
Introduction
In 2020, liver cancer was the 6th most commonly diagnosed cancer (~905.000 new cases) and the 3rd leading cause of cancer death (~830.000 deaths) worldwide.1 However, the incidence of liver cancer varies considerably between different geographic regions, with the highest incidence rates in Asia and Africa and the lowest rates in Europe and North America. This discrepancy originates mainly from regional differences in risk factors for the disease. With 1,103 new cases in 2020, liver cancer ranked only as the 13th most frequently diagnosed cancer in Switzerland, but the impact on cancer mortality was disproportionally higher with 913 deaths, as liver cancer was the 6th cause of cancer death.2
Hepatocellular carcinoma (HCC) is the most common type of liver cancer and accounts for about 85% of cases, followed by cholangiocarcinoma with 15% of cases.1 The pathophysiology of HCC is a complex multistep process that involves different factors including genetic predisposition, the interplay between viral and non-viral risk factors, various immune cells and the severity of the underlying chronic liver disease.3 The main risk factors for the development of HCC are chronic infections with hepatitis B virus (HBV) (~60% of HCC cases in Asia [excluding Japan], South America and Africa) or hepatitis C virus (HCV) (in Western Europe, North America and Japan), alcoholic liver disease and nonalcoholic fatty liver disease (NAFLD), aflatoxin-contaminated foods, excess body weight, type 2 diabetes and smoking.4 Most HCC patients also have cirrhosis, which is primarily caused by infection with HBV and HCV and is the strongest risk factor for HCC.5,6 Another common risk factor for cirrhosis is non-alcoholic steatohepatitis (NASH), which is involved in the development of HCC in patients with diabetes mellitus or obesity. In addition, chronic liver diseases are associated with inflammation that eventually leads to immunosuppression and the development of HCC.5,7 Male gender is another risk factor for HCC, as both incidence and mortality rates are 2−3 times higher among men than women in most countries. The risk for the disease also increases with older age, with the highest age-specific incidence reported in people older than 70 years.4,8
Several cancer driver oncogenes recurrently altered in HCC have recently been identified. The most common driver gene alterations are telomerase activation via TERT promoter mutations, considered as an early event in tumor stage progression, while FGF3, FGF4, FGF19 or CCND1 amplification and TP53 and CDKN2A alterations occur at more advanced stages in aggressive tumors.9 Studies also showed the activation of the Wnt/β-catenin signaling pathway in approximately 50% of patients, caused by mutations in CTNNB1, AXIN1 or APC.9,10 Other frequent genetic alterations can be found in genes controlling the cell cycle, such as TP53, RB1, CCNA2, CCNE1, PTEN, ARID1A, ARID2, RPS6KA3 or NFE2L2. As reported by Schulze et al. (2015), 28% of patients harbored at least one damaging alteration potentially targetable by an FDA-approved drug.9
Patients with HCC are typically diagnosed in an advanced stage, with a median survival of about 6−20 months and a 5-year survival rate of less than 20%.11 Survival, however, varies by stage at diagnosis and treatment; patients with few comorbidities, preserved liver function and small, isolated HCCs have the most favorable survival rate.12
Over the last decades, various therapeutic agents for the treatment of advanced HCC have been extensively investigated in randomized clinical trials. In 2007, sorafenib was the first targeted agent approved for patients with advanced HCC or those progressing on locoregional therapies,13 marking the start of the subsequent evolution of the HCC treatment landscape. More recently, many new therapeutics demonstrated encouraging clinical results in the first- and second-line setting and were subsequently integrated into the ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up (Figure 1).14 Here we present an overview of currently available systemic therapies for the treatment of advanced HCC, including the evidence-based data obtained in clinical trials. In addition, emerging novel combinations are briefly discussed, with a glimpse of (neo)adjuvant treatment options for advanced HCC.

