testing BRCA1/2 status
BRCA1 and BRCA2 proteins are involved in various molecular processes related to DNA metabolism, including homologous recombination and mediation of the replication stress response.16 Somatic and germline BRCA1/2 mutations pose significant risks to genome integrity and markedly increase the risk of several cancers, particularly breast and ovarian cancer in women.2 Although gBRCA mutation carriers are more susceptible to BC, the same DNA repair defect increases tumor sensitivity to treatments relying on the induction of DNA damage, such as platinum-based chemotherapy and radiotherapy, as well as PARP inhibition.2 In particular, PARPi prevents DNA damage repair in cells harboring a deficiency in homologous recombination repair (HRR), including mutations in BRCA1/2.17 Therefore, timely determination of gBRCA mutational status is critical to achieving an effective treatment strategy.18 Accordingly, there are two different rationales for gBRCA1/2 testing: (1) prevention testing in healthy individuals aiming to estimate their future risk of cancer and (2) predictive testing in individuals diagnosed with cancer to make treatment decisions. However, gBRCA1/2 testing also has implications for healthy family members of mutation carriers.
BRCA mutations in BC have a different prevalence depending on the subtype, as determined by the estrogen receptor (ER), progesterone receptor (PR) and HER2. The status of these three biomarkers is routinely tested in clinical practice to classify breast tumors and determine potential treatment strategies. BCs can be classified into four main subtypes as luminal A-like (ER-positive [PR-positive], HER2-negative and low proliferation [Ki 67-negative]); luminal B-like (ER-positive [PR-positive], HER2-negative or HER2-negative or positive and high proliferation [Ki 67-positive]); HER2-over-expression (ER-negative [PR-negative] and HER2-positive); triple-negative (ER-negative [PR-negative] and HER2-negative).19,20 BRCA1 mutations are often associated with TNBC, whereas BRCA2 mutations are more frequently associated with HR-positive tumors.21 Interestingly, in BC patients with BRCA2 mutations, ER expression does not predict superior survival, and limited benefit from endocrine therapies has been hypothesized.20 However, some data suggest that long-term survival for gBRCA2m patients with HR-positive/HER2-negative BC is worse than for patients without mutations.22,23 A recent real-world study reported that 10% of HER2-negative metastatic breast cancers (mBC) have a germline mutation in BRCA1 and/or BRCA2.17 gBRCA mutations are also more frequent in younger HER2-negative individuals (aged ≤50 years at initial breast cancer diagnosis) compared to older individuals (12.9% vs 5.4%, respectively),17 and in individuals with a strong family history of BC and/or ovarian cancer compared to those without (22.7% vs 6.6%).17
BRCA1/2 testing is traditionally reserved for BC patients with a significantly high risk of being a carrier (about 10% of BC cases), e.g., younger age at diagnosis (<40–45 years), TNBC in individuals younger than 60 years or a specific family history of breast and/or ovarian cancer.24 Moreover, it is often restricted by guidelines and curtailed by sequencing costs.25 Despite an increasing trend in gBRCA testing in recent years due to advances in multigene panel testing and next-generation sequencing (NGS) techniques, some studies estimate that up to 50% of BC patients with gBRCA pathogenic variants could be missed due to restrictive recommendations for testing in current guidelines, i.e., BC patients that may benefit from newer risk-reduction strategies remain untested.18,24 Moreover, identifying a pathogenic BRCA mutation in a woman already diagnosed with BC influences her treatment strategy and might decrease recurrence and prevent new primary tumors. A retrospective cohort study by Lynce et al. (2023) evaluated the Oncotype DX Breast Recurrence Score® (ODX RS) genomic test, a 21-gene prognostic and predictive assay.18,26 The authors noted that HR-positive, HER2-negative BC patients with a BRCA mutation have a higher score, meaning a higher risk of BC recurrence compared to those with gBRCA wild type. Notably, two-thirds of HR-positive, HER2-negative early BC patients in this study did not undergo genetic testing, including 351 patients with high ODX RS who may benefit from newer risk-reducing strategies.18 A cost-effectiveness study by Wu et al. (2022) reported that gBRCA testing for all patients with HER2-negative BC, including TNBC and HR-positive HER2-negative BC, intending to offer adjuvant PARPi to high-risk patients with a pathogenic variant in BRCA1 or BRCA2, is cost-effective and has a clinical benefit.27
Overview of PARP inhibition in BC
PARP polymerases are a family of related enzymes that share the ability to catalyze the transfer of ADP-ribose to target proteins.28 PARP1 and PARP2 are enzymes activated by DNA damage and play a key role in DNA repair pathways. PARP inhibition leads to stalled DNA replication forks and the accumulation of single-strand breaks (SSBs).28 Consequently, in BRCA-mutated cells, since the capacity for HRR has been lost, cytotoxic double-strand breaks (DSB) accumulate, leading to genomic instability and cell death,28,29 a phenomenon referred to as synthetic lethality.
