Introduction
Breast cancer remains the most common malignancy and the most frequent cause of cancer death among women worldwide, with over 2.3 million new cases (11.7% of all new cancer cases) and over 685,000 deaths each year, accounting for almost 7% of global mortality due to cancer.1 In 2020, breast cancer accounted for 24.5% of all cancer cases among women and 15.5% of all female cancer deaths, which classifies this disease as the leading cause of death in female populations worldwide.2
Over 80% of related fatalities are due to the development of therapy-resistant metastatic disease.3 Therefore, national efforts have been concentrated on developing early diagnostic and screening strategies. In the last 15 years, state-driven healthcare policies have led to the implementation of nationwide screening programs resulting in increased diagnosis rates, particularly among early-stage breast cancer cases. Together with lately amplified breast cancer risk factors (such as decreasing fertility rate, increasing hormonal therapy and/or contraceptive use, shorter breastfeeding time and increasing body weight), this resulted in a significant increase in breast cancer cases, creating a necessity for the development of new risk stratification and management tools.2
While the main predictive and prognostic factors rely heavily on intrinsic tumor features, such as size, lymph node involvement and extent of tumor spread (all incorporated into the American Joint Committee on Cancer [AJCC] Tumor, Node and Metastasis [TNM] staging system), other biological characteristics with predictive value, including tumor grade, histologic type, proliferation index, biomarker expression and molecular expression profiles, are also used to define and classify types of breast cancers according to clinical risk. These features have become core drivers of prognostic algorithms (e.g., Adjuvant! Online) and indices (e.g., the Nottingham Prognostic Index).4 As such, the latest TNM Update published in January 2018 included biomarkers, like estrogen receptor (ER), progesterone receptor (PR) and HER2 expression and histological grade, which are frequently used in daily clinical practice to help with risk and treatment assessment.
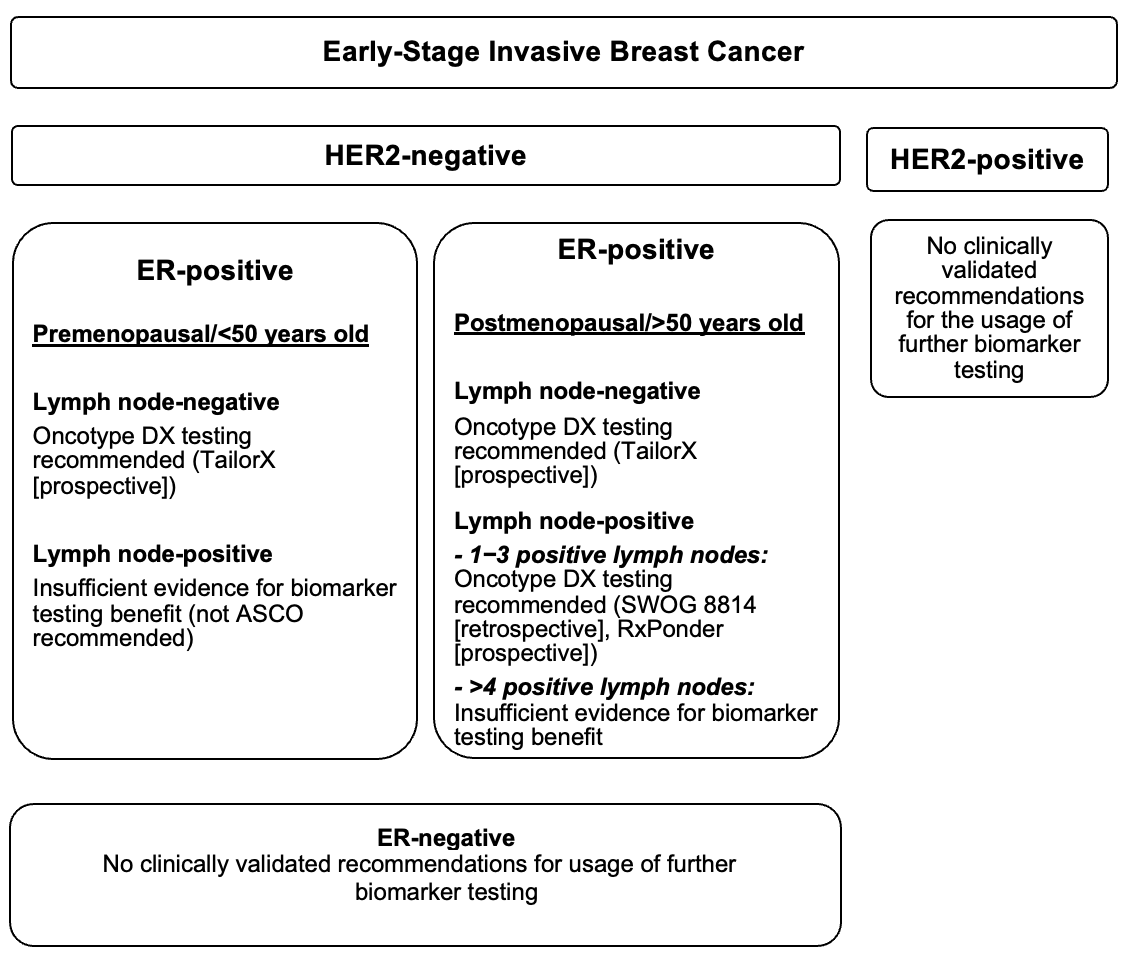
To reduce the burden of chemotherapy administration for both patients and healthcare providers, new prognostic tools emerged. In particular, genetic signatures have already been introduced into clinical practice to help guide adjuvant chemotherapy.5 Shortly after their validation through clinical retrospective and prospective trials, these novel prognostic assays were also incorporated into international breast cancer guidelines, including the American Society for Clinical Oncology (ASCO)6 (Figure 1) and the St. Gallen International Expert Consensus Guidelines.7 The latest TNM system update includes prognostic genomic assays, such as MammaPrint and Oncotype DX, which led to the creation of specific TNM prognostic stage groups. For example, HR-positive, HER2-negative, T1−2, N0 tumor will currently be considered stage IA, irrespective of tumor size, when the Oncotype DX Recurrence Score (RS) is in the low range.8 This new risk conceptualization led to the optimization of treatment, particularly for early luminal breast cancer, and pushed further the trend of personalized medicine.

