Early and advanced triple-negative breast cancer
Although the development of novel therapeutics resulted in prolonged survival, triple-negative breast cancer (TNBC) is still associated with the worst prognosis among all clinical subtypes of breast cancer. In the early-stage disease, neoadjuvant chemotherapy has been established as the current standard treatment but the risk for recurrence and high mortality remain.1 As a potential novel treatment strategy, the combination of immunotherapy and chemotherapy in the (neo)adjuvant approach has been explored in patients with early TNBC. In the randomized, double-blind, phase III KEYNOTE-522 trial, patients with previously untreated stage II or stage III TNBC underwent 2:1 randomization to receive neoadjuvant chemotherapy with paclitaxel and carboplatin plus either 4 cycles of pembrolizumab, a programmed cell death protein 1 (PD-1) inhibitor, every 3 weeks (n=784) or placebo (n=390), followed by 4 cycles of pembrolizumab or placebo, respectively, in combination with doxorubicin or epirubicin and cyclophosphamide.2 After definitive surgery, patients received adjuvant pembrolizumab or placebo every 3 weeks for up to 9 cycles. At the first interim analysis, pembrolizumab versus placebo was associated with a significantly increased rate of pathological complete response (pCR) (64.8% vs 51.2%; p=0.00055) (Table 1). The addition of pembrolizumab to chemotherapy also led to a statistically significant and clinically meaningful improvement in event-free survival (EFS), with 36-month EFS rates of 84.5% and 76.8%, respectively (HR: 0.63 [95% CI: 0.48−0.82]; p=0.00031). Data of five additional EFS sensitivity analyses, presented during the 2021 SABCS, were consistent with these results and corroborated the robust treatment benefit in this patient setting.3 Interestingly, a similar benefit was recorded for patients with programmed death-ligand 1 (PD-L1)-positive and PD-L1-negative tumors. Pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab also improved EFS outcomes in all prespecified subgroups, including nodal status, disease stage and menopausal status. At a median follow-up of 39.1 months, the overall survival (OS) rates were 89.7% with pembrolizumab and 86.9% with placebo (Table 1), but OS data were immature at this timepoint. Based on these results, the addition of immunotherapy to neoadjuvant chemotherapy is a potential new standard of treatment in early TNBC. In Table 1, features and outcomes of other main randomized trials on chemoimmunotherapy in early-stage TNBC are also presented.4
At the 2021 SABCS, Turner et al. presented an approach that aimed at screening for molecular recurrent disease by detection of circulating tumor (ct) DNA and incorporation of immune checkpoint inhibition at the time of relapse with minimal recurrent tumor burden. In the prospective, phase II c-TRAK TN trial, patients with trackable mutations who completed surgery and adjuvant chemotherapy underwent ctDNA testing at baseline and every 3 months for 1 year.9 At 12 months, 44/161 (27.3%) patients were ctDNA-positive, with significantly more patients with high-risk versus moderate-risk disease (55.7% vs 11.8%). These patients were randomized 2:1 between observation with continued standard follow-up (n=14) and intervention (staging and pembrolizumab every 3 weeks for 1 year) (n=32). However, the rate of overt metastatic disease on staging at the time of ctDNA detection was 71.9%. Out of 9 patients who were ctDNA-positive and staging negative, 5 initiated pembrolizumab. One patient remained on treatment, while 3 discontinued due to recurrence and 1 discontinued due to adverse events (AEs). Of note, none of these patients exhibited sustained ctDNA clearance after 6 months on pembrolizumab. Among patients assigned to observation, the median time to relapse was 4.1 months, which is shorter than previously reported in retrospective studies. The investigators concluded that these findings might have implications for future trial design and indicate the importance to start ctDNA testing early and to employ more sensitive ctDNA assays that track multiple variants. The ongoing clinical phase III ZEST trial currently assesses treatment with the PARP inhibitor niraparib after detection of ctDNA in patients with BRCA-mutated human epidermal growth factor 2 (HER2)-negative breast cancer or TNBC with the molecular disease.10
Pembrolizumab in combination with chemotherapy was also investigated in patients with previously untreated locally recurrent inoperable or metastatic TNBC in the phase III KEYNOTE-355 trial. Previous reports showed that pembrolizumab plus chemotherapy versus placebo plus chemotherapy improved progression-free survival (PFS) (HR: 0.66 [95% CI: 0.50–0.88]) and OS (HR: 0.73 [95% CI: 0.55–0.95]; p=0.0093) in patients with PD-L1-positive tumors (composite positive score [CPS] ≥10).11,12 No significant improvement in OS outcomes was reported with pembrolizumab plus chemotherapy compared with chemotherapy alone in patients with a CPS ≥1. The recent subgroup analyses by different PD-L1 CPS cutoffs showed no significant OS differences between the two treatment strategies.13 More specifically, OS was similar in the subgroups with PD-L1 CPS scores of <1 and 1−9 for pembrolizumab and placebo, although there were trends towards improved OS outcomes with pembrolizumab in the CPS 10−19 (HR: 0.71 [95% CI: 0.46−1.09]) and CPS ≥20 (HR: 0.72 [95% CI: 0.51−1.01]) subgroups. The subgroup analysis further showed favorable PFS outcomes among patients receiving pembrolizumab-based versus placebo-based therapies in the CPS ≥20, CPS 10−19 and CPS 1−9 groups. Altogether, the results of this analysis suggest that CPS ≥10 could be an optimal cutoff to define patients who are expected to benefit from this treatment regimen in the metastatic setting.
