

Introduction
For decades, intensive induction therapy consisting of a 7-day continuous infusion of cytarabine and a 3-day course of daunorubicin or idarubicin (“7+3”) has been the backbone of acute myeloid leukemia (AML) treatment.1,2 This regimen achieves durable response mainly in young and fit patients with favorable-risk AML. However, most patients with AML are older than 65 years with multiple comorbidities and the clinical outcomes in this population are poor, mostly due to unfavorable-risk genetics and low tolerance to intensive chemotherapy.3,4 Recently, CPX-351, a liposomal formulation with a fixed combination of cytarabine and daunorubicin, has been approved by the Food and Drug Administration (FDA) and European Medicines Agency (EMA) for the treatment of newly diagnosed AML patients with a poor prognosis.5,6 In the randomized, phase III CLTR0310-301 trial, the liposome-encapsulated combination versus the standard combination of cytarabine and daunorubicin (“7+3” regimen) was associated with significantly prolonged median overall survival (OS) (9.6 months vs 5.9 months; HR: 0.69 [95% CI: 0.52−0.90]; p=0.005) in patients aged 60–75 years with newly diagnosed high-risk or secondary AML.7 The improved OS with CPX-351 versus “7+3” was maintained after a follow-up of 5 years in this patient population.8 The antitumor activity of this therapy was also demonstrated in a real-world analysis of high-risk AML patients treated with frontline CPX-351, with a median OS of 21 months and a 1-year OS rate of 64% after a median follow-up of 9.3 months.9 A very recent retrospective comparative analysis further demonstrated that CPX-351 versus hypomethylating agent (HMA) plus venetoclax, a B-cell lymphoma-2 (BCL-2) protein inhibitor, was associated with prolonged OS in the overall population (range, 34−93 years).10 However, there was no difference in clinical outcomes between the two treatment regimens in the group of patients aged 60−75 years, despite a more than the doubled rate of transplant in the CPX-351 arm.
The hypomethylating agent (HMA) azacitidine is another treatment option for elderly patients with newly diagnosed AML with >30% bone marrow blasts who are not suitable for or cannot tolerate intensive chemotherapy.11 The efficacy and safety of this agent was established in the randomized, open-label, phase III AZA-AML-001 trial, which showed improved median OS with azacitidine versus conventional care regimens (CCRs) in patients age ≥65 years (10.4 months vs 6.5 months; HR: 0.85 [95% CI: 0.69−1.03]; p=0.1009), with 1-year OS rates of 46.5% and 34.2%, respectively.12 This OS benefit was maintained across all prespecified subgroups, including poor-risk cytogenetics. Azacitidine was generally well tolerated in this patient population; nausea, neutropenia and thrombocytopenia were the most common treatment-emergent adverse events.
In addition to age and the presence of comorbidities, the genetic background of the patient should be considered when assessing disease prognosis and planning the treatment.13 Recurrent mutations, identified mainly by next-generation sequencing (NGS), play an important role in AML prognosis and the response to the therapy (Figure 1). Their identification led to the development of genetic classification systems, which underline the variability of this heterogeneous disease and refine risk stratification. In 2010, the European LeukemiaNet (ELN) defined the first genetic-based stratification system for AML,14 which was recently revised, following the better understanding of the impact of recurrent mutations on outcomes after intensive chemotherapy.13 The most important changes in the updated guidelines include the refined definition of the three prognostic (genetic-risk) subgroups (favorable, intermediate and adverse) based on leukemia cell cytogenetics and mutations. Another novelty is the quantification of the FLT3-internal tandem duplication (ITD) allelic burden defined by the ratio of mutated and normal alleles. In addition, a specific AML subtype should be defined by genetic aberrations at the time of diagnosis, as well as the presence of particular gene mutations during or after treatment. For example, the detection of a residual mutation in NPM1 transcripts during complete remission in patients with NPM1-associated AML indicates an increased probability of relapse. This topic is briefly discussed in the section Monitoring disease progression with MRD.

Expanding AML treatment armamentarium
Targeted therapies
FLT3 inhibition
In the past years, targeted therapies have reshaped the treatment landscape of AML.15–17 Among these, the FLT3 and isocitrate dehydrogenase (IDH) inhibitors used as monotherapy have emerged as a treatment option particularly important for patients ineligible for intensive chemotherapy.
