

Overview of the San Antonio Breast Cancer Conference
The San Antonio Breast Cancer Symposium (SABCS) is an annual scientific conference that focuses on breast cancer. The conference has been taking place since 1977 and is considered one of the most important events in the field of breast cancer research. Each year, about 4,000 scientists from around the world participate in the SABCS to discuss and learn about the latest research findings. The conference provides a platform for scientists, clinicians, and patients to share their ideas and insights with others. In recent years, the focus of the conference has changed to better meet the needs of patients with breast cancer and to focus on early detection of cancer. The treatment options for breast cancer are also better understood, which helps to improve the quality of life for patients. The SABCS is also known for its friendly and open atmosphere. At the conference, people from all over the world and from different disciplines come together to learn and discuss. This diversity of perspectives is one of the reasons why the SABCS is considered one of the most important events in the field of breast cancer research.
Some of the top presentations at the conference
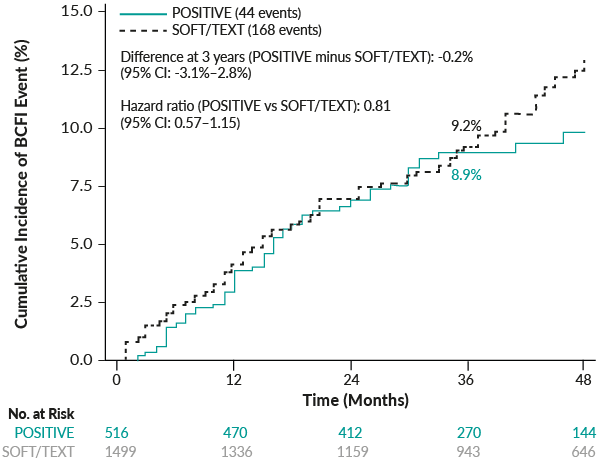
One notable study, also of interest from a Swiss perspective, was the POSITIVE/IBCSG 48-18 trial, which included patients with hormone receptor-positive (HR+) early breast cancer and a desire for children.1 In this single-arm study, endocrine therapy was interrupted for 2 years to attempt pregnancy. The median age was 37 years. The relapse risk after 41 months of median follow-up was not higher than in other studies at 8.9% (Figure 1). The birth rate was relatively high at 64%. The study prospectively demonstrated for the first time that pregnancy is also possible with an early HR+ breast cancer diagnosis.
_in_the_positive_study_in_the_context_of_the_soft_text_t.png)
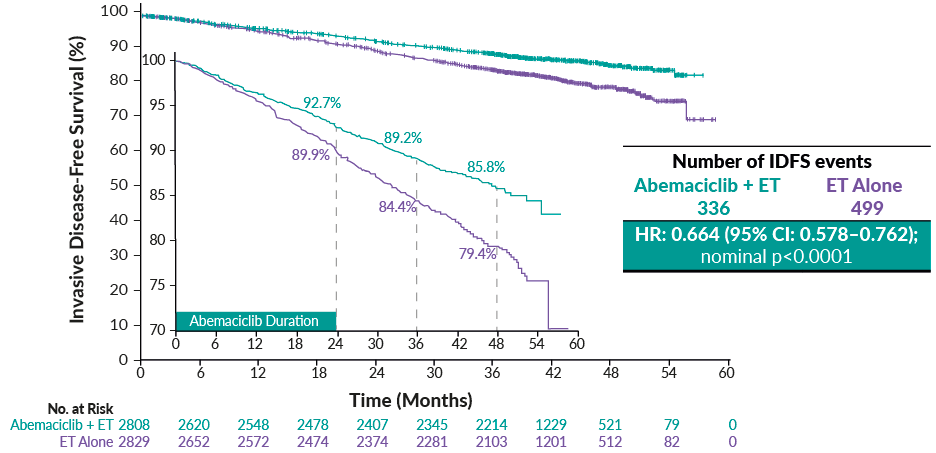
In early HR+ breast cancer with a high risk of relapse, follow-up data from the monarchE study after 42 months was shown.2 Abemaciclib, a cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitor, in combination with an aromatase inhibitor (AI) is a standard therapy in the metastatic setting and doubles the progression-free survival (PFS) compared with AI alone. In this study, adjuvant treatment with abemaciclib for 2 years added to standard AI therapy showed a continuous benefit in terms of relapse risk (Figure 2). During the follow-ups, 125 patients had metastases under the study therapy compared with 249 patients with AI alone. In Switzerland, the drug is not yet approved for early disease, but with a continuous benefit, an off-label use is likely after critical discussion with the patient.