HR-positive, HER2-negative breast cancer
The standard of care for patients with advanced hormone receptor (HR)-positive, HER2-negative breast cancer are cyclin-dependent 4/6 kinase (CDK4/6) inhibitors in combination with endocrine therapy (ET).14 Currently, there are three approved CDK4/6 inhibitors: ribociclib, palbociclib and abemaciclib.
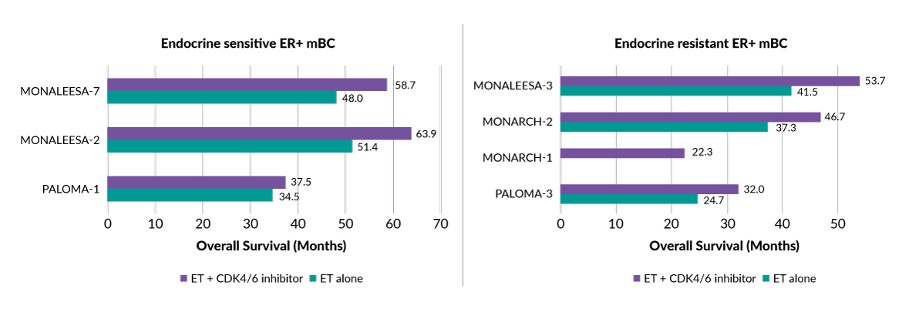
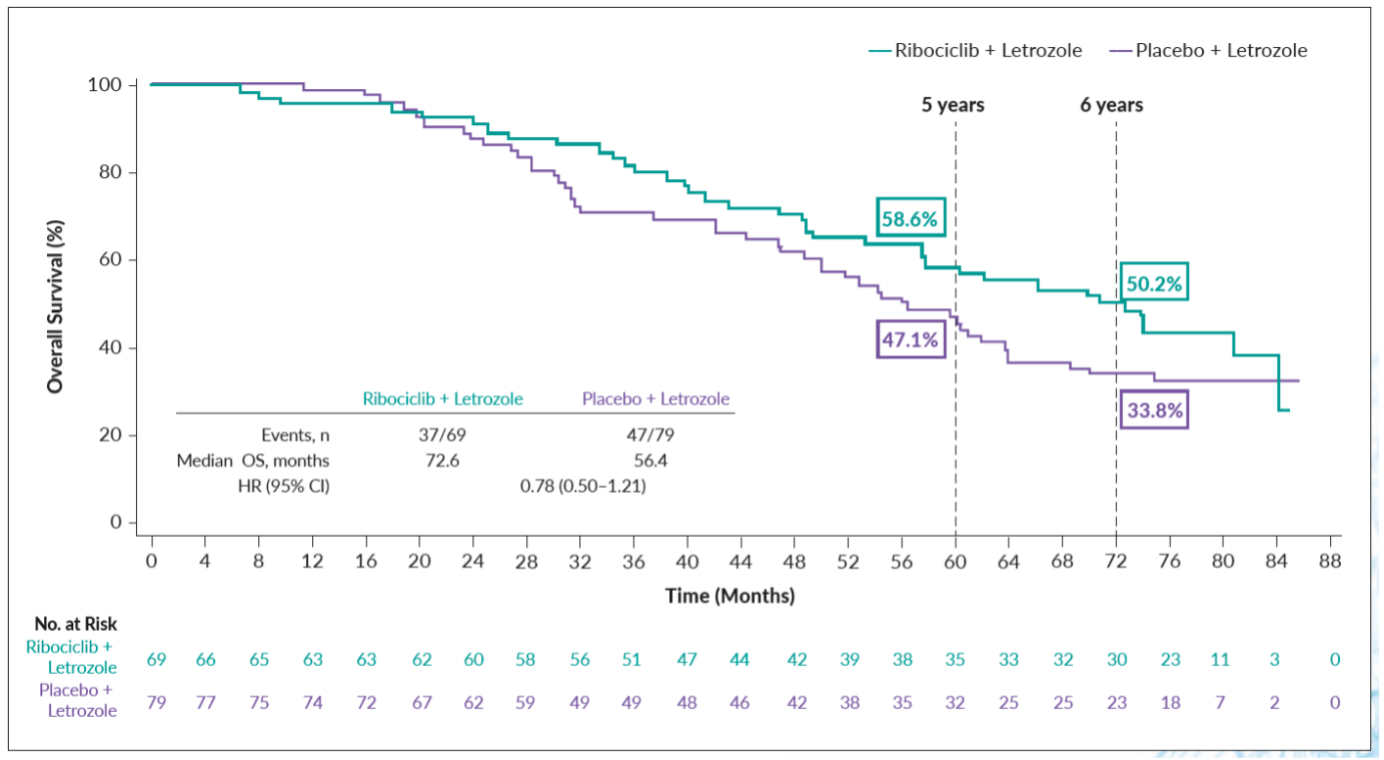
Ribociclib was assessed in the international, double-blind, randomized phase III MONALEESA-2 trial on postmenopausal patients with advanced HR-positive, HER2-negative breast cancer who had no prior therapy for advanced disease.15 Overall, 668 patients were randomized to receive either ribociclib plus letrozole (n=334) or placebo plus letrozole (n=334). The primary analysis showed that ribociclib plus letrozole compared with placebo plus letrozole significantly prolonged PFS, with a higher rate of myelosuppression in the ribociclib group.15,16 The final OS analysis at a median follow-up of 80 months further demonstrated that ribociclib plus letrozole was associated with significantly improved median OS of 63.9 months versus 51.4 months for placebo plus letrozole (HR: 0.76 [95% CI: 0.63−0.93]; p=0.004) (Figure 1), with estimated 6-year survival rates of 44.2% and 32.0%, respectively.17 This OS benefit with ribociclib versus placebo was preserved across prespecified subgroups, including bone-only metastases (6-year OS rate, 50.2% vs 33.8%) (Figure 2), liver metastases (31.0% vs 18.9%), lung metastases (40.5% vs 31.2%) and ≥3 metastatic sites (37.9% vs 24.2%).18 When stratified by prior (neo)adjuvant therapy, 6-year OS rates were improved with ribociclib versus placebo regardless of the receipt of prior chemotherapy or ET such as aromatase inhibitor (AI) or tamoxifen. These additional findings corroborated the significant survival benefit of ribociclib plus letrozole in first-line advanced HR-positive, HER2-negative breast cancer, further supporting the use of upfront ribociclib plus letrozole in this patient population. Figure 1 summarizes OS outcomes also with other CDK4/6 inhibitors reported in clinical trials on patients with HR-positive, HER2-negative breast cancer.19–24
_of_cdk4_6_inhibitors_in_clinical_trials.jpg)
