
Introduction
Fusariosis is the second most common invasive fungal infection (IFI) after aspergillosis, targeting mostly highly immunocompromised patients, such as allogeneic hematopoietic stem cell transplantation (HSCT) recipients, and is associated with a mortality rate of 50−80%.1–3 Hence, rapid recognition of its clinical manifestations and immediate introduction of effective treatment are essential.2 Treatment is particularly difficult because of an extended in vitro resistance against multiple antifungal agents.4 Although regimens based on liposomal amphotericin-B or voriconazole are suggested as first-line therapies, the optimal treatment strategy remains controversial.5 This case report illustrates the diagnostic and management challenges in the treatment of disseminated fusariosis.
Case report
An 18-year-old patient with a history of allogeneic HSCT from a related haploidentical donor for acute myeloid leukemia (AML) received a second allogeneic HSCT from an unrelated HLA-mismatched (8/10) donor following sequential reduced-intensity conditioning due to relapse of AML, 5 months after the first HSCT. The prophylaxis regimen consisted of acyclovir 500 mg/8h intravenously (IV), atovaquone 1,500 mg/24h orally (PO) and letermovir 480 mg/24h/PO. The patient was previously receiving isavuconazole 200 mg/24h/PO for more than 9 months (serum plasmatic level on post-transplant day [PTD]-1 was 2.9 mg/l), due to a pulmonary Rhizomucor spp. infection diagnosed 12 months before the second HSCT, for which the patient underwent surgical resection. Graft versus host disease (GvHD) prophylaxis consisted of cyclophosphamide, tacrolimus and mycophenolate mofetil (MMF). The patient had already presented long-term neutropenia for 2 months prior to the second HSCT as a result of salvage chemotherapy with venetoclax and 5-azacitidine.
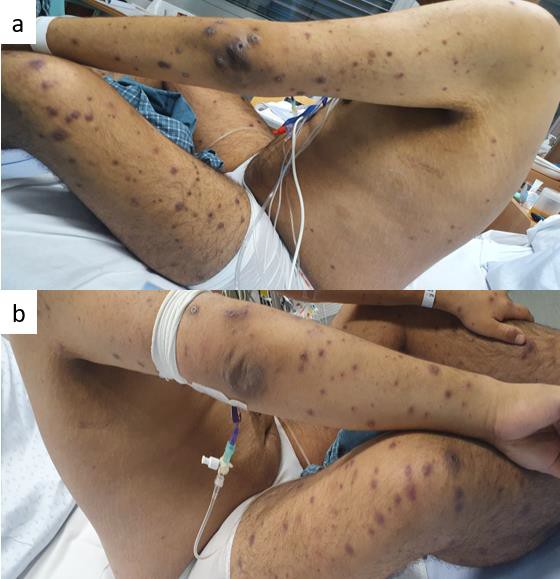
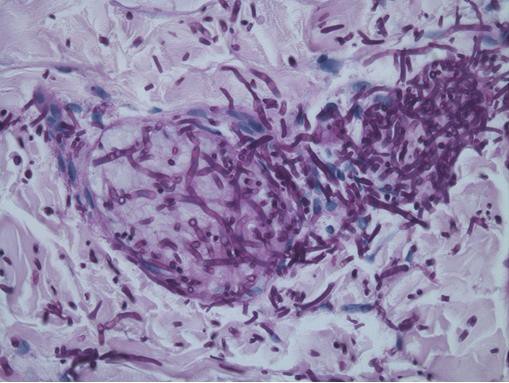
On PTD-2, the patient presented neutropenic fever associated with multiple cutaneous papular non-tender, non-pruritic lesions on the feet, soles, legs, palms, fingers and face, with significant inflammation and rapid dissemination by PTD-9 (Figures 1A and 1B). Empirical antibiotic treatment with liposomal amphotericin B (L-AmB) 5 mg/kg/24h/IV was started on PTD-2, considering the high clinical suspicion for fusariosis. Serum beta-D-glucan (Fungitell; <7 pg/ml) and galactomannan enzyme immunoassay (GM-EIA, Platelia Aspergillus Bio-Rad; <0.5) on PTD-1 were negative. Blood cultures taken on PTD-2 became positive on PTD-4, with the identification of Fusarium fujikoroi on PTD-5 and remained positive until PTD-14. A cutaneous biopsy of a skin lesion obtained on PTD-2 showed filamentous fungal-like structures on periodic acid-Schiff (PAS) and Grocott stains associated with vascular thrombosis (Figure 2). After the microorganism identification, voriconazole 4 mg/kg/12h/IV was added to L-AmB on PTD-5, after two doses of loading dose with 6 mg/kg/12h/IV. Antibiogram results became available on PTD-14 and showed the following minimal inhibitory concentrations (MICs): posaconazole: 0.5 mg/l, voriconazole: 2 mg/l, isavuconazole: 4 mg/l, itraconazole: 16 mg/l, fluconazole: 256 mg/l, Amp-B: 2 mg/l and anidulafungin-caspofungin: 8 