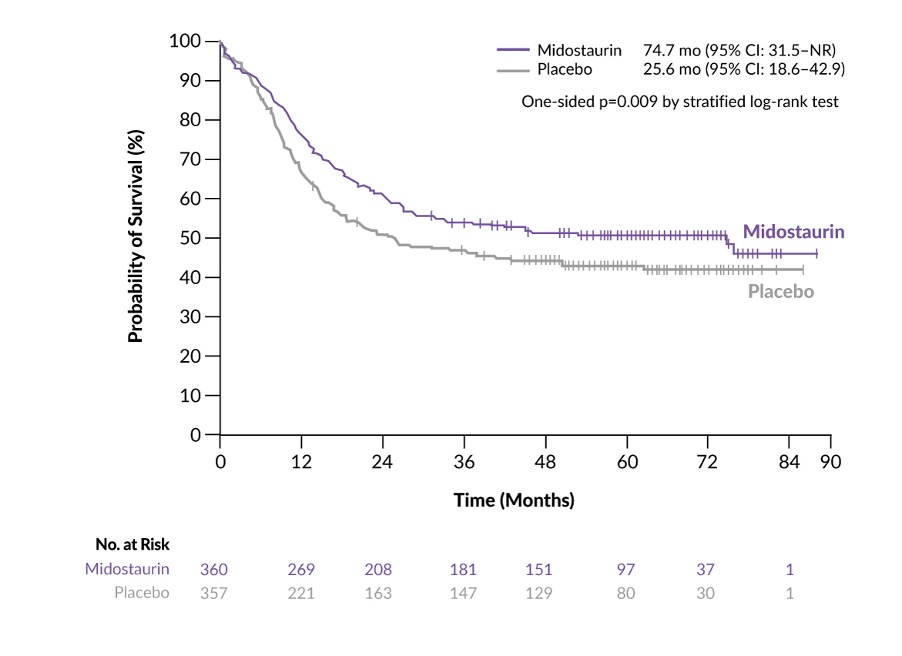
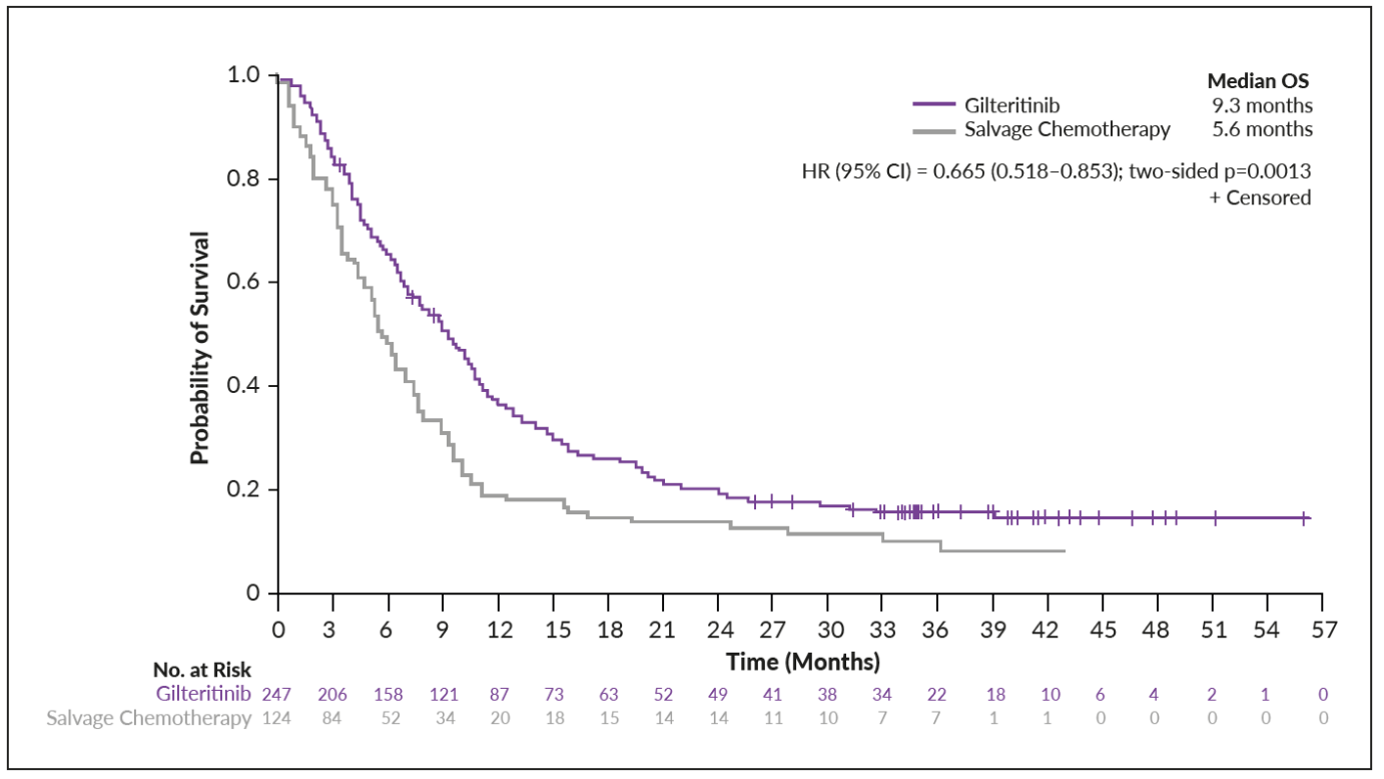
Mutations in FLT3, which are present in about 30% of patients with AML, result in constitutive activation of the receptor and its downstream pathways.18 FLT3 mutations are specific to the AML phenotype and may be detected in almost all AML subtypes, while they are rarely present in other myeloid neoplasms.19 The first-in-class FLT3 inhibitor midostaurin was approved in 2017 by Swissmedic for the treatment of patients with newly diagnosed FLT3-mutated AML in combination with standard chemotherapy for induction and consolidation and as monotherapy for maintenance treatment.20 The approval was based on the OS benefit with midostaurin plus chemotherapy versus placebo plus chemotherapy in patients with AML and an FLT3 mutation, as demonstrated in the RATIFY trial (Figure 2).21 Following the FDA and EMA authorization, the Swissmedic approved also gilteritinib,22 a more potent and specific FLT3 inhibitor, as a single agent for the treatment of patients who have relapsed or refractory (R/R) AML with FLT3 mutations. Efficacy was demonstrated in the international, controlled phase III ADMIRAL trial.23 In this study, 371 adult patients with R/R FLT3-mutated AML were randomized to receive either gilteritinib (n=247) or salvage chemotherapy (n=124). In the final analysis, gilteritinib was associated with significantly prolonged OS versus chemotherapy (9.3 months vs 5.6 months; HR: 0.64 [95% CI: 0.49−0.83]; p<0.001). Furthermore, the proportion of patients who achieved complete remission (CR) with full or partial hematologic recovery was 34.0% in the gilteritinib group and 15.3% in the chemotherapy group, with a CR rate of 21.1% and 10.5%, respectively. The follow-up analysis at a median follow-up of 37.1 months showed consistent superior median OS (Figure 3), with a 1-year OS rate of 36.6% with gilteritinib and 19.2% with chemotherapy and a 2-year OS rate of 20.6% and 14.2%, respectively.24 These results were corroborated in the phase III, open-label, multicenter COMMODORE trial on Asian patients with R/R FLT3-mutated AML after first-line therapy, which demonstrated that gilteritinib versus salvage chemotherapy significantly prolonged OS (median, 9.0 months vs 4.7 months; HR 0.549 [95% CI: 0.379−0.795]; p=0.00126) and event-free survival (EFS) (median, 2.8 months vs 0.6 months; HR 0.551 [95% CI: 0.395−0.769]; p=0.00004) in this patient population.25 The ongoing head-to-head HOVON 156 trial further aimed to compare the efficacy of gilteritinib and midostaurin when combined with intensive chemotherapy in fit patients with newly diagnosed AML.26