This article aims to provide a current literature review on the role of Oncotype DX testing in breast cancer patients in the daily clinical setting, with a focus on the main prospective and retrospective trials leading to the validation and incorporation of RS in the main breast cancer guidelines currently in place. This is a literature review-based work that assessed various peer-reviewed original articles, review articles, regulatory communications and retrospective and prospective trial studies.
Development of prognostic multigene assays in breast cancer
In early luminal breast cancer, standard treatment after resection and radiation therapy includes endocrine therapy with an aromatase inhibitor (AI), gonadotropin-releasing hormone (GnRH)-analog/AI or tamoxifen.9 The treatment decision regarding chemotherapy has been traditionally based on histopathological characteristics, such as grading, Ki-67, ER and PR expression levels, and disease stage.10 Based on prior prospective studies, the need for additional chemotherapy in patients with low-risk breast cancer (e.g., node-negative) has also been considered. However, since in low-risk breast cancer patients treated with single-agent tamoxifen therapy the estimated recurrence risk at 10 years is below 15%, in order to avoid overtreatment, the role of additional adjuvant chemotherapy needed to be determined. As a result, genomic assays were developed at the beginning of the 21st century.11
Genomic assays were introduced by van’t Veer and colleagues in 2002 as an alternative to pathology reports lacking consistency, allowing for more precise prognosis stratification.12 Many of them have been created based on complementary or copy DNA (cDNA), oligonucleotide arrays and multiplex polymerase chain reactions (PCR). Tests such as 21-gene Oncotype DX (Genomic Health, Redwood City, CA), 70-gene MammaPrint (Agendia BV; Amsterdam, the Netherlands; also referred to as the “Amsterdam signature”), 12-gene EndoPredict (Myriad Genetics, Salt Lake City, UT)13 and PAM50 (patented to NanoString, Seattle WA) emerged to identify those tumors that substantially benefit from additional chemotherapy.14
These genomic tests assess markers of proliferation and invasion, as well as ER and HER2 status, and subsequently provide a numerical score of prognostic and predictive value, which could be used in therapy planning. In the past decade, this has constituted a pivoting point in personalized cancer care. In particular, the Oncotype DX RS has increasingly gained momentum and is now broadly used in triaging patients eligible for chemotherapy worldwide.