Three PARP inhibitors, olaparib, niraparib and rucaparib have been approved by the European Medicines Agency (EMA) to treat high-grade ovarian, fallopian tube or primary peritoneal cancers in women with BRCA mutations.30 In addition, olaparib is approved by the EMA and Swissmedic for various other indications, including early-stage BC with gBRCA mutation, HER2-negative mBC with gBRCA mutation, adenocarcinoma of the pancreas, ovarian cancer and prostate cancer.14,31 A fourth PARPi, talazoparib, is also approved by the EMA as monotherapy for the treatment of adult patients with gBRCA1/2 mutations who have HER2-negative, locally advanced or metastatic BC previously treated with an anthracycline and/or a taxane. However, olaparib is the only PARP inhibitor available to treat early BC.14 Olaparib monotherapy is approved by Swissmedic as an adjuvant treatment in adult patients with gBRCA-mutated HER2-negative, early high-risk breast carcinoma who have been previously treated with neoadjuvant or adjuvant chemotherapy, as well as to treat patients with HER2-negative mBC with a gBRCA mutation who have been previously treated with an anthracycline and a taxane (unless contraindicated) in either a neoadjuvant, adjuvant or metastatic setting.14 Notably, patients with HR-positive BC should have shown progression with appropriate prior endocrine therapy or be considered unsuitable for endocrine treatment.14
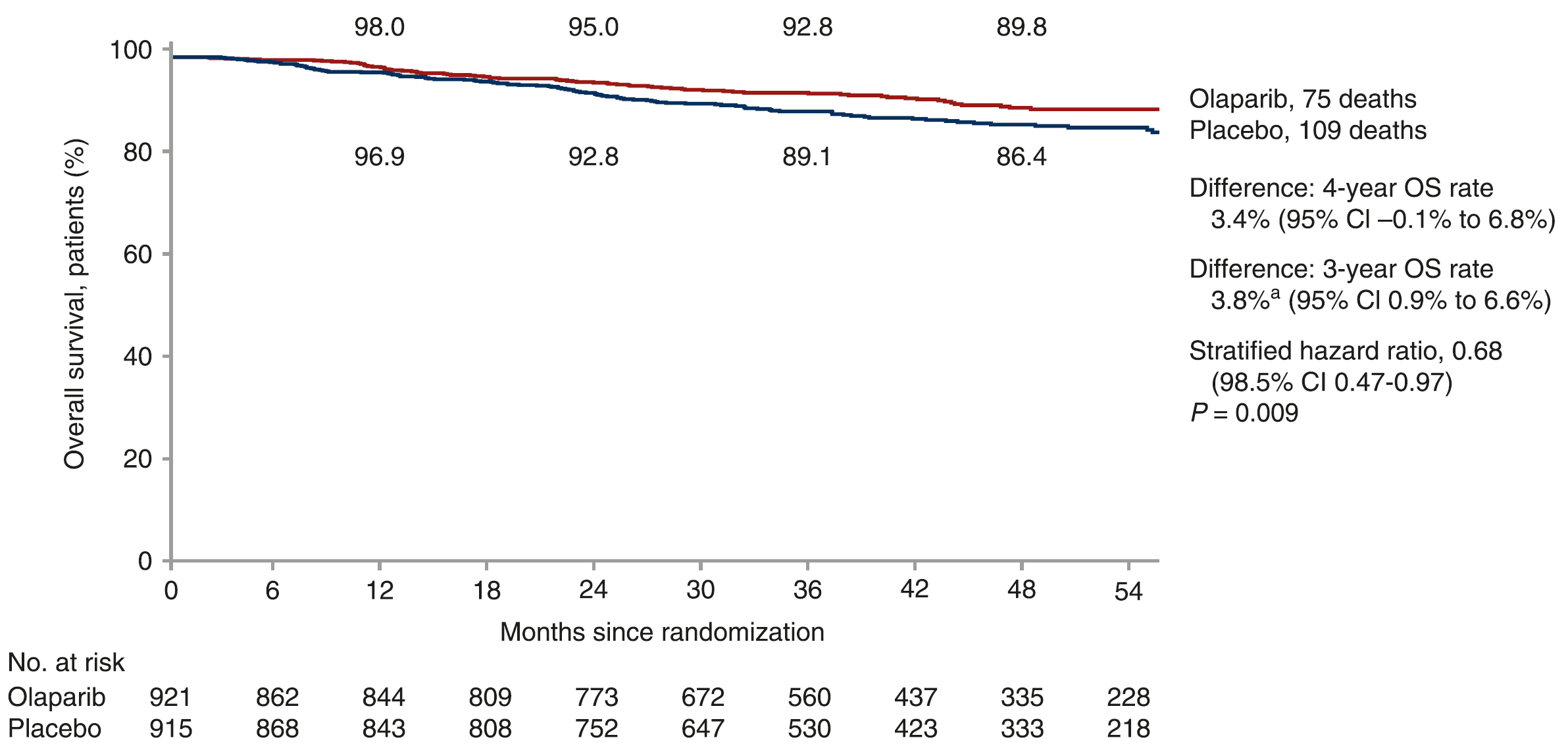
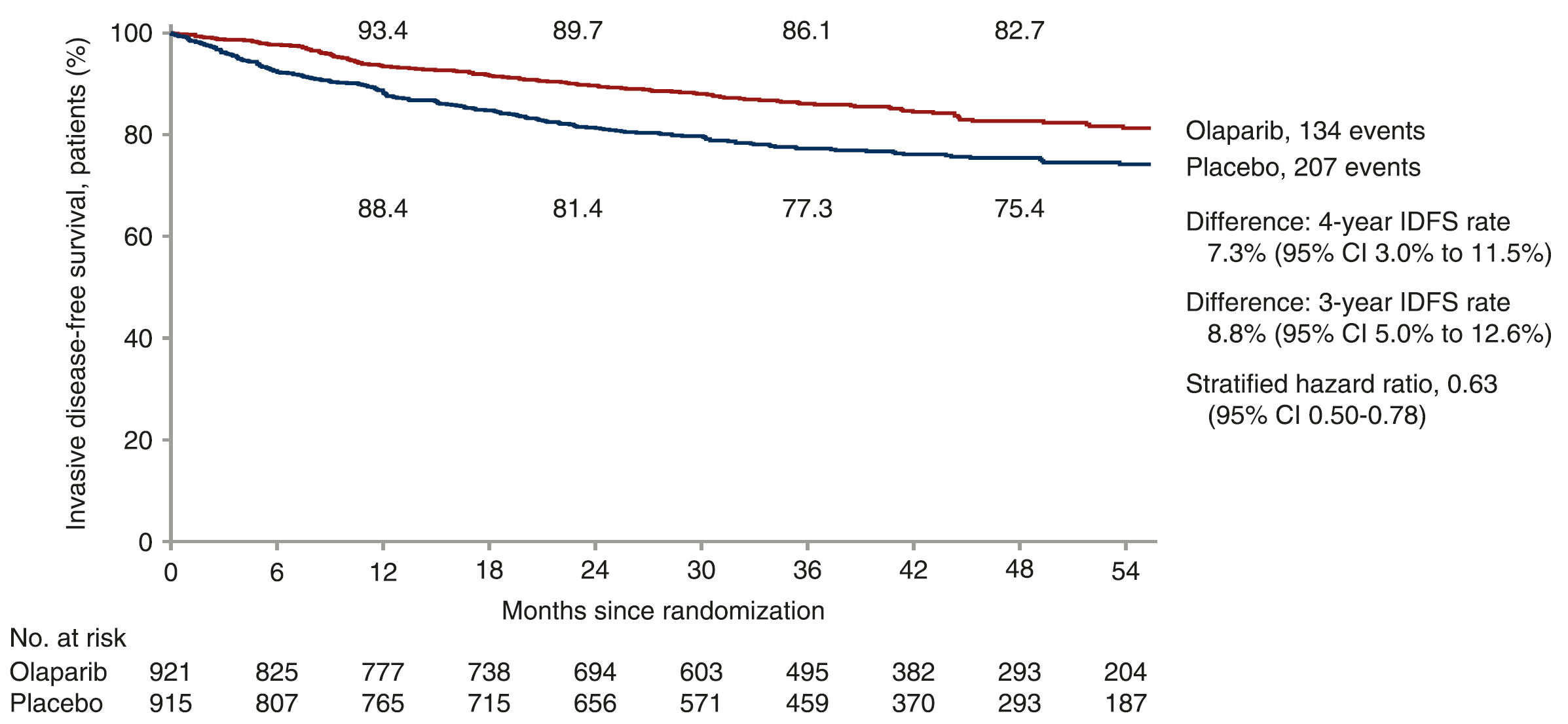
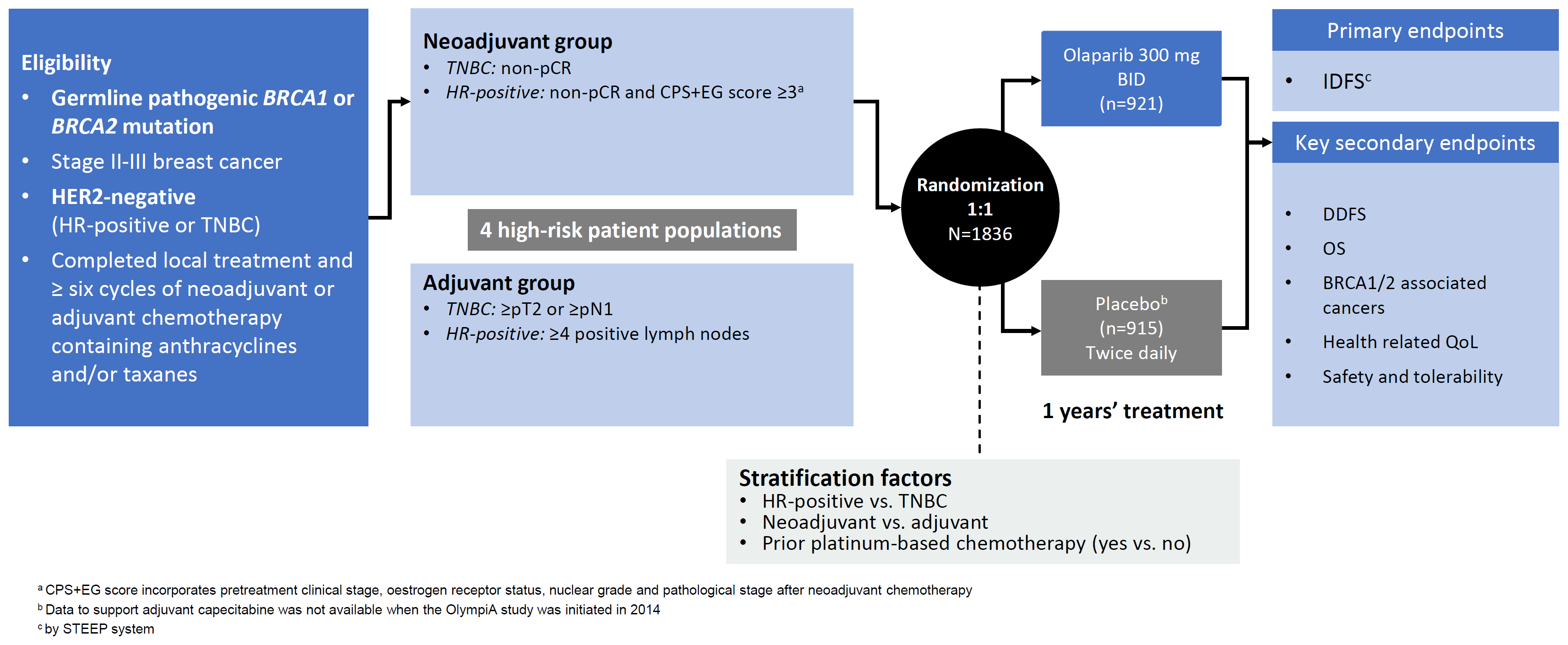
Table 1 summarizes the phase III clinical trials with PARPi in gBRCA-mutated BC. OlympiA (NCT02032823) is a randomized, double-blind, parallel-group, placebo-controlled, multicenter, phase III study comparing olaparib to placebo in patients who completed locoregional treatment, radiotherapy when indicated and neoadjuvant or adjuvant chemotherapy.15 It is the only phase III trial evaluating PARPi in early gBRCA-mutated BC that is completed and shows better invasive disease-free survival (iDFS), distant relapse-free survival (DRFS) and overall survival (OS) in the overall study population following one-year olaparib treatment compared to placebo.15 At a median follow-up of four years, results from a second prespecified event-driven interim analysis showed that olaparib significantly