

Introduction
Fusarium species (spp.) are ubiquitous molds, formerly known to mainly cause plant diseases. Over recent decades, they have emerged as opportunistic pathogens of superficial, locally invasive and disseminated infections in humans worldwide,1 with a higher incidence in (sub)tropical areas.2,3 Of the 10 phylogenetic species complexes (SC), Fusarium solani SC is responsible for about half of the cases of invasive fusariosis (IF) in humans, followed by F. oxysporum SC and F. fujikuroi SC.2 Fusarial infections rarely affect immunocompetent individuals, with keratitis, especially in contact lens wearers, and onychomycosis being the most common manifestations.1–3
Immunocompromised hosts exhibit a higher risk for invasive and disseminated fusariosis as compared to other mold infections, with rising prevalence in the last decades, presumably due to increased usage of antifungal prophylaxis.2,4 In contrast to patients with hematologic malignancies and hematopoietic cell transplantation (HCT), Fusarium spp. cause less than 1% of all invasive fungal infections (IFIs) in solid organ transplant (SOT) recipients2–6 (compared to about 2.5% in patients with hematologic malignancies and HCT7) and are associated with a significantly lower mortality rate (40% vs 70−100%).2,8 In kidney transplant recipients in particular, fusariosis seems to occur only sporadically and usually more than one year after transplant.5,6,9,10 Due to the angioinvasive capability of these fungi, however, no or delayed therapy in this immunocompromised patient population can also lead to systemic dissemination with poor outcomes.2,11
In order to raise awareness of this still rare but potentially life-threatening opportunistic fungal infection, we present the case of a kidney transplant recipient who was treated for locally invasive cutaneous fusariosis in our tertiary care center in Switzerland. In addition, we review the current literature on IF in patients with SOT, with a special focus on kidney transplant recipients.
Case presentation
In November 2019, a 69-year-old black male with diabetes mellitus type 2 was referred to the department of dermatology for the evaluation of an incidental finding of an 8x4 mm painful skin ulcer on the medial edge of the left foot (Figure 1). The skin lesion atypical for a diabetic skin ulcer had been present for two months and was accompanied by an inflamed rim. The patient had not noticed the initial traumatic wound. Clinically, no onychomycosis or further skin lesions were revealed by skin examination. The patient`s medical history included a non-related cadaveric kidney transplant in 2005 due to endothelio-mesangial proliferative glomerulonephritis, arterial hypertension, dyslipidemia and splenectomy in 1996 due to splenic rupture. His infectious disease history was remarkable for recurrent staphylococcal folliculitis of the face and formerly treated latent tuberculosis and malaria. Furthermore, positive serologies for filariae, Strongyloides and hepatitis A and B were documented before the transplant. His immunosuppressive maintenance therapy comprised extended-release tacrolimus, mycophenolate mofetil and low-dose prednisone. The patient was originally from Nigeria and had been staying permanently in Switzerland since 1982, occasionally visiting his home country. No occupational or private contact with soil, plants and animals was known.

Since histologic examination of the first skin biopsy revealed a florid dermal inflammation without further specification, delayed wound healing in diabetic foot syndrome was considered. Under conservative wound care with topical antiseptic and pressure relief, the lesion resolved completely by May 2020.
Two months later, a recrudescence occurred with progression to multiple suppurating pustules within the next weeks. Granulomatous inflammation with zones of necrosis was histologically depicted in two deep skin biopsies in September 2020, without microbiological evidence for mycobacteria. First, it was again interpreted as a wound-healing disorder. As the growth of Cutibacterium acnes and Fusarium spp. was considered colonization, local disinfection with povidone-iodine was applied and no specific antifungal treatment was initiated.
In October 2020, new skin biopsies of persistent pustular ulcerated nodules on the medial edge of the left foot and the pretibial region of the left lower leg excluded the clinical differential diagnosis of verrucous carcinoma. However, periodic acid-Schiff (PAS) staining of a tissue specimen demonstrated not further specifiable isolated fungal hyphae and yeast-like elements in granulation tissue. This raised the suspicion of mycosis. Because no fungal culture was obtained at that time, empirical antifungal therapy with topical ciclopiroxolamine cream and carbamide was prescribed in November 2020 but not implemented by the patient until January 2021 due to malcompliance.