Oncotype DX prognostic assay: the background
The Oncotype DX was adopted into practice shortly after its publication in 2004. The assay was created based on the expression of 250 genes, quantified by reverse transcriptase PCR (RT-PCR) using microRNA (mRNA) from 447 different tumor samples from the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-20 study.15 In total, 16 genes were selected based on statistical association with breast cancer recurrence. These genes regulate estrogen signaling, proliferation, HER2 amplification, cell invasion, tumor-associated macrophages (CD68), detoxification (GTSM1) and chaperone protein binding (BAG-1, co-chaperone for HSP70 involved in BCL-2 expression). Five more housekeeping genes were added to create an algorithm generating a score of recurrence.16
A recent analysis of data from the TransATAC study of 785 ER-positive, HER2-negative breast cancer biopsy samples showed that variation estimates of residual risk of distant recurrence between different genomic arrays, including Oncotype DX, mainly depend on estrogen or proliferation profile in the algorithm calculation.17 The estrogen module (ESR1, PGR, BCL2, SCUBE2) accounts for almost 60% of the variance in risk stratification and is therefore the key factor for RS. In comparison to other genomic tests, Oncotype DX is largely based on estrogen profile but also utilizes a proliferation threshold, making the correlation between proliferation-related genes and the result more relevant.
The range of RS was set between a value of 0 and 100, with higher scores representing a greater likelihood of disease recurrence. The RS was initially defined as low-risk (<18), intermediate-risk (18−30) and high-risk (>30), based on the results of the NSABP B-20 study.18 Higher scores indicated a higher likelihood of recurrence at 10 years in patients treated with adjuvant tamoxifen therapy alone.16
The Oncotype DX RS algorithm has been subsequently validated in a retrospective analysis of tumor samples stored in the NSABP Tissue Bank from patients treated with tamoxifen in a large prospective U.S. study (NSABP trial B-14).19 Data showed a 10-year rate of distant recurrence of 30.5% in the high-risk group (RS>31), significantly higher when compared with patients in the low-risk (RS<18) and intermediate-risk groups with a recurrence rate of 6.8% and 14.3%, respectively. Based on these findings, Oncotype DX and other signatures have established adjuvant chemotherapy as standard treatment in patients with high RS.15
In 2009, national screening implementation programs debuted across the U.S. and led to a boom in early breast cancer diagnoses. As most of these tumors are ER-positive, HER2-negative and associated with a 5-year survival rate of >94% and a recurrence rate of 15%, the benefit of chemotherapy in this patient population was not clear.20,21 Data analysis from the Surveillance, Epidemiology and End Results (SEER) on the impact of Oncotype DX testing on ER-positive breast cancer patients in the first decade of use found an inverse correlation between the usage of chemotherapy and genomic testing.22 Between 2004 and 2015, the utilization rate of Oncotype DX increased from 1.5% to 34%, with a decrease in chemotherapy usage from 42% to 36% in those who underwent testing. More so, patients who underwent Oncotype DX testing tended to have improved survival when compared with those who did not, even after adjustment for clinical variables. Data also showed that Oncotype DX is a prognostic tool mainly for middle-aged patients and less for older patients. Consistent with the Oncotype DX testing recommendations, the use of adjuvant chemotherapy increased in high-risk groups and decreased in the intermediate and low-risk groups. Further analysis indicated a massive reduction of approximately 80% in breast cancer-specific risk of death among patients who underwent testing. Results also demonstrated that Oncotype DX is widely used in the clinical setting for risk stratification and the utilization of the test remained almost double in lymph node-negative versus lymph node-positive breast cancer patients.