_in_patients_with_metastases_in_the_bone_only.png)
Another presentation given during the 2021 SABCS reported the results of a retrospective, exploratory analysis investigating the association between intrinsic subtype and OS in patients treated with ribociclib plus ET in the MONALEESA-2, -3, and -7 trials.17,25–27 The present analysis included 585 samples from patients treated with ribociclib plus ET and 412 from patients treated with placebo plus ET.25 Ribociclib provided an OS benefit in both, the intention-to-treat (ITT) (n=2,066) (HR: 0.76 [95% CI: 0.67−0.86]; p<0.0001) and biomarker (n=997) (HR: 0.75 [95% CI: 0.63−0.89]; p=0.0012) populations. There was a strong association between intrinsic subtype and OS for patients treated within the placebo arms and those treated within the ribociclib arms. The median OS for subpopulations receiving placebo was as follows: luminal A: 54.6 months; luminal B: 44.9 months; HER2-enriched: 29.4 months; basal-like: 21.2 months. Compared with placebo, the median OS was improved with ribociclib in patients with luminal A (68.0 months), luminal B (58.8 months) and HER2-enriched (40.3 months) subtypes, but not basal-like (19.4 months). Using luminal A as the referent population, multivariable models showed that the intrinsic subtype was associated with OS outcomes. The adjusted HRs for death in the placebo arms were 1.47 for luminal B (p=0.013), 2.87 for HER2-enriched (p<0.001) and 2.35 for basal-like (p=0.012) subtypes. In the ribociclib arms, the adjusted HRs were 1.16 for luminal B (p=0.32), 1.83 for HER2-negative enriched (p=0.00023) and 7.06 for basal-like (p<0.0001) subtypes. Kaplan-Meier curves also demonstrated the benefit with ribociclib versus placebo in the subtypes of luminal A, luminal B and HER2-enriched, but not in the basal-like subtype. Efficacy of ribociclib plus ET in patients with HER2-enriched subtype is further investigated in the head-to-head phase III HARMONIA trial.28