_in_admiral_at_a_median_follow-up_of_37.1_months.png)
Gilteritinib was also investigated in combination with azacitidine in newly diagnosed patients with FLT3-mutated AML ineligible for intensive induction chemotherapy.27 Although the trial did not meet the primary endpoint of OS and the key secondary endpoint of EFS, the composite CR (CRc) rates were significantly higher with gilteritinib plus azacitidine versus azacitidine alone (58.1% vs 26.5%; p<0.001).27 These results underline that achieving higher CR rates does not necessarily translate into better OS in elderly AML patients.
Several first- and second-generation FLT3 inhibitors are currently being investigated in phase II and phase III clinical trials, mostly in combination with chemotherapy.28 These include quizartinib, which provided a survival benefit and manageable toxicity profile versus chemotherapy in patients with R/R FLT3 ITD-positive AML.29 Furthermore, crenolanib, a potent type I pan-FLT3 inhibitor effective against both ITD and resistance-conferring tyrosine kinase domain (TKD) mutations, demonstrated clinical benefit in R/R AML patients both as monotherapy and in combination with the “7+3” regimen.30,31 In the phase II SORMAIN study, treatment with sorafenib, another multikinase inhibitor, led to a reduced risk of relapse and death after allogeneic hematopoietic cell transplantation (HCT) for FLT3-ITD-positive AML.32 Other emerging combinations also demonstrated anti-leukemic activity, including sorafenib plus azacitidine in patients with untreated or relapsed AML and FLT3-ITD,33,34 as well as quizartinib plus azacitidine/low-dose cytarabine (LDAC) in patients with FLT3-ITD-mutated myeloid leukemias, including AML.35 Quizartinib combined with decitabine and venetoclax was also shown to be active in heavily pretreated and prior FLT3 inhibitor-exposed patients with FLT3-ITD mutated AML in an ongoing, single-arm, open-label, phase I/II trial.36 Among those with R/R AML (n=23), the CRc rate was 78% and the median OS was 7.6 months. However, the additional benefit compared with decitabine and venetoclax remains to be clarified. Data also suggested that RAS/MAPK and FLT3 F691L mutations were associated with resistance to the treatment. There were no major safety signals and no grade ≥2 QTcF prolongation was reported.