mg/l. The additional diagnostic evaluation included: (i) chest (PTD-2) and sinus CT (PTD-6) without signs of a fungal infection, (ii) transthoracic echocardiogram on PTD-8 and PTD-11 without any signs of cardiac valve vegetations and (iii) repeat beta-D-glucan and serum GM-EIA. On PTD-12, the serum beta-D-glucan resulted positive (9.1 pg/ml) and continued to increase until PTD-25 (108 pg/ml), while serum GM-EIA remained negative. On PTD-16, L-AmB was discontinued due to acute renal injury and voriconazole was changed to posaconazole at 300 mg/12h/IV on PTD-19, due to the relatively high voriconazole MIC and the steady-state voriconazole trough level of 3.20 mg/l on PTD-18. The patient engrafted on PTD-20. Posaconazole trough level on PTD-29 was undetectable, prompting replacement by voriconazole on PTD-31 at 7 mg/kg/12h/PO, with a trough voriconazole level at 2.67 and 4.01 mg/l on PTD-43 and PTD-53, respectively. To complete the diagnostic work-up, a whole-body positron emission tomography (PET)-CT was performed on PTD-33, showing multiple cutaneous, subcutaneous, muscular, lung, thyroid and bone hypermetabolic foci (Figure 3A). The patient was eventually discharged home on PTD-36 on voriconazole monotherapy (7 mg/kg/12h/PO).


-computed_tomography_(ct).jpeg)
On PTD-74, the patient was re-hospitalized due to a new cutaneous inflamed lesion on the right foot, raising suspicion for the progression of the fusariosis and leading to the addition of L-Amp-B 5 mg/kg/24h/IV to voriconazole on PTD-79. The known lesions on the lower and upper extremities were stable and the serum beta-D-glucan was 16.3 pg/ml, with a voriconazole trough level of 4.13 mg/l upon readmission. A PET-CT scan on PTD-79 showed more sub-cutaneous and muscular nodules in the upper and lower extremities and contrast bilateral uptake of the knees and a minimal right pleural effusion (Figure 3B). A biopsy of the new right foot lesion (PTD-80) revealed a granulomatous suppurative reaction (dense mixed infiltrate of numerous neutrophils and foci of granulomatous reaction associated with multinucleated giant cells and foci of necrosis) with rare filamentous elements on the hematoxylin-eosin stain; PAS and Grocott stains were negative. A diagnostic arthrocentesis of both knees was performed on PTD-81 (left knee: leucocytes 9,126 m/l, 74% neutrophils; right knee: leucocytes 11,750 m/l, 81% neutrophils), with negative fungal culture and a panfungal polymerase chain reaction (PCR) 18S-rDNA confirming the presence of a Fusarium spp. on the left knee but not on the right one. A broncho-alveolar-lavage (BAL) was performed on PTD-85 and the BAL cultures remained negative, while a panfungal PCR 18S-rDNA was positive for Fusarium spp. A diagnosis of disseminated fusariosis with proven skin, joint, probable lung and possible bone involvement was established. Combination antifungal therapy with L-AmB at 5 mg/kg/24h/IV and voriconazole at 8 mg/kg/12h/PO was maintained. The trough voriconazole plasmatic level on PTD-83 was 5.66 mg/l and both antifungal agents were well tolerated. GvHD prophylaxis with tacrolimus was discontinued on PTD-80 and the patient was eventually discharged home on PTD-107 under voriconazole (8 mg/kg/12h/PO) and L-AmB (7.5 mg/kg/3 times a week/IV).