Palbociclib plus ET yielded improved survival outcomes versus placebo plus ET in the phase III PALOMA-2 and PALOMA-3 studies on treatment-naïve and ET-pretreated patients, respectively, with advanced HR-positive, HER2-negative breast cancer (Figure 1).20,29,30 However, no survival benefit was observed with adjuvant palbociclib plus ET in patients with stage II−III HR-positive, HER2-negative early breast cancer, according to the final results from the randomized phase III PALLAS trial.31 In this study, patients were randomized to receive either palbociclib for 2 years in combination with adjuvant ET (n=2,884) or adjuvant ET alone for at least 5 years (n=2,877). At a median follow-up of 31 months, 4-year invasive disease-free survival (iDFS) rates were 84.2% versus 84.5%, respectively (HR: 0.96 [95% CI: 0.81–1.14]; p=0.65). There was also no difference across subgroups, including anatomic staging, T-stage, N-stage, grading, neo/adjuvant chemotherapy, age group and clinical risk. Treatment with palbociclib-containing therapy versus ET alone yielded comparable 4-year rates of invasive breast cancer-free survival (85.4% vs 86.0%) and distant recurrence-free survival (86.2% vs 87.8%). The authors of the study offered potential explanations for the lack of activity of ribociclib in combination with adjuvant ET, including the treatment schedule and the strict rules regarding dose reductions and study drug termination.
Although the introduction of CDK4/6 inhibitors dramatically changed the management of advanced HR-positive, HER2-negative breast cancer, intrinsic and acquired resistance to these agents is a persistent clinical challenge.32 Samuraciclib, an investigational CDK7 inhibitor, in combination with standard dose fulvestrant showed encouraging antitumor activity in patients with advanced HR-positive breast cancer that is resistant to CDK4/6 inhibitors in a small study, which was presented at the 2021 SABCS.33 All included patients had previously received an AI and a CDK4/6 inhibitor for advanced disease. Among evaluable patients (n=25), 72% experienced tumor shrinkage, with 12% achieving a partial response (including one that lasted for about 1 year) and 52% having stable disease. The 24-week clinical benefit rate was 36% in the overall population, 55% in patients without liver metastases and 53% in those with TP53 wild-type disease. Patients who had no liver metastases had also pronounced survival benefit, with a median PFS of at least 48 weeks versus 11.9 weeks in patients with liver metastases (HR: 0.16 [95% CI: 0.05–0.59]; p=0.0021). Similarly, median PFS