_benefit_persists_beyond_completion_of_abemaciclib_in.png)
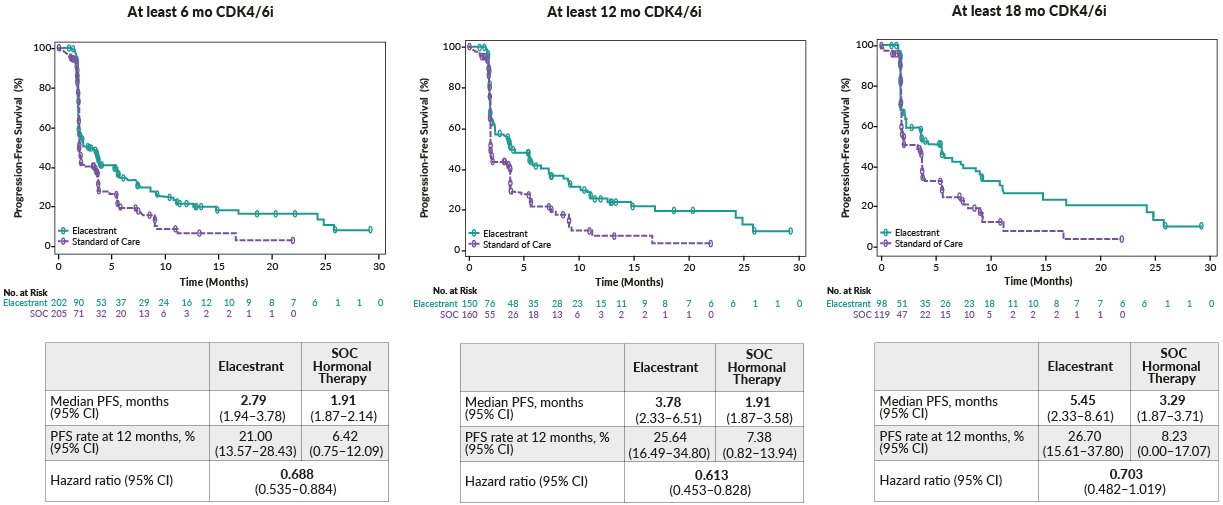
In the treatment of advanced HR+ breast cancer, there is room for innovation after CDK4/6 inhibitor failure and many studies on this topic were presented. The data from EMERALD showed a clear advantage of elacestrant over a standard second-line therapy.3 Elacestrant is an oral selective estrogen receptor downregulator (SERD) that is presumed to work better than AI in breast cancer harboring receptor mutations (ESR1 mutations). The longer patients were under treatment with CDK4/6 inhibitors, the greater benefit they derived from subsequent treatment with elacestrant (Figure 3). In the future, oral SERDS will significantly change the treatment landscape of breast cancer, probably also in early stages, and will likely serve as a backbone for other tyrosine kinase inhibitors. The data from the CAPItello-291 study was also presented at the congress.4 Here, patients who had received prior CDK4/6 inhibitor therapy were treated with fulvestrant, an intramuscular SERD, together with either the pan-AKT inhibitor capivasertib or placebo. The study demonstrated a significant PFS benefit with the combination therapy (Figure 4).