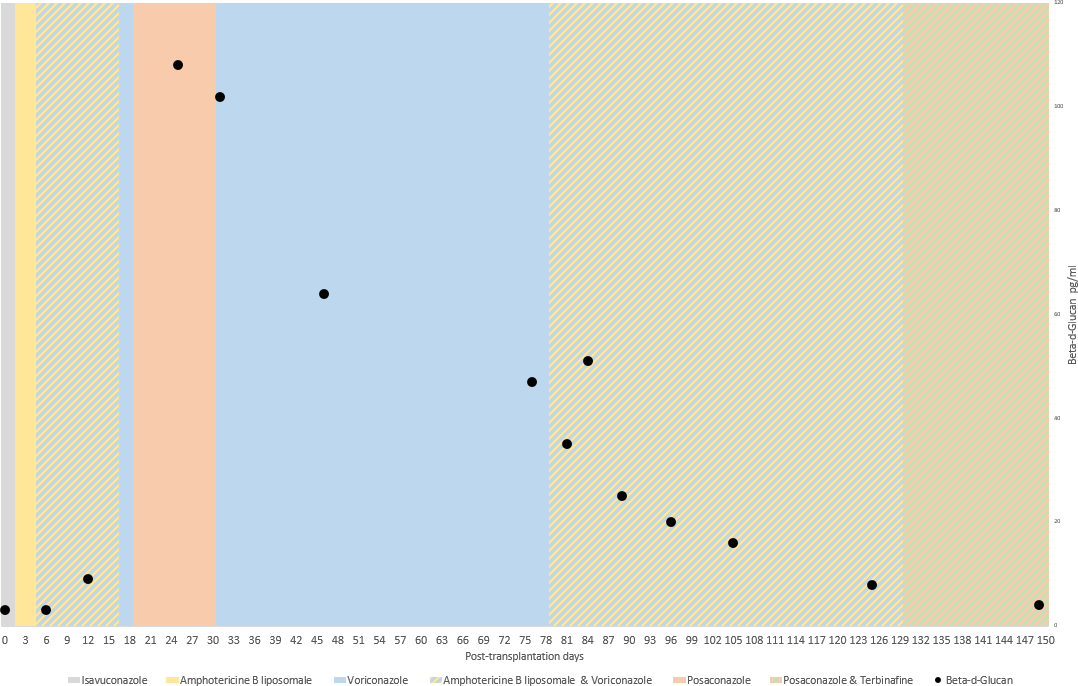
Several weeks after discharge, the patient developed acute, intense bilateral hip pain, more pronounced on the left than the right side, which could not be controlled with morphine. Due to the intense pain, the patient was not able to get out of bed and had to be transferred to the hospital on a stretcher. A new whole-body PET-CT performed on PTD-121 showed new contrast uptake on the left hip, with a discordant evolution of the extremity lesions (reduction of some cutaneous, sub-cutaneous and muscular lesions and progression of some others) (Figure 3C). A diagnosis of left hip periostitis was made, considered to be associated with the administration of high-dose voriconazole. Voriconazole and L-AmB were discontinued on PTD-130 and replaced by posaconazole at 200 mg/8h/PO, a dose selected based on the undetectable posaconazole plasma level on a 300 mg/12h/IV dose during the previous hospitalization, with an increase to 300 mg/8h/PO on PTD-142 due to a plasma level of 1.8 mg/l. Terbinafine 250 mg/12h/PO was added to posaconazole on PTD-130 based on the extent of this infection, with literature data showing good efficacy against molds, including Fusarium spp., and its good bone penetration (Figure 4). On PTD-136, the patient was discharged on the above-mentioned orally administered antifungal therapy, which was well tolerated. Within days after voriconazole discontinuation, the patient’s pain gradually improved and several weeks later the patient was pain-free and fully mobile. Posaconazole trough levels on PTD-145 and PTD-203 were 3.0 mg/l and 3.9 mg/l, respectively.

Numerous PET-CT scans (on PTD-180, PTD-237, PTD-321 [Figure 3D] and PTD-445) were performed in order to assess the evolution of the multiple lesions. As seen in Figure 3E, the disseminated lesions resolved almost completely on the last PET-CT on PTD-445, with the persistence of the known osteolytic lesion, but with a reduction of the metabolic hypercaptation (talus and tibia left). On PTD-501, considering the complete clinical and partial radiological response, complete immune reconstitution and lack of immunosuppression, the antifungal treatment was discontinued.
Discussion
This case illustrates three major points in the management of fusariosis in allogeneic HSCT recipients: (i) high clinical suspicion based on typical clinical and microbiologic findings, (ii) challenging treatment options, with variable MICs to different antifungal agents, (iii) multiple adverse events associated with long-term administration of voriconazole.