improved OS with a 32% reduction in risk of death compared to placebo (HR: 0.68 [98.5% CI: 0.47−0.97]; p=0.009), yielding a 3.8% absolute improvement.32,33 Four-year OS was 89.8% in the olaparib group and 86.4% in the placebo group (3.4% absolute improvement [95% CI: -0.1% to 6.8%]) (Figure 1). Four-year iDFS demonstrated a 7.3% improvement in the olaparib group compared with the placebo group (Figure 2). Following the results from OlympiA, several questions were raised, including how to incorporate PARPi into the standard management of early-stage BC and other future directives for PARPi in BC treatment and prevention. OlympiA results are practice-changing since they highlight the importance of broader genetic testing, i.e., the results underscore how olaparib should be offered to early BC patients meeting the entry criteria for the study (Figure 3).15,32 Real-world data reported by Andersen et al. (2023) also provides evidence for broadening BRCA testing to HER2-negative early BC patients.34 This cohort study examined patient characteristics, treatment patterns and OS by gBRCA status among 19,258 women with HER2-negative early BC in a U.S. community oncology setting.34 Among the 7.5% with a documented gBRCA test result, 10% were identified with gBRCA mutations.34
_of_adjuvant_olaparib_in_patients_with_g*brca1*_2_pathogeni.png)
_of_adjuvant_olaparib_in_patients_with_g*br.png)

Guidelines and recommendations for gBRCA1/2 testing and treatment – the status quo
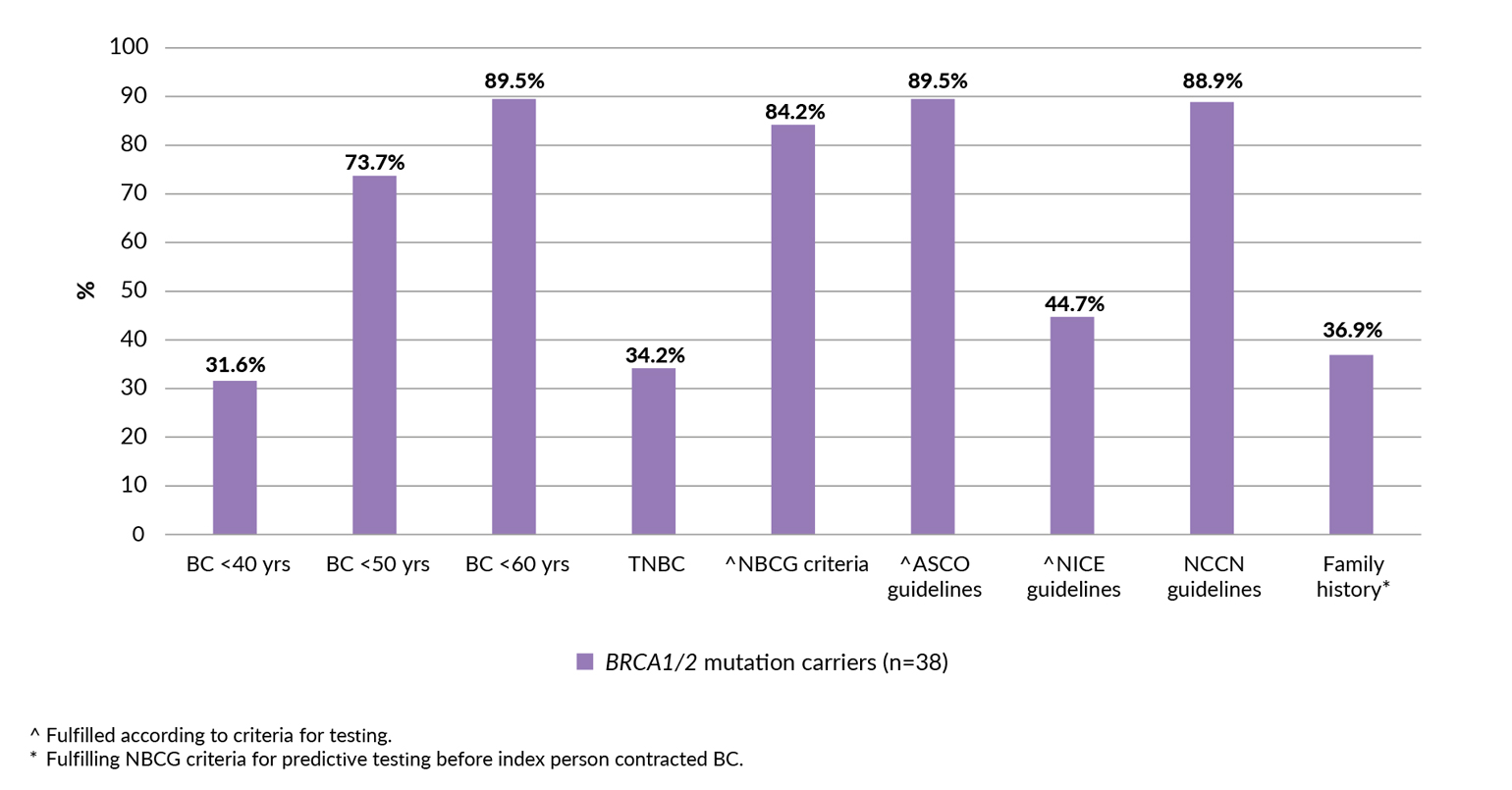
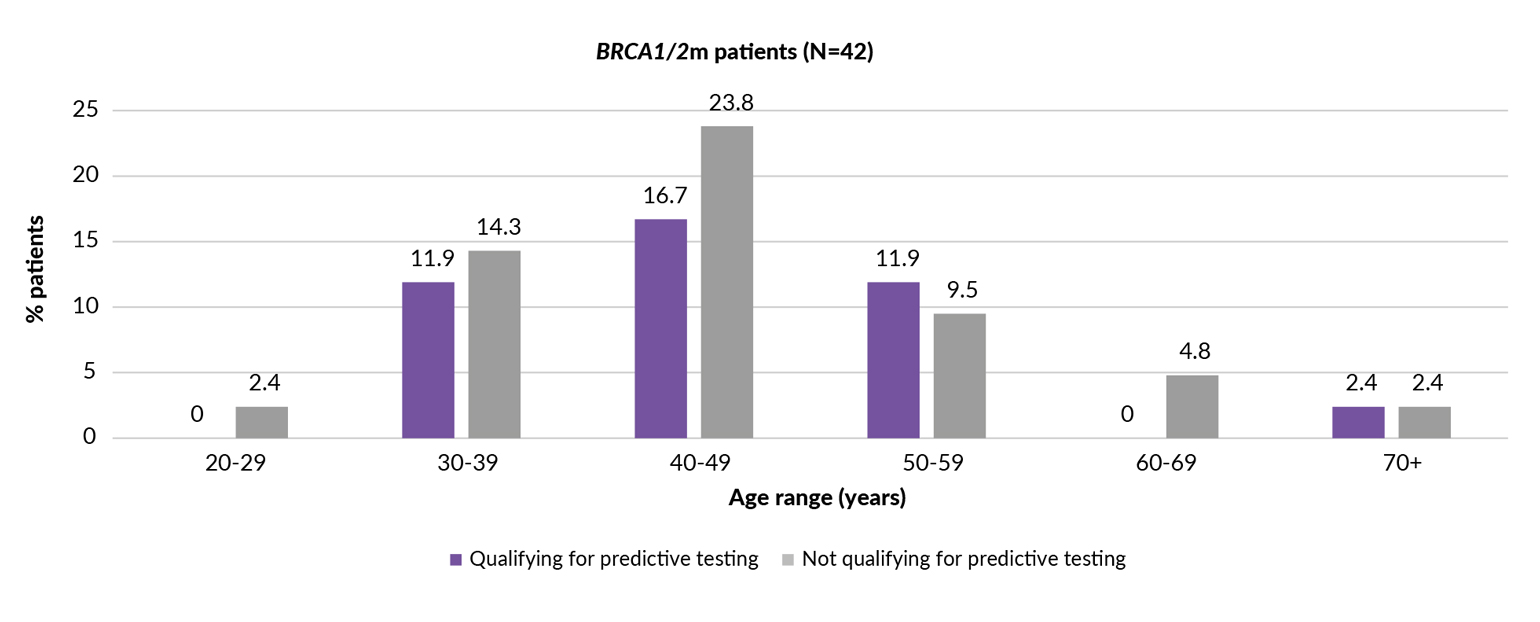
Traditionally, genetic testing for gBRCA1/2 was performed as a preventative measure using defined clinical criteria that maximized the probability of finding a disease-causing variant.35 More recently, therapeutic indications for testing gBRCA1/2 mutations in hereditary breast and ovarian cancer (HBOC)-associated tumors have emerged, leading to a lower threshold and evolved clinical criteria for testing. In addition to a strong family history suggestive of gBRCA1/2 mutation, BC patients at an unusually young age or with TNBC are also considered. Moreover, NGS has revealed additional causative genes of HBOC syndrome with varying degrees of risk.35 However, due to the high costs and capacity issues of testing as well as other potential factors (e.g., hereditary impact, emotional impact, etc.), recommendations on testing for gBRCA1/2 status in guidelines remain primarily restricted to BC patients having a significant risk of being a carrier.12,36,37 It is important to note that only 37% of BRCA1/2 carriers actually have a family history of cancer to qualify for predictive BRCA testing (Figure 4).24 Based on the OlympiA trial outcomes, any newly diagnosed BC patient who meets the trial’s eligibility criteria should be offered germline testing to identify those who might benefit from olaparib.38 Many international, national and local guidelines for genetic testing for HBOC syndrome are available.36,37,39–48 Significant inter-guideline heterogeneity in relation to thresholds for genetic testing and treatment recommendations exists. For example, despite positive outcomes with olaparib in the OlympiA trial, only five guidelines recommend genetic testing today to help decision-making for targeted therapy with PARPi agents in HER2-negative BC (Table 2). Moreover, only three of these guidelines recommend testing criteria for both predisposition of genetic disease and therapy decision (Table 2).