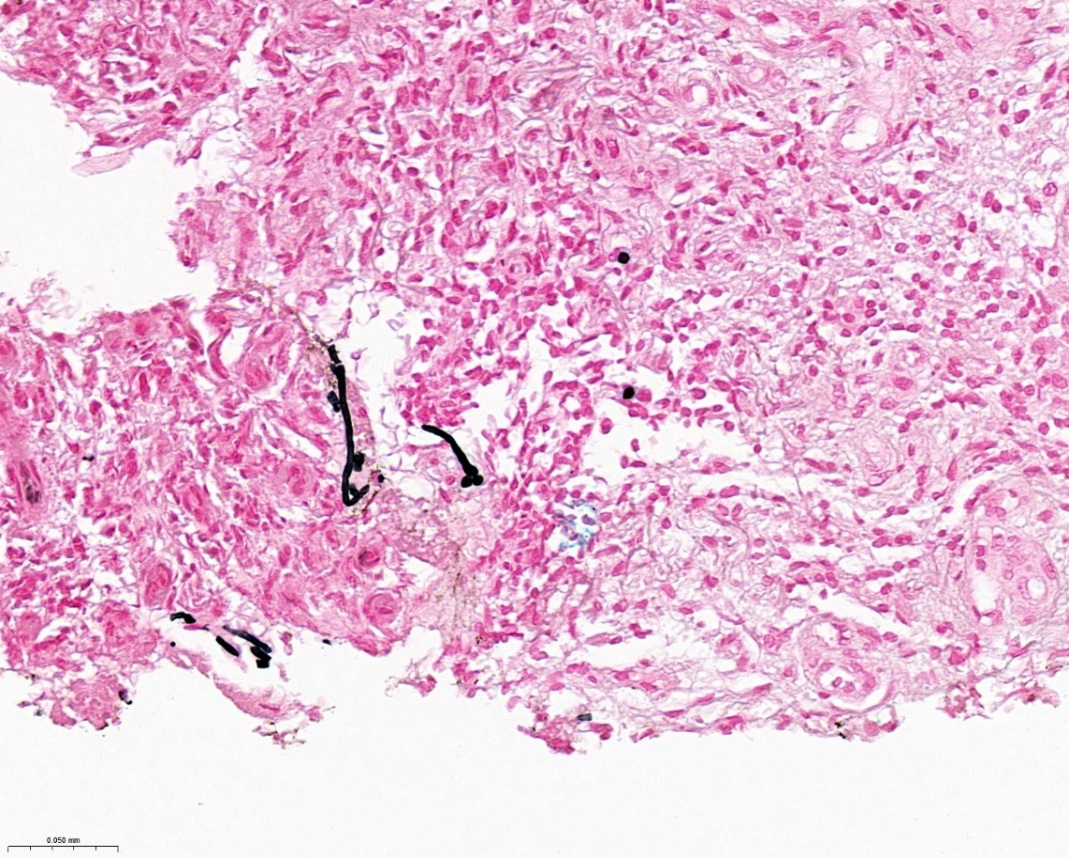
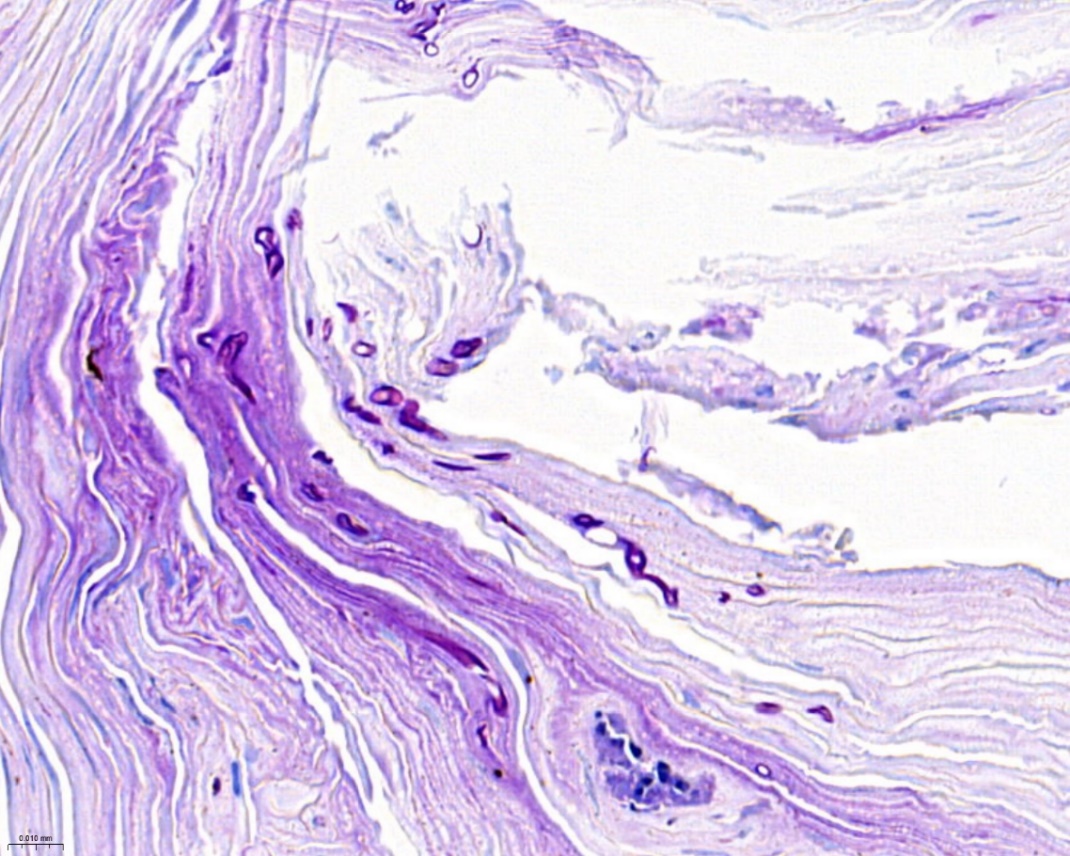
Finally, Fusarium solani SC was identified in the fungal culture from a deep wound swap performed in March 2021 due to a lack of healing. The spread of additional nodules along the lymphatics of the left leg up to the knee (Figures 2A and 2B) without lymphadenopathy led to the involvement of the department of infectious diseases and the performance of a repeat skin biopsy in May 2021. PAS staining showed moderately abundant fungal elements with some sloped cuts of hyphae and many questionable fungal spores without budding (compatible with microconidia), as well as partly empty imposing thick-walled chlamydoconidium in the horny layer (Figures 3 and 4). Repeated cultivation of the skin tissue confirmed Fusarium solani SC infection.
_further_deterioration_of_the_lesions_on_the_left_foot_and_b)_the_occurrence_of_addition.png)
_without_budding._grocott_staining__39.5.jpeg)

Antifungal resistance testing revealed low minimum inhibitory concentrations (MICs) for amphotericin B (AmB) (MIC: 0.125−0.19 µg/ml) and voriconazole (4.0 µg/ml), compared to the other antifungal agents such as posaconazole, fluconazole and echinocandins (MIC >32 µg/ml), respectively. Routine blood cultures remained without growth and the patient did not present fever or other signs of hematogenous dissemination. Systemic inflammatory parameters were normal. Considering all clinical, microbiological and histological findings, a focally invasive fusarial skin infection with lymphatic spreading in an immunocompromised SOT recipient was diagnosed.
Given the patient’s good general condition, systemic antifungal therapy with oral voriconazole was initiated in July 2021 (loading dose of 6 mg/kg/body weight every 12 hours, followed by 4 mg/kg/body weight every 12 hours as maintenance dosage), while closely monitoring tacrolimus blood levels. After four months of treatment, all skin ulcers subsequently resolved by November 2021.
In December 2021, the patient had to be admitted to an intensive care unit due to Covid-19 pneumonia. Voriconazole treatment was continued because of a few persistent palpable nodules. A computed tomography scan raised no suspicion of fungal superinfection of the lung and there was no clinical evidence of disseminated fusariosis. Unfortunately, the patient deteriorated respiratorily and died due to acute respiratory distress syndrome. According to the will of the patient’s relatives, no autopsy was performed.
Discussion and literature review
With primary cutaneous infection, direct inoculation via impaired skin barrier was the presumable route of transmission in our patient and is also described in the literature as the main entry point for Fusarium in immunocompromised patients, along with the respiratory tract.2,3 As the patient wore unsuitable non-orthopedic footwear despite diabetic neuropathy, minor skin injuries, which were not noticed due to decreased sensibility, were the most likely port of entry.