Our patient presented the typical diffuse purple cutaneous papular lesions with central necrosis in all four extremities, seen in about 85% of fusariosis cases; these findings should promptly raise suspicion for this entity in the relevant clinical context.6,7 Clinical suspicion requires microbiological confirmation, either via tissue biopsy or culture and other surrogate diagnostic biomarkers. Skin biopsies with the histopathological examination are accessible and simple to perform, even in patients with thrombocytopenia, and provide definitive evidence of invasive disease. As the morphology of hyphae is similar to Aspergillus spp. and Scedosporium spp. (septate, narrow and acute angle branching), the diagnosis has to be confirmed by culture or PCR.1 Disseminated fusariosis is one of the few mold infections associated with fungemia, as Fusarium spp. can sporulate in vivo and blood cultures may become positive in >50% of immunosuppressed patients after a median of three days of incubation.1,8 Indirect biomarkers, such as beta-D-glucan and GM-EIA may become positive in cases of fusariosis. The specificity and sensitivity after two consecutive tests of beta-D-glucan are 69% and 85%, respectively, with a high negative predictive value of 99% reported.9 The GM-EIA has been reported to have a sensitivity of 83% and specificity of 67%.8 Notably, the GM-EIA was negative in our patient and it remains unknown whether this is related to the specific Fusarium spp. isolated or other reasons. In this case, the prompt diagnosis and targeted treatment initiation were based on the identification of those classical findings, which is pertinent considering the high mortality associated with this infection.3
The combination of immunosuppression reduction and prompt initiation of an effective antifungal regimen is the cornerstone of the therapy of fusariosis.5 Considering that this pathogen is often resistant to the most commonly used antifungal agents, treatment selection can be challenging.10 Fusarium solani spp. complex (FSSC) is the most common pathogenic species and presents the highest MICs against different agents (e.g. L-AmB: 0.5−16 µg/ml, voriconazole: 0.12 to >16 µg/ml, posaconazole: 2 to >16 µg/ml).4 Infections by Fusarium fujikuroi spp. complex (FFSC) represents one-third of all disseminated fusariosis and show a similar resistance profile to FSSC.11 Moreover, data on the correlation between MICs to Fusarium spp., or other molds, and the response to treatment are very scarce.12 Empirical antifungal treatment recommendations include either voriconazole or L-AmB, as suggested by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID).5 To date, no clinical breakpoints exist for Fusarium species, but the Clinical and Laboratory Standards Institute (CLSI) has proposed epidemiological cut-off values (ECVs; e.g. F. verticillioides [FFSC] AmB: 4 µg/ml, posaconazole: 2 µg/ml, voriconazole: 4 µg/ml).13
Consistent with multiple recent reports, our patient developed an isavuconazole breakthrough IFI, further adding to the complexity of treatment of a disseminated IFI in highly immunocompromised hosts.14,15 Since the most studied antifungal combination of voriconazole is with L-AmB, the latter was initiated despite the lack of robust relevant clinical data.6,16 Data on the use of posaconazole and terbinafine are scarce and based mostly on case reports.17 ESCMID guidelines recommend posaconazole only as salvage therapy.5 The choice of the salvage concomitant administration of posaconazole with terbinafine was based on different in vitro studies that showed a potential synergy between voriconazole and terbinafine, relatively low MIC for terbinafine associated with good bone penetration and the possible oral administration of this agent.17 Our experience supports the limited body of evidence suggesting that the combination of those two agents can be effective and well tolerated, particularly in cases where other treatment options, at least based on the currently available antifungal therapies, may be extremely limited.
Triazoles and polyenes are often associated with multiple side effects leading to treatment changes and interruptions.18 Although less frequently described, long-term administration of voriconazole has been particularly associated with adverse events, such as skin lesions and cancers, neurological disorders, arrhythmias and periostitis.19 Our patient developed hip periostitis, a rare side effect unique to voriconazole which is present in <10% of patients on long-term voriconazole therapy, probably due to its high fluoride content (15 times higher than the normal daily intake). High doses of voriconazole are associated with a higher risk but patients on prophylaxis can also develop this side effect.20 The ulna and ribs are the most common locations. Plasma fluoride level >8 μmol/L (not investigated in our case), high level of alkaline phosphatase and bilirubin associated with bone pain and radiological signs can further support this diagnosis. In the case of periostitis, the immediate transition to another active agent is necessary and it is normally associated with a complete and rapid resolution of symptoms.
Conclusion
In conclusion, typical skin lesions and positive blood cultures for molds should promptly raise suspicion for fusariosis. Amphotericin-B and voriconazole are the first-line agents for the treatment of fusariosis. Second-line agents such as posaconazole and terbinafine can occasionally be used.
Ethics approval and consent to participate
Not applicable.
Consent for publication
General written informed consent was obtained from the patient for the publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Availability of data and materials
All patient data that support this case report are included in anonymized form in the published article.
Conflict of interest
Yves Chalandon has received honoraria for participation in symposia and advisory boards and funding for participation at meetings from Novartis. Dionysios Neofytos has received research support from MSD and Pfizer and consulting fees from MSD, Pfizer, Basilea, and Gilead. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way. Other authors have declared that the manuscript was written in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.