IDH inhibition
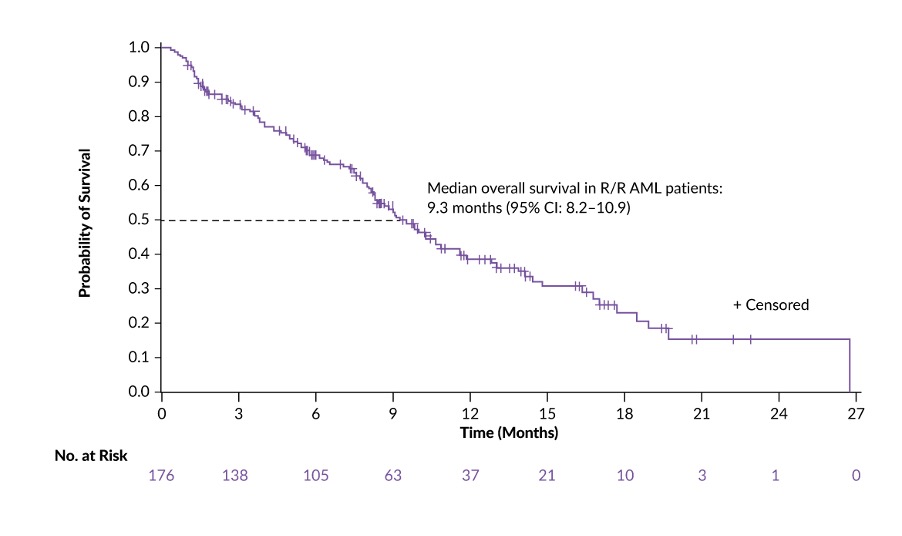
Mutations in the IDH1 and IDH2 genes are present in 8−15% of patients with AML and are associated with normal cytogenetic status.37,38 Authorized in 2017, enasidenib was the first IDH2 inhibitor that was approved for the treatment of adult patients with R/R AML harboring an IDH2 mutation,39 based on the results from the open-label, single-arm, phase I/II AG221-C-001 trial (Figure 4).40 The phase III, randomized, open-label IDHentify trial further compared enasidenib monotherapy with CCRs including intermediate-dose cytarabine (IDAC), LDAC, azacitidine or best supportive care (BSC) in older patients with late-stage IDH2-mutated R/R AML previously treated with multiple AML therapies.41 The study did not meet the primary point, as no statistically significant improvement in OS was shown among patients treated with enasidenib versus CCR. At the 2021 ASH Annual Meeting & Exposition, results were reported from post hoc analyses of this study that included patients preselected to lower-intensity azacitidine, LDAC or BSC only.42 The overall response rate (ORR) was substantially increased with enasidenib versus CCR (41% vs 11%), with CR rates of 26% and 3%, respectively, and rates of hematologic improvement of 41% and 13%, respectively (p<0.001 for all comparisons). Enasidenib versus CCR was also associated with prolonged OS (HR: 0.74 [95% CI: 0.56−0.97]; p=0.029) and EFS (HR: 0.68 [95% CI: 0.50−0.92]; p=0.011).
_aml_treated_with_enasidenib_i.jpg)
In 2019, the FDA approved ivosidenib, an IDH1 antagonist, as a single agent for the first-line treatment of adult patients with IDH1-mutant AML who are ≥75 years old or who have comorbidities that preclude intensive induction chemotherapy.43 This was due to data from the open-label, single-arm, phase I/II AG120-C-001 trial, which showed that ivosidenib monotherapy induced durable remissions, favorable OS outcomes (Figure 5) and transfusion independence in patients with newly diagnosed AML, with tolerable safety profile.44 The ongoing SAKK/HOVON 150 trial further aimed to assess whether ivosidenib or enasidenib can improve treatment outcomes in patients with newly diagnosed AML or myelodysplastic syndrome(MDS)-EB2 and an IDH1 or IDH2 mutation.45

Many phase I and II trials are currently investigating different combination therapies encompassing IDH1/2 inhibitors, with encouraging results. These include enasidenib plus azacitidine in IDH2-mutated newly diagnosed AML,46 ivosidenib in combination with azacitidine for newly diagnosed AML47 and ivosidenib plus venetoclax with or without azacitidine in IDH1-mutated myeloid malignancies.48 The efficacy and safety of ivosidenib plus azacitidine in patients with newly diagnosed AML with an IDH1 mutation was assessed in AGILE, a randomized, double-blind, phase III study on 146 patients who were randomized 1:1 to receive either ivosidenib plus azacitidine or placebo plus azacitidine.49 Results showed that ivosidenib-containing regimen significantly improved clinical outcomes compared with placebo-containing regimen, including EFS (HR: 0.33 [95% CI: 0.16−0.69]; p=0.0011), OS (median, 24.0 months vs 7.9 months; HR: 0.44 [95% CI: 0.27−0.73]; p=0.0005) and ORR (62.5% vs 18.9%; p<0.0001), with CR rates of 47.2% and 14.9% (p<0.0001), respectively, and CR plus partial hematologic recovery (CRh) rates of 52.8% and 17.6% (p<0.0001), respectively. However, it remains to be clarified whether combinations with IDH1/2 inhibitors are superior to those with venetoclax.