Since its introduction to clinical practice, the ASCO (Figure 1),6 the National Comprehensive Cancer Network (NCCN),9 the European Society for Medical Oncology (ESMO),23 the National Institute for Health and Care Excellence24 and the St. Gallen Consensus Conference7 have included Oncotype DX into their breast cancer guidelines. In the U.S., Medicare has been funding Oncotype DX screening for its beneficiaries since 2006.25
Validation of Oncotype DX
Initially intended as a prognostic/predictive tool for ER-positive, lymph node-negative tumors, the use of Oncotype DX has been progressively extended to different breast cancer patient populations (Figure 1).16 Although current NCCN guidelines for Oncotype DX testing refer to patients with ER-positive, early-stage, lymph node-negative tumors,9 there is a trend toward increased Oncotype DX screening among those with more advanced, lymph node-positive tumors. Prognostic value on Oncotype DX in lymph node positive breast cancer patients was initially shown in the TransATAC study, where postmenopausal women with node negative and node positive disease on one endocrine agent alone or on combinations of tamoxifen and aromatase inhibitors, had distant recurrence rate in the low, intermediate and high RS categories, at 9 years of 4%, 12% and 25% in the N0 group and 17%, 28% and 49% in the N+ group respectively.26 More recent findings indicate a clear added value for patients with ER-positive, HER2-negative, lymph node-positive breast cancer with an RS <25 who undergo chemotherapy.27 When referring to tumor stage, a significant benefit was observed for both late- and early-stage disease; however, late-stage cancers tended to have a lower hazard ratio when compared with early-stage.22 Clinical benefit seemed to be uniform across lymph node status and HER2 expression. Prescription of chemotherapy led to an overall death risk reduction of 40% in high-risk patients and a 25% reduction in intermediate-risk patients compared with patients who had no chemotherapy, without clear benefit in the low-risk group. More recently, large, randomized clinical studies have demonstrated the beneficial role of chemotherapy in patients with high- and intermediate-risk disease with certain risk factors, such as early age, attained menopause and intermediate- and high-risk RS.11
The prediction of chemotherapy advantage was initially evaluated in the prospective-retrospective NSABP B20 trial studying tumor samples from 651 patients.28 The 10-year DFS rate in patients with high RS was 62% with endocrine therapy alone versus 88% with the addition of chemotherapy (cyclophosphamide with or without methotrexate and fluorouracil). These results were concordant with the B14 study findings, which showed an overall distant recurrence-free survival rate of 70% at 10 years in women who received only endocrine therapy.15 Altogether, RS appears to be prognostic for distant recurrence, with increased recurrence rates for higher RS and predictive of response to additional chemotherapy.29
Early Breast Cancer Trialists Collaborative Group (EBCTCG)
A meta-analysis by the Early Breast Cancer Trialists Collaborative Group (EBCTCG) of data from approximately 100,000 patients enrolled in 123 trials showed that postoperative administration of an anthracycline regimen versus no chemotherapy improved the relapse-free survival (RFS) by 8% and the disease-specific survival (DSS) by 6.5%, accounting for a relative risk reduction of 25%.21 This benefit was maintained regardless of nodal involvement, HR expression, age and administration of endocrine therapy. The addition of taxanes to anthracyclines resulted in a 4.6% absolute increase in RFS and a 2.8% increase in DSS at 8 years, with an additional relative risk reduction of 15%. Among patients receiving a dose-dense chemotherapy regimen (every two weeks), data were even more promising, showing an additional relative risk reduction of 15%. These results were sustained irrespective of clinico-pathological factors, including HR expression. However, in luminal A tumors with low clinical risk, the toxicity rate associated with chemotherapy at about 1−2% does not seem to justify the absolute added benefit of a 3% reduction in recurrence rate.16
Another EBCTCG meta-analysis encompassed 194 clinical trials of hormonal therapy or chemotherapy that started after 1995.30 Data showed that at 15 years, there was almost a two-fold reduction in mortality rate among premenopausal women <50 years of age when compared to postmenopausal women >50 years of age (38% vs 20%). This raised the question of the benefits of chemotherapy-induced ovarian suppression among younger women who usually experience a more aggressive type of tumors. These arguments will be further used in the TAILORx study.