was significantly longer in patients with wild-type versus mutated TP53 tumors (32 weeks vs 7.9 weeks; HR: 0.17 [95% CI: 0.05−0.53]; p=0.0008). Notably, most of the patients who progressed had TP53 mutant disease and all of the responders were TP53 wild-type. Based on these results, samuraciclib has been granted Fast Track designations by the food and drug administration (FDA) for use in combination with fulvestrant for the treatment of CDK4/6 inhibitor-resistant advanced HR-positive, HER2-negative breast cancer.34
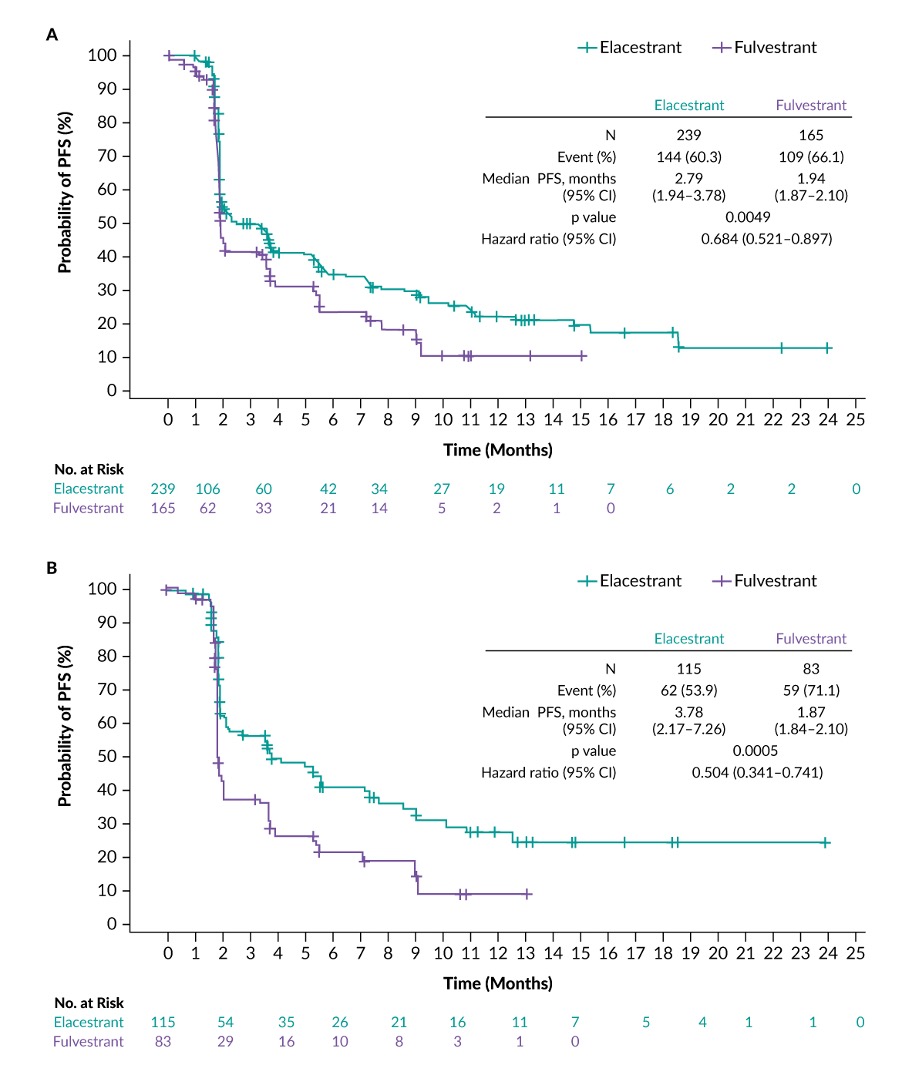
The estrogen receptor (ER) is an important therapeutic target in ER-positive breast cancer and fulvestrant is the only selective estrogen receptor degrader (SERD) currently approved in the metastatic setting. The clinical efficacy of fulvestrant is however limited by its poor oral bioavailability and the need for intramuscular administration.35 Therefore, there is a high unmet medical need for a potent oral SERD for the treatment of ER-positive breast cancer. Among several oral SERDs currently in development, elacestrant is the first oral SERD that showed positive clinical outcomes in patients with advanced or metastatic ER-positive, HER2-negative breast cancer. This agent was investigated in the open-label, phase III EMERALD trial that randomized 477 postmenopausal women who had been treated with 1−2 prior lines of ET and progressed on a CDK4/6 inhibitor, to receive either elacestrant (n=239) or the standard of care (SOC) (fulvestrant or AI) (n=238).36 Among all patients, 228 had tumors with mutations in the estrogen receptor (ESR1) gene (elacestrant, n=115; SOC, n=113). The study met both its co-primary endpoints of improved PFS with elacestrant versus SOC in the ITT population (HR: 0.697 [95% CI: 0.552–0.88]; p=0.0018) (Figure 3A) and the subgroup of patients with ESR1 mutations (HR: 0.546 [95% CI: 0.387–0.768]; p=0.0005) (Figure 3B). The 12-month PFS rates were 22.3% with elacestrant and 9.4% with SOC for all patients, with respective rates of 26.8% and 8.2% in the mutated ESR1 group. This PFS benefit was preserved in key prespecified subgroups, including visceral metastases, number of prior lines of therapy and pretreatment with fulvestrant. A prespecified interim OS analysis