Combinations with BCL-2 inhibition
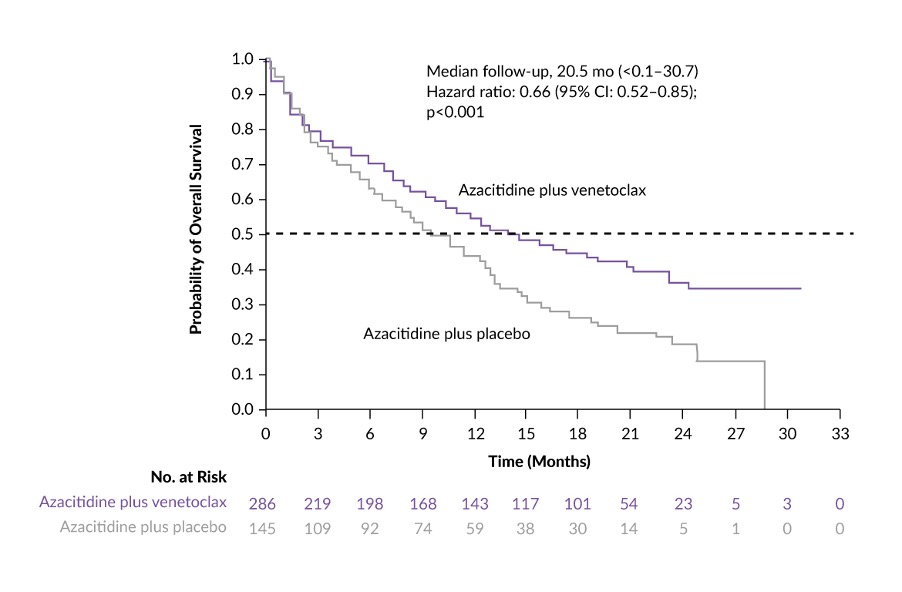
Targeted therapies may also be directed towards relevant pathways independent of mutational status. Swissmedic’s authorization of venetoclax50 in combination with an HMA (azacitidine or decitabine) or LDAC for the treatment of previously untreated AML in patients ineligible for induction chemotherapy, was based on the CR data of two open-label, non-randomized trials (Study M14-35851 and Study M14-38752) in this patient population. Efficacy was further confirmed in two randomized, double-blind, placebo-controlled trials. In VIALE-A, 431 patients underwent 2:1 randomization to receive venetoclax plus azacitidine (n=286) or placebo plus azacitidine (n=145).53 At a median follow-up of 20.5 months, the median OS was 14.7 months in the venetoclax-containing arm and 9.6 months in the placebo-containing arm (HR: 0.66 [95% CI: 0.52−0.85]; p<0.001) (Figure 6). Venetoclax-treated patients also achieved improved CR rate (37% vs 18% with placebo). The efficacy of venetoclax plus azacitidine versus azacitidine was also evaluated in a subgroup of untreated AML patients with poor-risk cytogenetics, with or without TP53 mutations. Analysis of pooled data from VIALE-A and a phase Ib trial of venetoclax plus azacitidine/decitabine presented at the 2021 ASH Annual Meeting & Exposition indicated improved CR plus CR with incomplete blood count recovery (CRi) rates in patients with wild-type versus mutated TP53 (70.0% vs 40.8%).54 Venetoclax plus azacitidine versus azacitidine alone was further associated with increased remission rates in patients with wild-type and mutated TP53, while this treatment regimen prolonged duration of response and OS only in patients with wild-type TP53.

In VIALE-C, patients were randomized to receive venetoclax plus LDAC (n=143) or placebo plus LDAC (n=68).55 At a median follow-up of 12.0 months, CR+CRi rates were 48% with venetoclax plus LDAC and 13% with LDAC alone with CR achieved in 27% and 7% of patients, respectively. At the primary analysis, the study did not meet its primary endpoint of OS. However, after an additional 6-months of follow-up, the median OS was 8.4 months in the venetoclax plus LDAC arm versus 4.1 months in the LDAC alone arm, corresponding to a 30% reduction in the risk of death with venetoclax (HR: 0.70 [95% CI: 0.50−0.99]; p=0.040).56
As an induction therapy, venetoclax plus decitabine was assessed in younger adults (range, 18−59 years) with newly diagnosed ELN adverse-risk AML in a prospective, multicenter, single-arm, phase II trial.57 Preliminary results showed a CRc rate of 76% with venetoclax plus decitabine versus 38% for historical controls, with a minimal/measurable residual disease (MRD) negativity rate after cycle 1 of 64%. At data cutoff, median progression-free survival (PFS) and OS were not reached. Compared with historical controls, venetoclax plus decitabine was associated with lower rates of infections, pneumonia and sepsis.