.__2.jpg)
The European Society for Medical Oncology (ESMO) 2020 guidelines acknowledge that family history-based testing misses about half of HBOC syndrome gene carriers.36 Moreover, ESMO encourages the development of strategies to identify high-risk HBOC individuals.36,37 Some healthcare professionals (HCPs) submit tumor tissue from BCs for assessment of somatic mutations of BRCA2 by NGS. However, this strategy can also miss some patients with gBRCA1/2 mutations. Notably, the use of PARPi, based on results from the OlympiA study, is only indicated if a gBRCA1/2 mutation is detected. The concept of testing for guiding therapy is different from genetic counseling for predisposition to breast, ovarian, pancreatic and prostate cancer. A Swiss guideline is in place; however, this guideline cannot be used to evaluate testing for therapy decisions.41 There is currently a clear unmet need for international alignment on genetic testing to optimize outcomes for all BC patients.
Current challenges (and possible solutions) in defining high-risk in early BC
Different definitions of ‘high-risk’ for recurrence have been used in pivotal BC clinical studies.15,49 Today, we have to use the inclusion criteria in the OlympiA trial for testing patients for BRCA1/2 mutation and adjuvant olaparib treatment, i.e., testing is reserved for HER2-negative TNBC or HR-positive individuals with completed breast and axilla surgery, and those who complete at least six cycles of neoadjuvant or adjuvant chemotherapy.15 Also, participants in the OlympiA study had axillary lymph node dissection to define the number of positive lymph nodes; however, this surgical procedure is no longer standard practice. Current guidelines for BRCA1/2 testing of BC patients are mainly focused on detecting genetic predisposition and not to guide therapy. Swiss guidelines from the Network for Cancer Predisposition Testing and Counseling (CPTC) of the Swiss Group for Clinical Cancer Research (SAKK) recommend testing based on criteria for genetic predisposition alone.41 Using the same testing criteria, a Norwegian study highlights that many BRCA1/2 carriers with a pathogenic mutation can be missed when testing for predisposition of genetic disease without considering treatment decision (Figure 5).24 This study highlights that more than 50% of BRCA1/2 carriers with a pathogenic mutation from a Norwegian cohort did not qualify for testing based on criteria for predisposition of genetic disease (Figure 5).24 In contrast, the 2021 St. Gallen International Consensus Guidelines recommend testing to target therapy with PARPi.42 However, the more recent 2023 St. Gallen International Consensus Guidelines update for the treatment of primary BC discussed the impact of genetics on adjuvant therapy, but a consensus was not reached for universal genetic testing for all BC patients.50 Identifying patients eligible for therapeutic testing beyond hereditary risk assessment criteria is needed.24 Moreover, the National Comprehensive Cancer Network (NCCN) U.S. guidelines recommend, in accordance with the eligibility criteria of the OlympiA trial, adjuvant PARPi therapy for all TNBC patients with non-pathological CR (pCR) and pathological tumor or node staging ≥pT2 or ≥pN1, respectively, and for all HR-positive BC patients with non-pCR and CPS+EG (pre-treatment clinical [CS] and post-treatment pathological stage [PS], ER status [E] and grade [G]) score ≥3 and positive BC with upfront surgery and ≥pN4.51
_qualifying.jpg)
Achieving insurance coverage for genetic testing also remains challenging, and obligatory testing for therapy versus for predisposition is an argument relevant for health insurance companies. Health insurance guidelines may not meaningfully differentiate between patients with cancer who are likely to benefit from germline cancer genetic testing and those who will not.52 Some health insurers might reject reimbursement requests for genetic testing because they do not consider treatment to be associated with testing intent. A recent study reported that while payers define high risk based on the OlympiA trial definition (i.e., clinical and pathologic stage, lymph node involvement, tumor grade and size and ER status), healthcare providers adopt a broader definition to include genomic risk scores.22 Additional challenges that may impact universal genetic testing include the provider’s knowledge and comfort with guidelines, testing and timing of gBRCA tests in relation to first-line treatment (i.e., especially for HR-positive patients).53 Real-world evidence highlights that germline testing is underutilized and offered to fewer than half of patients with BC who meet the criteria for testing.54–59 There is an urgent clinical need to clearly identify women whose tumors harbor deleterious BRCA mutations early in their cancer treatment journey to maximize the number of women afforded the opportunity to benefit from a PARPi upon completion of (neo)adjuvant chemotherapy. Therefore, testing should be considered by the whole multidisciplinary team and initiated rapidly. Moreover, not testing or providing the best treatment for high-risk patients in a curable setting is an ethical issue that requires further discussion.