The TAILORx study
Altogether, the EBCTCG data warranted the implementation of genomic screening when selecting patients for endocrine or chemoendocrine therapy.22 While adjuvant chemotherapy may be omitted in patients with low RS, the need for chemotherapy for a high number of patients with intermediate RS remained unclear. The benefit of chemotherapy in patients with intermediate RS was further evaluated in the Trial Assigning Individualized Options for Treatment (TAILORx) study. In this non-inferiority study published in June 2018, a total of 10,273 women with HR-positive, HER-negative, lymph node-negative disease were randomly assigned to receive either endocrine therapy alone or chemoendocrine therapy.31 In the intermediate group (RS: 11−25) (n=6,711), endocrine therapy was non-inferior to chemoendocrine therapy in terms of invasive disease-free survival (DFS) (HR: 1.08 [95% CI: 0.94−1.24]; p=0.26). A subgroup analysis further demonstrated a clear benefit among premenopausal women under 50 years of age who received chemoendocrine therapy, with the added benefit of 3.5% in the RS 11−15 subgroup, 9% in the RS 16−20 subgroup and 6.3% in the RS 21−25 subgroup. Among women in the low RS group (RS<10) (n=1,626) who did not receive chemotherapy, the DFS rate was 84% at 9 years.
Subsequent analyses of TAILORx data assessed the role of further clinical-risk stratification for identifying patients who could benefit from additional chemotherapy.32 It appears that in premenopausal women with intermediate RS and low clinical risk (defined as tumor ≤3 cm and G1, 1−3 cm and G2, or ≤1 cm and G3) the estimated risk for distant recurrence was lower with chemotherapy. Intermediate RS correlated with a higher degree of relapse in the endocrine therapy alone group, irrespective of clinical risk. In patients with higher and lower clinical risk who were randomly assigned to endocrine or chemoendocrine therapy and in patients with high RS (≥26) who received chemoendocrine therapy, the clinical risk was found to be prognostic of distant recurrence independently of RS. These data confirmed that both RS and clinical risk have independent prognostic value on recurrence rate and could be considered separately in age-specific groups. The clinical risk was not found to be a predictor of chemotherapy benefit and should not be used alone in therapy decision-making. Altogether, clinical and pathological features could provide prognostic information about disease recurrence in women with localized breast cancer after surgery but are not predictive of benefit from adjuvant chemotherapy when considered independently of RS.
A secondary analysis of TAILORx evaluated the clinical outcome in 1,389 women with breast cancer with high RS (26−100) who received chemoendocrine therapy.29 The 5-year DFS was 93%, which was better than expected with endocrine therapy alone. In this cohort, the distant recurrence rate with endocrine therapy alone was estimated by combining patient-specific distant recurrence risk with chemotherapy benefit information from the NSABP B20 trial.10 The expected DFS rates without chemotherapy were 78.8% and 65.4% at 5 years and 9 years, respectively. In the overall population, DFS was 87.6% at 5 years and 86.8% at 9 years.29
The selection of the chemotherapy regimen was based on the patients’ age.29 Interestingly, cyclophosphamide/methotrexate and 5-FU (CMF) were mostly administered in older women (median age, 61.5 years), followed by taxanes plus cyclophosphamide or anthracycline without taxanes (median age, 57 years) and anthracyclines plus taxanes in younger women (median age, 53.5 years).