When combined with gilteritinib, venetoclax induced a high ORR in patients with FLT3-mutated AML, particularly in patients with previous exposure to FLT3 tyrosine kinase inhibitor (TKI), in a multicenter, open-label, phase Ib clinical trial.58 In the final report, the modified CRc rate, defined as CR plus CR with incomplete platelet recovery (CRp) plus CRi plus morphologic leukemia-free state (MLFS), was 79% in patients with FLT3-ITD-mutated AML, 78% in FLT3-mutated patients with prior TKI exposure and 75% in all FLT3-mutated patients.59 At a median follow-up of 15.1 months, the median OS in patients with FLT3-ITD-positive AML was 10 months. Of note, gilteritinib plus venetoclax achieved molecular clearance of FLT3 allelic burden <10-2 in 60% of patients with FLT3-ITD who attained modified CRc. Similarly, the treatment with venetoclax in combination with ivosidenib resulted in high ORR, with a CR rate of 44% and CR+CRi rate of 78% in patients with IDH1-mutated myeloid malignancies in a phase Ib/II study.60
Inhibition of Hedgehog signaling pathway
Both the FDA and EMA also approved glasdegib, a small molecule inhibitor of the Hedgehog signaling pathway, in combination with low-dose cytarabine for the treatment of patients aged at least 75 years or those ineligible for induction chemotherapy,61,62 based on OS benefit reported in the randomized, phase II BRIGHT AML 1003 trial (median, 8.3 months with glasdegib plus LDAC vs 4.3 months with LDAC alone; HR: 0.46 [95% CI: 0.30−0.71]; p=0.0002).63 At data cutoff, the ORR, defined as CR+CRi+MLFS, was 26.9% in the glasdegib plus LDAC arm and 5.3% in the LDAC alone arm, including CR rates of 17.9% versus 2.6%, respectively, and CRi rates of 6.4% versus 2.6%, respectively.
Immunotherapy for AML
Immunotherapies in AML include antibody-drug conjugates (ADCs), mono- and bispecific antibodies, dual affinity re-targeting (DART) molecules and cell-based approaches, including chimeric antigen receptor (CAR) T-cell therapy. In December 2019, the ADC gemtuzumab ozogamicin, an antibody against CD33, a myeloid differentiation antigen highly expressed in AML, combined with toxin calicheamicin, was authorized by Swissmedic in combination with daunorubicin and cytarabine (“7+3” regimen) for the treatment of newly diagnosed adult patients with CD33-positive AML.64 This approval was based on the randomized, open-label phase III ALFA-0701 trial, which included 271 patients aged 50−70 years who received induction therapy consisting of daunorubicin and cytarabine with (n=135) or without (n=136) gemtuzumab ozogamicin.65 At 2 years, the estimated median EFS rate was 40.8% with gemtuzumab ozogamicin and 17.1% with the control treatment (HR: 0.58 [95% CI: 0.43−0.78]; p=0.0003), while the OS rates were 53.2% and 41.9%, respectively (HR: 0.69 [95% CI: 0.49−0.98]; p=0.0368). The efficacy update showed that the final OS favored gemtuzumab ozogamicin, although statistical significance was not reached (median, 27.5 months vs 21.8 months; HR: 0.81 [95% CI: 0.60−1.09]; p=0.16).66 A meta-analysis of 5 randomized clinical trials (n=3,325) however showed improved OS rates in favorable-risk and intermediate-risk cytogenetics, with the best response in patients with favorable risk.67
Other immunotherapies for the treatment of AML are currently in clinical development. These include magrolimab, the first-in-class anti-CD47 antibody, in combination with azacitidine,68 and cusatuzumab,69 an anti-CD70 antibody, which both demonstrated promising anti-tumor activity in previously untreated patients with AML in phase I studies; data from ongoing phase II and III clinical trials of these two agents are awaited.70,71 Magrolimab has also been assessed in combination with azacitidine and venetoclax in a phase I/II study on patients with newly diagnosed older/unfit or high-risk AML and R/R AML.72 Data showed that the triplet as frontline therapy yielded a CR rate of 64% regardless of TP53 status, with ORR rates of 86% in TP53-mutated and 100% in wild-type TP53 patients. In the R/R cohort, the CR+CRi rates were 63% among venetoclax-naïve patients and 20% among those with prior venetoclax exposure. Two phase III trials of magrolimab combinations are ongoing: ENHANCE-2 on previously untreated patients with TP53-mutated AML and ENHANCE-3 on newly diagnosed AML patients ineligible for intensive chemotherapy.73,74 Potential relevant toxicity include hemolysis of CD47-expressing erythrocytes, which need very careful monitoring during the initial cycles.
Similarly, the open-label, multicenter, phase Ib ELEVATE study aimed to test cusatuzumab combined with venetoclax and azacitidine in patients with previously untreated AML who are not eligible for intensive chemotherapy.75 After a median follow-up of 40 weeks, 77% of patients achieved CR+CRi, with an MRD negativity rate of 50%.