Limited superficial and deep skin infections appear to be the most common manifestation of fusariosis among SOT patients (45–70%), except for pneumonia in lung transplant recipients. Other organ manifestations described in transplanted individuals are sinusitis, peritonitis, osteomyelitis and infections of the central nervous system.9,10 Disseminated disease occurs in up to 25% of the cases.9 According to the literature, most kidney transplant recipients affected by fusariosis also presented with localized cutaneous disease, predominantly on the lower extremities.10,12
Fusarium can cause a variety of infection patterns on the skin, complicating the clinical diagnosis. Typically, primary skin involvement manifests with erythematous plaques, papules or nodules that can lead to pustular reactions and cause purulent or hemorrhagic ulcers and necrosis with vascular invasion, imitating vasculitis. Dermal or subcutaneous involvement may also be associated with the development of nodules with granulomas or panniculitis-like inflammation. Central necrotic ulceration occurs in up to 75% of cases with disseminated disease.3,13 Our patient initially suffered from ulcerations, for which an ischemic-vascular or neoplastic origin was first assumed. The interpretation as a wound-healing disorder with bacterial and mycotic colonization in diabetic foot delayed diagnostics and the targeted treatment of Fusarium. Furthermore, the lack of response to topical therapy was partly misinterpreted due to the patient’s malcompliance. The subsequent appearance of purulent nodules raised the suspicion of an infectious genesis, which could only be confirmed after repeated cultivation.According to the revised European Organization for Research and Treatment of Cancer/Mycoses Study Group (EORTC/MSG) criteria for proven IFI, diagnostic criteria for IF are fulfilled by the cultural detection of Fusarium spp. and the histological depiction of fungal elements from sterile material of a skin biopsy.14,15
Histopathologically, 3 to 8 µm wide, septate and hyaline filamentous hyphae with haphazardly branching, often perpendicularly to their hyphae of origin, are usually seen, in some way resembling those of other hyalohyphomycetes like Aspergillus and often making further differentiation difficult.2,3,11 However, adventitious yeast-like sporulation without budding (microconidia), as in the presented case, can give a clue for fusariosis in high-risk patients.2,15 As morphological subtyping of fungal elements is not possible, microbiological culture results are necessary to confirm the diagnosis and identify the species of the pathogen.2,16
Negative blood cultures excluded hematogenous dissemination in our patient. In fact, fungemia is described in the literature in up to 40% of invasive cases but seems to be uncommon in SOT patients.2,10 Serological tests are hence of limited clinical relevance; while galactomannan is mostly negative in fusariosis, 1,3-beta-D-glucan is often detectable but nonspecific.4
International guidelines recommend liposomal AmB or voriconazole as first-line antifungal therapy for fusariosis due to intrinsic resistance to most currently used antifungals.16–18 Frequently, combination therapy is used in primary treatment for severe invasive infections despite the lack of evidence from clinical trials. We opted for oral monotherapy with voriconazole because of acceptable cure rates for localized infections in the literature.9 Furthermore, given the potential nephrotoxicity, its cost and availability only as an IV formulation, requiring hospitalization, we decided against the treatment with liposomal AmB in this kidney transplant patient.19 The well-known drug-drug interaction by inhibition of CYP3A4 and CYP3A5 enzymes by voriconazole required close monitoring of the tacrolimus blood levels.20 According to Gavaldà et al. (2014),17 dose reduction by around 30% for tacrolimus should be considered in the case of concomitant use of voriconazole. In our patient, tacrolimus blood levels were within the target range after halving its dose. The lack of standardized MIC break-points for Fusarium complicates the interpretation of the susceptibility profile of isolates.18 However, Nucci et al. (2021) could demonstrate that there is no correlation between MIC and mortality in patients with IF.21 Since our patient showed clinical improvement of the skin lesions after about four months of treatment, we assumed that therapy with voriconazole was effective and continued it until his Covid-19-related death without evidence of systemic dissemination or relapse. No therapy-related adverse events occurred during treatment.
Conclusion
Fusariosis represents a very rare IFI in SOT patients, especially in kidney transplant recipients, with cutaneous infections being the most common manifestation. However, since even localized disease may progress to systemic dissemination with increased mortality, this patient population should be regularly screened for the presence of skin lesions. An accurate histopathological examination and microbiological workup of these lesions, including fungal cultures, is necessary for diagnosis. Systemic antifungal therapy with voriconazole remains the treatment of choice for localized IF. In SOT patients specifically, immunosuppressant drug levels should be monitored closely due to potential drug-drug interactions.
Ethics approval and consent to participate
Not applicable.
Consent for publication
General written informed consent was obtained from the patient for the publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Availability of data and materials
All patient data that support this case report are included in anonymized form in the published article.
Conflict of interest
The authors have declared that the manuscript was written in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
No funding was obtained for this article.
Authors’ contributions
HS: Involved in patient care, drafted and revised the manuscript
RR: Performed histological assessment and contributed to the pathological section
IS: Involved in patient care, revised the manuscript
KB: Involved in patient care, contributed to the infectiological section, revised the manuscript
WA: Involved in patient care, contributed to the infectiological section, revised the manuscript
JS: Involved in patient care, drafted and revised the manuscript
All authors contributed to and approved the final manuscript.