_with_elacestrant_versus_endocrine_therapy_by_duration_of_p.png)
_in_the_capitello-291_trial.png)
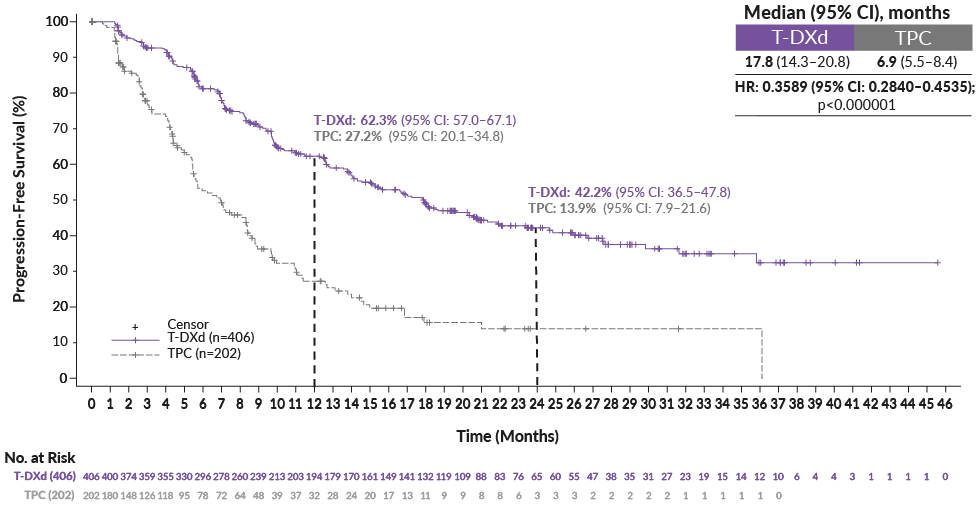
Both in triple-negative and in advanced HR+/human epidermal growth factor receptor 2-positive (HER2+) breast cancer, antibody-drug conjugates (ADCs) have shown a significant improvement in prognosis and are currently being intensively researched. At SABCS 2022, several updates as well as new data were presented. On trastuzumab deruxtecan (T-DXd), a molecule consisting of the HER2-targeting antibody trastuzumab, a linker substance, and the chemotherapy drug deruxtecan, a topoisomerase I inhibitor. The phase III study DESTINY-Breast02 compared T-DXd with treatment of physician’s choice (TPC) in patients with HER2+ advanced breast cancer previously treated with the longer approved ADC trastuzumab emtansine (T-DM1).5 T-DXd significantly improved response rates, PFS (Figure 5), and overall survival (OS). The ADC was also tested in metastatic breast cancer with low HER2 expression (HER2-low) (DESTINY-Breast04) and demonstrated a clear advantage over standard chemotherapy.6 A subgroup analysis of the study, which was presented at SABCS 2022, showed that patients whose tumors were rapidly progressive particularly benefited from treatment with T-DXd, with an overall response rate of 50% compared with 0% among those who received standard chemotherapy (Figure 6).7
_in_the_destinybreast02_trial.png)
_in_the_destinybreast04_trial.png)
What the conference means for the future
In recent years, treatment options for breast cancer have improved significantly. There is now more hope for those affected that their cancer can be cured. At the SABCS 2022 a great deal of new data on new and more effective therapeutic options were presented. Notably, treatment is becoming more complex. For example, breast cancer is no longer necessarily treated according to classical intrinsic subtypes, but instead based on theragnostic markers such as HER2 expression or BRCA mutations. ADCs are playing a pioneering role here. In the future, more personalized approaches will become available. In particular, many studies are now also focusing on patients’ quality of life, such as the feasibility of pregnancy when diagnosed with breast cancer. Overall, the prognosis for patients with breast cancer will continue to improve.
Conflict of interest
Marcus Vetter received honoraria for consultancy from GSK, Roche, Novartis, Exact Sciences, Pfizer, Stemline, AbbVie and ASC Oncology. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way. Julia Landin has declared that the manuscript was written in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors have declared that no financial support was received from any organization for the submitted work.
Author contributions
All authors contributed to and approved the final manuscript.