National Cancer Database: High clinical risk breast cancer
Oncotype DX was found to be a useful prognostic tool also in patients with high clinical risk breast cancer. This was shown in an analysis evaluating over 30,000 patients from the U.S. National Cancer Database with pT1−pT2, pN0−pN1, G3 invasive breast cancer, diagnosed between 2010−2015, with RS cut-offs according to the manufacturer’s recommendations.33 From the selected population, 36% of patients had node-positive disease, representing only half of those with node-negative disease (72%). Between 2010 and 2015, the increase in the use of RS testing was documented both in patients with lymph node-negative disease (from 53.2% to 72.3%) but also among patients with lymph node-positive disease (from 16.9% to 36.0%). Data showed that patients with lymph node-positive disease, histologic G3 and high RS benefited significantly from chemotherapy in terms of overall survival (OS) at 5 years (pN0: 12.2% vs pN1: 25.5%). On the contrary, patients with pN1 but low RS did not achieve improved 5-year OS rates (pN0: 2.5% vs pN1: 1%). In patients with intermediate RS receiving chemotherapy, the 5-year OS rate increased by 2.5% among those with node-negative tumors and 7.5% in those with node-positive tumors. Similarly, among patients with G3 tumors and unknown RS who received endocrine therapy plus chemotherapy, unadjusted improvement in the 5-year OS rate was 10.3% in those with node-negative disease (52.2% of the total untested pN0 population) and 20.1% in those with node-positive disease (82.8% of the total untested pN1 population).
This study further demonstrated that tumor grade is prognostic and independently associated with the risk of recurrence but may not correlate strongly with the prognostic provided by RS.33 However, a significantly larger proportion of patients had G3 tumors (N1: 30%; N0: 27.1%) compared with the PlanB trial (18% of the total population)34 and the TAILORx study (17.8% of all tumors; 22% in the original cohort used for the development of RS).15
Studies on lymph node-positive breast cancer
Oncotype DX was also assessed in patients with lymph node-positive tumors adjusted to histologic grade. Data from 4,695 breast cancer patients treated between 2015 and 2018 in Germany were analyzed according to clinical and histological parameters, such as grading, lymph node status, tumor size and Ki-67 proliferation index.35 The RS cut-offs were selected according to TAILORx findings. Patients with lymph node-positive tumors (31% of the total population) had lower tumor grade and lower Ki-67 (<20%) but higher clinical risk and larger size tumors, while lymph node-negative tumor patients (69% of the population) had higher histological grade tumors, Ki-67 and RS. This study comprised a large group of patients with low RS tumors and higher clinical risk features, such as high Ki67 (>20%) or high histologic grade, with no benefit from additional chemotherapy according to data from TAILORx. These results are also supported by the Plan B study, which showed that endocrine therapy alone yielded a 5-year DFS rate of 94% in clinical high-risk patients with low RS (<11).36
MINDACT. Comparable results were also reported in the MINDACT trial on 6,693 women with early-stage breast cancer.37 Among patients with high clinical risk but low genomic risk, the addition of chemotherapy led to an absolute difference for DFS of 0.9% at 5 years and 2.6% at 8 years. In those with low clinical risk and high genomic risk, chemotherapy was associated with a 0.2% and 1.5% difference in DFS at 5 years and 8 years, respectively. No differences in the OS were noted. Updated results showed 8-year DFS rates of 91.7% with chemotherapy and 89.2% without chemotherapy in lymph node-negative patients.38 For patients with 1−3 positive lymph nodes, DFS at 8 years was 91.2% with chemotherapy and 89.9% without chemotherapy.
SWOG-8814. Various other studies assessed the prognostic value of RS for the use of chemotherapy in patients with lymph node-positive disease. Among these, a retrospective analysis of the randomized Southwest Oncology Group (SWOG)-8814 trial on postmenopausal women with lymph node-positive, ER-positive breast cancer showed that chemotherapy failed to improve DFS in 146 patients with RS <18, while there was a trend toward DFS improvement in the intermediate RS group but statistical significance was not reached.39 Furthermore, large retrospective data from the SEER showed better outcomes with chemotherapy in breast cancer patients with limited lymph node involvement (1−2 nodes) and low RS.40 DFS improved with the lower number of involved lymph nodes, with 5-year DFS rates of 92.8%, 95.1%, 97.1%, 99.4% and 98.9% for patients with ≥4, 3, 2, 1 involved nodes and micro-metastasis, respectively.