demonstrated a numerical trend favoring elacestrant over SOC in the ITT population (HR: 0.751 [95% CI: 0.542–1.038]; p=0.0821), as well as among patients with ESR1 mutations (HR: 0.592 [95% CI: 0.361–0.958]; p=0.0325). The final OS analysis is expected next year. According to the investigators, further elacestrant combinations in earlier lines with other targeted therapies, including CDK4/6 inhibitors and mTOR inhibitors, are ongoing and/or planned in this patient setting.

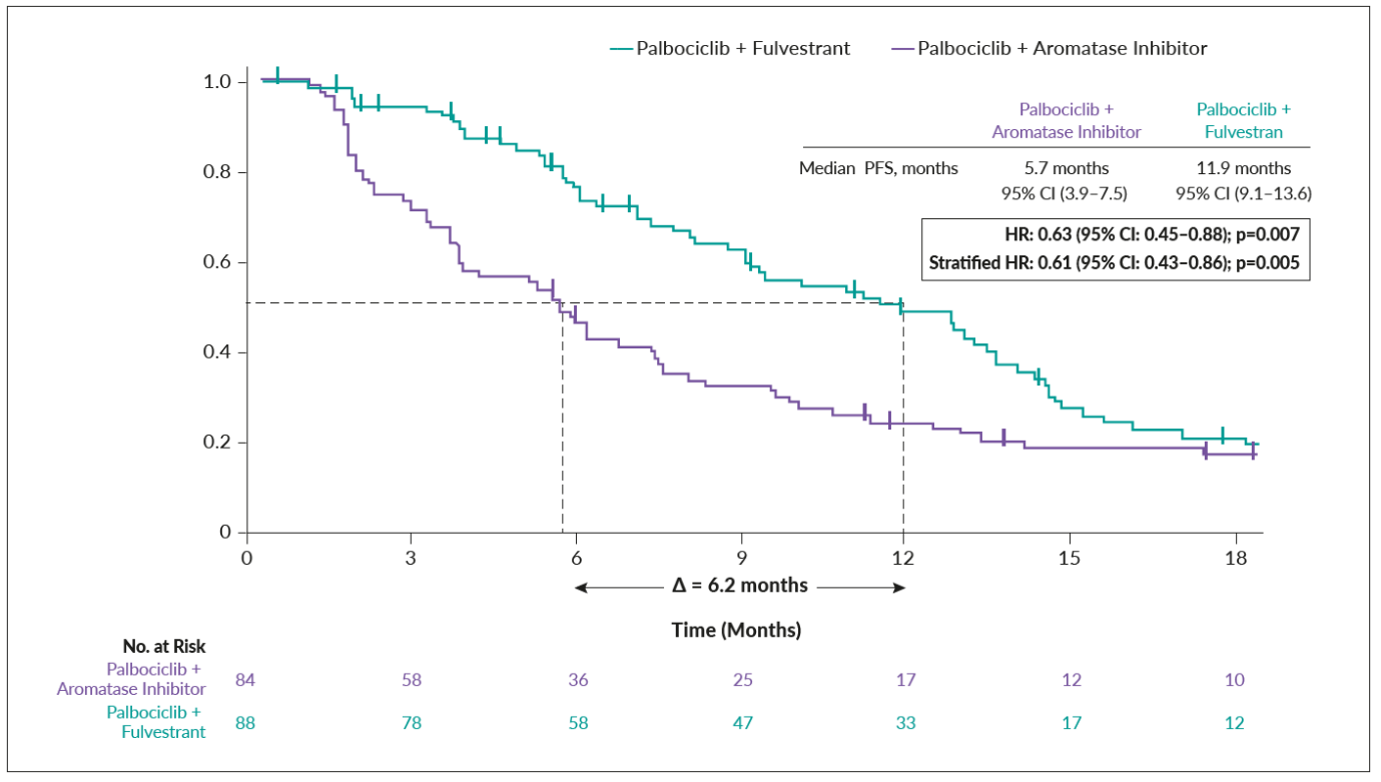
Although ESR1 mutations retain sensitivity to SERDs, they are a common cause of acquired resistance to AI-based therapy and are associated with worse survival outcomes in patients with metastatic HR-positive, HER2-negative breast cancer. ESR1 mutations can be detected in the blood by cell-free circulating DNA analysis and are typically present in less than 5% of patients at metastatic relapse and 30−40% of patients at progression following first-line AI-based therapy.37,38 The clinical utility of blood ESR1 mutation monitoring was demonstrated in the phase III PADA-1 trial, indicating that this patient population can derive clinical benefit from switching from an AI to fulvestrant in combination with palbociclib when an ESR1 mutation is detected before tumor progression.39 This multicenter study included 1,017 women who were treated with an AI plus palbociclib as frontline therapy and provided blood samples at baseline, after 1 month and every 2 months until progression. After a median follow-up of 15.6 months, 172 patients had rising ESR1 mutations but no evidence of disease progression. These women were randomized to either continue with standard AI plus palbociclib (n=84) or to switch to fulvestrant plus palbociclib (n=88). At a subsequent median follow-up of 26.0 months, the median PFS was 11.9 months in the fulvestrant arm and 5.7 months in the standard therapy arm, translating into 37%-reduced risk for disease progression or death (stratified HR: 0.61 [95% CI: 0.43–0.86]; p=0.005) (Figure 4). In total, 69 patients who received an AI plus palbociclib developed progressive disease and 47 patients crossed over to the fulvestrant plus palbociclib arm. At a median follow-up of 14.7 months, the median PFS was 3.5 months in the cross-over