Systemic bottlenecks such as the limited capacity of genetic counselors (in some countries) and the creation of improved workflows are inherent problems.60 Improving current rates of genetic counseling/testing remains a significant challenge.24,59,61–63 Further studies are required to determine how many patients that should be tested are missed. Educating Swiss oncologists and gynecologists about the implications of genetic testing (e.g., Swiss Group for Clinical Cancer Research [SAKK] courses) might help to speed up counseling referral and targeted treatment in Switzerland. Variations in genetic testing exist among racial and ethnic groups.64 Historically, carriers of pathogenetic variants among specific ethnic groups have been subject to different forms and degrees of genetic discrimination, and many individuals at risk have forgone BRCA testing to avoid potential discrimination.65 Although there are no quick solutions and profound cultural, legal and regulatory changes are required to create understanding and acceptance of all differences, changes by the scientific and medical community, together with patients and the public, can help tackle the issue of genetic discrimination in genetic testing.65
Conclusions and future outlook
Access to genetic counselling, testing and PARPi treatment must be guaranteed for all patients who fulfil the OlympiA inclusion criteria. Notably, the definition of ‘high risk’ used in the OlympiA trial is not exhaustive. And especially the required number of involved lymph nodes for the HR-positive/HER2-negative population within OlympiA are not in line anymore with the changed threshold for sentinel lymph node biopsy. Indeed, many patients would require axillary lymph node dissection for a treatment decision despite it not being helpful as a surgical treatment. Therefore, in addition to the OlympiA study entry criteria, individual decisions within the interdisciplinary team are needed. Adequate genetic testing, as well as training and qualifications for multidisciplinary team members, are crucial for the success of the BC patient care journey.
Conflicts of interest
CL: Advisory Boards/Advisory for AstraZeneca, Roche, MSD, Daiichi-Sankyo, Gilead, Novartis, Pfizer, Seagen, Exact Sciences. CK: Consulting Fees from GSK, Astra Zeneca, Novartis, Roche, Eli Lilly S.A., Pfizer, Genomic Health, Merck MSD, Novartis, PharmaMar, Tesaro; Advisory Boards for GSK, Astra Zeneca, Novartis, Roche, Eli Lilly S.A., Pfizer, Genomic Health, Merck MSD, Novartis, PharmaMar, Tesaro; Travel Support from GSK, Astra Zeneca, Roche. JH: Research Support for Lilly; Lecturing activities for Lilly, Novartis, Roche, Pfizer, AstraZeneca, MSD, Seagen, Gilead, Daiichi; Consulting activities for Lilly, Novartis, Roche, Pfizer, AstraZeneca, Daiichi, Gilead; Travel Support from Roche, Pfizer, Daiichi, Gilead. MV: Advisory Boards for AstraZeneca and GSK; Consulting Fees from GSK, Roche, Novartis, Exact Sciences, Pfizer, Stemline, AbbVie and ASC Oncology; grant support from GSK. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way. KS, RC, NB and KZ declared that they do not have any conflict of interest and that they have no financial relationships with any organizations that might have an interest in the submitted work.
Funding
Preparation of this article was financially supported by AstraZeneca AG. AstraZeneca did not have any decision-making role in the development of the manuscript and did not influence its content in any way.
Acknowledgments
We thank Dr Ellen Heitlinger, H+O communications Ltd., Zurich, Switzerland for her medical writing support of the manuscript (including writing, language editing, referencing, formatting and proofreading).
Author Contributions
All authors contributed to and approved the final manuscript.