Overall, most studies show a clear benefit of added chemotherapy in younger patients with RS >25, irrespective of clinical and pathological features, but data are controversial in older or postmenopausal subgroups with comparable RS. Additional investigations demonstrated comparable benefit of chemotherapy in lymph node-negative patients with RS 26−30 and those with RS >31.41 RS >31 was independently associated with lower a mortality rate versus RS of 26−30 despite chemotherapy, a finding consistent with the secondary TAILORx analysis.
SWOG S1007 RxPONDER. Consistent results were reported from the recent SWOG S1007 RxPONDER trial, showing that premenopausal women with HR-positive, HER2-negative, pN1 and RS ≤25 had a 45% relative risk reduction in invasive DFS events when treated with endocrine therapy plus chemotherapy.42 This study enrolled 5,083 women with N1 disease (1−3 lymph nodes) and RS ≤25, premenopausal (33.2%) or postmenopausal (66.8%) status who were randomized 1:1 to receive endocrine therapy alone or in combination with chemotherapy. Patients were subsequently followed for a median of 5.3 years. This prospective trial was sponsored by the National Cancer Institute Cancer Therapy Evaluation Program and coordinated by SWOG and was conducted in 9 countries at 632 clinical sites. Results were stratified according to RS (0−13 vs 14−25), menopausal status and type of axillary surgery (axillary dissection or sentinel-node biopsy).
In this trial, RS alone failed to predict significant benefit from chemotherapy with respect to DFS.42 Overall, the 5-year invasive DFS rate was 91.6%, while it was 92.2% among patients receiving chemotherapy plus endocrine therapy and 91.0% and among those receiving endocrine therapy alone. When adjusted for menopausal status and chemotherapy benefit, RS was found to have a relevant prognostic value (p=0.008). In the premenopausal population, the invasive DFS rate was 93.9% with chemotherapy plus endocrine therapy and 89% with endocrine therapy alone (HR: 0.60 [95% CI: 0.43−0.83]). Among postmenopausal women, 5-year invasive DFS was 91.3% with added chemotherapy and 91.9% with endocrine therapy alone. No significant differences were found when adjusting for RS and age (<50 years vs >50 years).
Higher RS was found to be non-significantly associated with greater benefit from chemotherapy, which contradicted the TAILORx study showing that chemotherapy benefit was directly proportional to an increase in RS.42 More detailed, TAILORx reported that younger women (<50 years old) achieved higher DFS rates with the addition of chemotherapy as RS increased (RS 16−20: 92.0% to 94.7%; RS 21−25: 86.3% to 92.1%).31
Despite emerging data, it remained unclear whether the chemotherapy benefit in the premenopausal group is due to direct cytotoxic effects or due to treatment-induced menopause. To avoid confusion, RxPONDER reported data according to age (clinically relevant cut-off point at 50 years), with significant chemotherapy benefit among women aged 50 or younger with RS >16.42 A subgroup analysis of this trial further showed no correlation between chemotherapy benefit and two stratification factors: type of axillary surgery and RS categories 0−13 and 14−25.
Details showing all the studies leading to validation of the 21-gene assay recurrence score are included in Table 1.
TEXT & SOFT Studies: The impact of ovarian suppression on survival
The NSABP B-30 trial previously demonstrated that induced ovarian suppression two years after chemotherapy initiation was associated with longer OS in the premenopausal group.43 Comparable results were observed in the Tamoxifen and Exemestane Trial (TEXT) and the Suppression of Ovarian Function Trial (SOFT), which showed a 5% increase in the proportion of patients with high clinical risk tumors who were recurrence-free at 8 years after receiving chemotherapy. In SOFT, the 8-year DFS rate was 78.9% with tamoxifen only, 83.2% with tamoxifen and ovarian suppression and 85.9% with exemestane and ovarian suppression (p=0.009). Among patients with HER2-negative tumors who received chemotherapy, the 8-year DFS rate with exemestane and ovarian suppression was lower compared with tamoxifen and ovarian suppression (by 7% vs 5% in SOFT vs TEXT, respectively).