cohort. In conclusion, PADA-1 is the first trial to demonstrate that resistance-associated mutations in the ESR1 gene can be detected and targeted before tumor progression. By adopting this strategy in clinical practice, switching to fulvestrant during the first-line therapy when ESR1 mutations have emerged and before disease progression might provide a considerable benefit for the patients.
_in_the_phase_iii_pada-1_trial_in_patients_receiving_fulves.png)
Metastatic HER2-positive breast cancer
Trastuzumab deruxtecan (T-DXd) is a HER2-targeting antibody-drug conjugate (ADC) that demonstrated durable antitumor activity in patients with previously treated metastatic HER2-positive breast cancer in the single-arm, phase II DESTINY-Breast01 trial,40 which led to its global regulatory approval. The open-label, randomized, phase III DESTINY-Breast03 trial further demonstrated clinically meaningful and statistically significant improvement in PFS with T-DXd versus trastuzumab emtansine (T-DM1) in this patient population (median, not reached vs 6.8 months; HR: 0.28 [95% CI: 0.22−0.37]; p=7.8x10-22).41 Recent analyses showed that this PFS benefit was maintained regardless of HR status, prior pertuzumab use, number of prior lines of therapy and the presence of visceral disease.42 In addition, median PFS was considerably prolonged among patients with brain metastases at baseline treated with T-DXd versus T-DM1 (15 months vs 3 months; HR: 0.25 [95% CI: 0.13−0.45]), as well as among those without brain metastases at baseline (not reached vs 7.1 months; HR: 0.30 [95% CI: 0.22–0.40]). T-DXd was also associated with substantial intracranial response and reduction in central nervous system disease, with an intracranial objective response rate of 63.9% compared with 33.4% for T-DM1 and a complete response rate of 27.8% versus 2.8%, respectively. The authors pointed out that the activity of T-DXd in patients with stable baseline brain metastases is encouraging and may provide another potential option for those with disease progressing on currently available therapies. Further exploration of the activity of T-DXd is ongoing and the DESTINY-Breast12 trial is currently recruiting patients with and without active brain metastases within two prospective cohorts.