Encouraging results were also reported from the clinical studies investigating the combination of nivolumab, an anti-programmed cell death protein (PD-1) antibody, and ipilimumab, an anti-cytotoxic T lymphocyte antigen-4 (CTLA-4) antibody,76 as well as sabatolimab, a high-affinity antibody targeting TIM-3, in patients with newly diagnosed AML.77
Among bispecific antibodies that are being tested in clinical trials, flotetuzumab, a DART antibody that simultaneously recognizes CD123, another attractive target antigen in AML, and CD3, demonstrated clinical benefit in patients with primary induction failure (PIF) or early relapse (ER), with an acceptable safety profile, in an open-label, phase I/II study in 88 adults with R/R AML.78 CD123 has become an important target also in designing CAR T-cell therapies.79
Although CAR T-cell therapy demonstrated efficacy in certain hematological malignancies, its antitumor activity in AML patients has been unsatisfactory. To date, CAR T-cell therapies directed against CD33, CD123, CLL-1, NKG2D, Lewis-Y and CD19 have been investigated in 65 AML patients with PIF or ER in 13 clinical trials.80 Overall, 17 patients achieved CR, CRi or CR+CRh and 11 of them were negative for MRD.
Despite some promising results, immunotherapy for treating AML has several challenges, including the lack of specific targets on AML cells, the antigenic shift and the need for the protection of healthy hematopoiesis, as well as the heterogeneity within the AML stem and progenitor cell compartments. However, immunotherapy is an emerging strategy for AML and will be further investigated in ongoing trials.
Targeting epigenetic alterations in AML
A large proportion of AML patients harbors no targetable mutations, indicating an important role of epigenetic processes in the disease pathogenesis. Data showed that genes regulating DNA methylation are frequently mutated in AML and that epigenetic alterations may be associated with the aggressive phenotype of AML.81,82 Driver mutations were identified in genes affecting epigenetic modifiers, such as histone modification (EZH2, ASXL1) and DNA methylation (DNMT3A, TET2). Several agents targeting the epigenetic machinery in AML have already received regulatory approval or are currently being investigated in clinical trials.83 Azacitidine and decitabine, also approved in Switzerland, are HMAs that have become the standard of care for patients with AML and high-risk MDS who are unfit for intensive induction chemotherapy. The favorable survival outcomes observed with HMAs in selected patient populations in clinical trials indicated that HMAs are among the most advanced epigenetic cancer therapies with significant therapeutic potential in AML.84,85
Recent data also showed that the oral formulation of azacitidine, known as CC-486, is effective and well-tolerated as maintenance therapy in hematopoietic stem cell transplantation (HSCT)-ineligible patients with AML in first remission following induction chemotherapy. In the phase III, double-blind, placebo-controlled QUAZAR AML-001 trial, patients receiving CC-486 versus placebo experienced significantly prolonged overall and relapse-free survival.86 At a follow-up of 51.7 months, the median OS was maintained, with 5-year OS rates of 26% with azacitidine and 19.2% with placebo (HR: 0.69 [95% CI: 0.56−0.86]; p=0.0008).87 Results from QUAZAR AML-001 led to the authorization of oral azacitidine by Swissmedic.88
There are many other epigenetic therapies under clinical development, such as panobinostat and vorinostat, two histone deacetylase (HDAC) inhibitors that have demonstrated anti-tumor activity in preclinical AML models in combination with other drugs.89 Other investigational treatments include histone methyltransferase inhibitors (i.e., pinometostat, a DOT1L inhibitor),90 bromodomain-containing protein inhibitors (OTX015, BI-7273)91,92 and histone demethylase inhibitors (tranylcypromine, an Lysine Demethylase 1 [LSD1]-inhibitor).93 These therapies showed encouraging results in AML in early-phase clinical studies, mostly in combination with either conventional chemotherapy, other epigenetic or targeted therapy, or immunotherapy.85
Monitoring disease progression with MRD
Treatment response monitoring is an important tool to predict clinical outcomes in AML patients.94 However, the predictive value of MRD in guiding treatment decisions has not yet been established by prospective studies95 and the ELN MRD Working Party thus recommends ≥10-fold increase in MRD as an indicator for therapy requirement.96 In December 2021, updated ELN MRD recommendations were published and important modifications include technical specifications for NGS-based MRD testing and integrative assessments of MRD irrespective of technology.97 The new guidelines also include the clinical implementation of MRD assessment, such as the use of MRD as a prognostic risk factor and as a monitoring tool to identify impending relapse, as well as a potential surrogate endpoint for OS in clinical trials. In addition, the 2021 ELN MRD recommendations incorporate the selection of MRD detection technique, technical requirements for flow- and molecular-MRD analysis, biological material and appropriate time points for MRD assessment.