Current systemic therapy for advanced HCC
Prior to the introduction of sorafenib, the prognosis of patients with advanced HCC was dismal. Cytotoxic chemotherapy provided no clinically relevant improvements in survival outcomes in this patient population. In a randomized, phase III study, cisplatin/interferon alpha-2b/doxorubicin/fluorouracil (PIAF) versus doxorubicin did not demonstrate significantly improved overall survival (OS) (median, 8.67 months and 6.83 months; HR: 0.97 [95% CI: 0.71−1.32]; p=0.83) and overall response rates (ORR) (20.9% vs 10.5%) in patients with unresectable HCC.15 PIAF was also associated with increased treatment-related toxicity, with neutropenia, thrombocytopenia and hypokalemia being statistically more common in the PIAF than the doxorubicin group. Similar results were obtained from the phase III trial comparing nolatrexed and doxorubicin,16 as well as an open-label study of oxaliplatin plus fluorouracil/leucovorin versus doxorubicin.17 In addition, the phase III CALGB 80802 trial showed that the addition of doxorubicin to sorafenib in advanced HCC patients previously not treated with systemic therapy did not lead to improvement in OS (9.3 months with sorafenib plus doxorubicin vs 9.4 months with sorafenib alone; HR: 1.05 [95% CI: 0.83−1.31]) and progression-free survival (PFS) (4.0 months vs 3.7 months; HR: 0.93 [95% CI: 0.75−1.16]).18 Based on these results, chemotherapy is not recommended as a standard of care for advanced HCC.14
First- and second-line targeted therapy
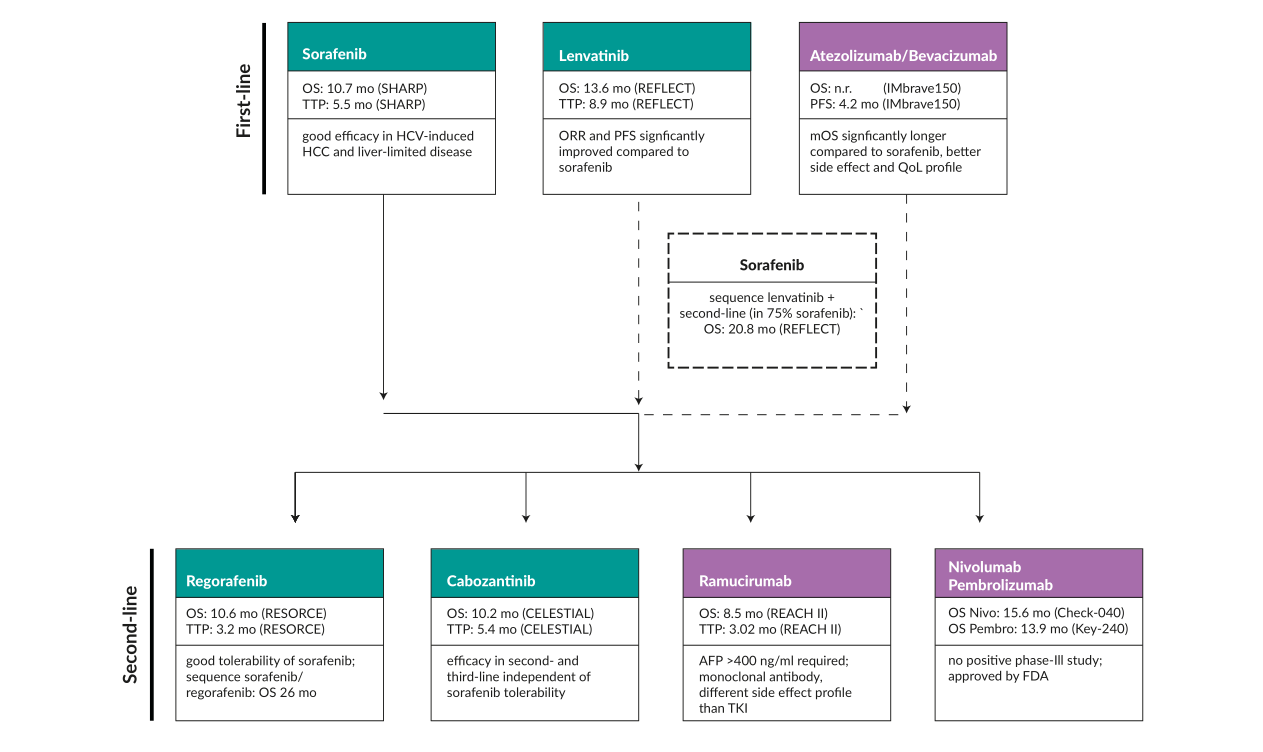
For a decade, sorafenib, a protein kinase inhibitor with activity against many protein kinases, including vascular endothelial growth factor receptors (VEGFR), platelet-derived growth factor receptors (PDGFR) and RAF kinases, has been the mainstay of treatment for patients with previously untreated unresectable HCC (Figure 2). The efficacy and safety of this agent were demonstrated in the phase III SHARP trial, which reported significantly improved median OS with sorafenib versus placebo (10.7 months vs 7.9 months with placebo; (HR: 0.69 [95% CI: 0.55 to 0.87]; p<0.001), with significantly improved time to radiologic progression (median, 5.5 months vs 2.8 months; p<0.001).19 Despite the clear survival advantage, the response rate to sorafenib was extremely low at only 2%. Improvement in OS with sorafenib was also reported in the SHARP-AP trial on the Asia-Pacific population (median, 6.5 months vs 4.2 months with placebo; HR: 0.68 [95% CI: 0.50−0.93]; p=0.014), with a median time to progression of 2.8 months and 1.4 months, respectively (HR: 0.57 [95% CI: 0.42−0.79]; p=0.0005).20 In both studies, diarrhea, weight loss and hand-foot skin reaction were among the most common adverse events.19,20
_.png)