Controversies
The application of Oncotype DX remains consistent with the findings of most clinically validated studies. Real-world data however, show that most breast cancer patients have an intermediate RS result, with a proportion of intermediate RS nearly twofold higher than reported in the Oncotype DX development studies.15,28,44 Due to TAILORx and RxPONDER reports, therapy decisions among younger women with intermediate RS became clearer and benefit of RS testing among these patients surpassed those in other RS categories. However, younger women with node-positive disease are given the maximum available therapy oftentimes bypassing RS testing, while in older women, treatment decision is based mostly on tumor characteristics, patient fitness level, expectations and physician’s judgment.
These studies also raised questions about the applicability of Oncotype DX in non-white populations, since only 5% of participants were African American and 6.5% Asian in RxPONDER45 and 7.1% and 4.2%, respectively, in TAILORx.39 Given the cost of RS testing, other important questions emerged, especially regarding the equity of healthcare access worldwide. Selection of clinical trial patients in countries with racially and ethnically driven socio-economic or political stratification reflects unequal access to healthcare and ultimately skews trial results.
From socioeconomic considerations to technical issues, Oncotype DX remains a rather unavailable prognostic and predictive tool available to the regular breast cancer patient and the treating oncologist.
Conclusions
The available literature shows that Oncotype DX RS should be incorporated into current recommendations for the management of early breast cancer patients, to guide treatment de-escalation of adjuvant chemotherapy, as recommended by the ASCO guidelines.6 Although various molecular biomarkers have been tested, RS has been validated through multiple retrospective and prospective trials and has been shown to outperform standard clinico-pathological characteristics as a prognostic tool.
Since its development in 2004, the Oncotype DX assay offers a new dimension in the field of personalized medicine, by assigning an independent prognostic score to patients with early, HR-positive, HER2-negative breast cancer. This prognostic tool soon evolve into a predictor of chemotherapy benefit and according to the NSABP B-20 study, results were categorized into low, intermediate and high, with increased benefit from chemotherapy with higher scores.18 Because no clear guidelines existed for patients with intermediate scores, a large prospective TAILORx study on around 10,000 patients was designed to investigate the addition of chemotherapy in women with HR-positive, HER2-negative breast cancer who had a midrange 21-gene recurrence score.31 This study showed a clear benefit of chemotherapy in premenopausal women under 50 years old. In premenopausal patients, chemotherapy was also associated with a considerable reduction in mortality rate compared with women over 50 years of age.
More recently, the RxPONDER trial enrolling around 5,000 patients with N1 breast cancer demonstrated that women with an intermediate RS had a significant benefit from the addition of chemotherapy when adjusted for menopausal status.42 As such, premenopausal women who received chemotherapy had a DFS of almost 4% more than with endocrine therapy alone, while no significant benefit was demonstrated for postmenopausal women.
Altogether, these pivoting studies indicated that chemotherapy can be safely avoided in certain breast cancer segment populations and have therefore reinforced the predictive value of Oncotype DX. This work has propelled genomic research and assay development even further. Indeed, multiple prognostic genomic assays are now available in the clinic, however not all have been tested in the context of predictive benefit and therefore cannot be used to guide treatment. Since Oncotype DX predictive value has been demonstrated, current literature supports RS testing in the daily clinical setting to reduce the burden of chemotherapy administration in selected breast cancer patients.
Conflict of Interest
Marcus Vetter received honoraria for consultancy from GSK, Roche, Novartis, Exact Sciences, Pfizer, Stemline, AbbVie and ASC Oncology. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way.
Funding
All authors have declared that no financial support was received from any organization for the submitted work.
Author Contributions
All authors contributed to and approved the final manuscript.