Studies have shown that MRD relapse, now defined as either conversion of MRD negativity to MRD positivity independent of the MRD technique or increase of MRD ≥1 log10 between any two positive samples measured in the same tissue,97 can be induced by an extremely low level of residual leukemic cells.98 These residual cells can be detected by several sensitive methods, including the conventional flow cytometric technologies and real-time (RT) quantitative polymerase chain reaction (qPCR) or newer technologies such as multiparametric flow cytometry (MFC), digital droplet (dd) PCR and NGS.99 The obtained information on MRD can help guide risk-adapted management and predict clinal outcomes in AML patients, resulting in the incorporation of MRD into clinical algorithms for some hematological malignancies like AML, multiple myeloma, acute lymphocytic leukemia (ALL) and chronic lymphocytic leukemia (CLL).97,100 The high prognostic impact of MRD assessed by flow cytometry has been indicated in the HOVON/SAKK AML 42A Study, which showed that low MRD values distinguished patients with relatively favorable clinical outcomes from those with a high probability of relapse and worse relapse-free and overall survival.101 A study conducted by Jongen-Lavrencic et al. (2018) further demonstrated that the detection of molecular MRD during CR had significant independent prognostic value regarding relapse and survival rates.102 Finally, a meta-analysis evaluating the association between MRD status and survival outcomes in AML patients suggested that achieving MRD negativity is associated with superior disease-free survival and OS in patients with AML, with the value of MRD negativity being consistent across age groups, AML subtypes, time of MRD assessment, specimen source and MRD detection methods.103
Although intensive induction chemotherapy can provide complete remission in most patients with newly diagnosed AML, relapse rates remain above 50%, mainly due to the emergence of resistant clones.104,105 Thus, MRD monitoring during the treatment course is important for prognosis assessment and subsequent management, such as intensive chemotherapy, stem cell transplantation and participation in clinical trials.97 In MRD-negative patients with favorable-risk and core-binding factor (CBF) AML, autologous stem cell transplantation (ASCT) is a potent anti-leukemic therapy.106 Furthermore, patients with intermediate- or unfavorable-risk disease at the time of diagnosis, such as FLT3-ITD-positive or complex karyotype, who achieved MRD-negativity during therapy should receive allogeneic SCT.107 The ELN guidelines however suggest considering ASCT for MRD-negative patients with intermediate or adverse genetics and a high risk of treatment-related mortality in the first CR.13 Indeed, a recent study demonstrated that MRD status is especially clinically relevant for informed treatment choice in intermediate-risk AML.108 For those who remain MRD-positive after consolidation, emerging data suggest that allogeneic transplantation is associated with unfavorable outcomes.109 According to 2021 ELN MRD recommendations, ELN intermediate-risk patients with MRD negativity in bone marrow after two cycles of chemotherapy should be considered for consolidation chemotherapy or ASCT.97 All eligible ELN adverse risk patients should undergo allogeneic SCT, regardless of MRD status. Furthermore, MRD positivity and/or MRD relapse at the end of treatment, during maintenance and follow-up are associated with poor clinical outcomes and should lead to consideration of salvage treatment options, including allogeneic HCT.
Biomarkers for MRD assessment
State-of-the-art technologies revealed lots of AML biomarkers suitable for MRD assessment through the identification of highly specific leukemia-associated immunophenotypes (LAIP) by MFC and rare genetic mutations by digital PCR and NGS. In AML, MRD monitoring typically includes quantification of NPM1-mutated, PML-RARA, RUNX1-RUNX1T1 and CBFB-MYH11 by using RT-qPCR.97 In particular, NPM1 mutations, which are present in about half of the AML patients with a normal karyotype, are constant at diagnosis and relapse, making them ideal leukemia-specific targets for MRD assessment.110 The clinical relevance of NPM1 monitoring has been shown in clinical trials in patients with NPM1-mutated AML,111 which is currently recognized as a distinct entity due to its unique biological and clinical features. Similar findings were reported for the PML-RARA, RUNX1-RUNX1T1 and CBFB-MYH11 fusion transcripts, with increased levels after consolidation therapy and during remission being predictive of relapse risk.99 Based on these data, the ELN Working Party consensus document recommends molecular MRD assessment through quantification of NPM1 mutations, as well as PML-RARA, RUNX1-RUNX1T1 and CBFB-MYH11 fusion transcripts in AML patients at diagnosis, at least after 2 cycles of induction/consolidation chemotherapy and every 3 months (for 24 months) after the end of consolidation.97 Ongoing molecular MRD monitoring beyond 24 months of follow-up should be based on individual clinical features.
Conclusions
In the past few years, the introduction of more effective and less toxic targeted therapies, better understanding of disease biology, refined diagnostic criteria and new advanced tools for disease monitoring have improved response rates and survival of patients with acute myeloid leukemia (AML). The personalized approach, which provides the opportunity to deliver treatments tailored to each patient, has achieved clinical benefit in a proportion of patients with AML, especially of those who do not respond to intensive chemotherapy regimens or cannot tolerate them. AML, however, remains incurable in most cases and allogeneic stem cell transplantation (SCT) is still an important treatment option. To fill this medical need, many investigational therapies, including new targeted agents and immunotherapy, are currently being investigated, including mono- and bispecific antibodies, cell-based therapies and immune checkpoint inhibitors.
CONFLICTS OF INTEREST
The authors declare that they have no conflict of interest.
Author Contributions
All authors contributed to and approved the final manuscript.
Acknowledgments
Writing and editing assistance was provided by H+O communications Ltd., Zurich, Switzerland.
Disclosures
TBC