In the past few years, we have witnessed the emergence of other promising therapies for the treatment of advanced HCC. The introduction of another multikinase inhibitor, lenvatinib, to the treatment landscape of HCC was based on the randomized, phase III, non-inferiority REFLECT trial, which compared lenvatinib with sorafenib in 954 previously untreated patients with unresectable HCC.22 At data cutoff, lenvatinib was non-inferior to sorafenib in terms of OS (median, 13.6 months vs 12.3 months; HR: 0.92 [95% CI: 0.79−1.06]). Of note, the response rate was 23% in the group of patients receiving lenvatinib. The most common any-grade adverse events for lenvatinib were hypertension, diarrhea and decreased appetite, with treatment-emergent adverse events of grade ≥3 occurring in 75.0% of patients receiving lenvatinib and 66.5% of patients receiving sorafenib. Both sorafenib23 and lenvatinib24 were approved by Swissmedic, but due to its better safety profile in a palliative setting, sorafenib remained more widely used.
There were also further attempts to boost the survival of previously untreated advanced HCC patients with targeted therapy, although no positive results were reported. For example, the phase III SEARCH trial demonstrated that adding erlotinib to sorafenib did not improve survival in patients with advanced HCC who were naïve to systemic treatment.25 More specifically, no difference between the sorafenib plus erlotinib group and the sorafenib plus placebo group was reported in regards to median OS (9.5 months vs 8.5 months; HR: 0.929; p=0.408) and median time to progression (3.2 months vs 4.0 months; HR: 1.135; p=0.18), with a significantly lower disease control rate with the combination treatment (43.9% vs 52.5%; p=0.021).
In HCC patients who progress on sorafenib, several therapies are currently available, including regorafenib, cabozantinib, ramucirumab and immune checkpoint inhibitors (ICIs) (Figure 2). The efficacy and safety of regorafenib, an oral multikinase inhibitor, were assessed in the randomized, double-blind, parallel-group, phase III RESORCE trial on HCC patients progressing during sorafenib treatment.26 Among 567 patients who initiated the treatment (regorafenib: n=374; placebo: n=193), regorafenib was associated with significantly improved OS (median, 10.6 months vs 7.8 months with placebo), corresponding to a 37%-reduced risk of death (HR: 0.63 [95% CI: 0.50−0.79]; one-sided p<0.0001). The most common clinically relevant grade 3 or 4 treatment-emergent adverse events with regorafenib were hypertension, hand-foot skin reaction and fatigue. An exploratory study further showed that regorafenib provided a clinical benefit regardless of the last sorafenib dose and regardless of the time to progression on prior sorafenib.27 The updated analysis demonstrated consistent OS outcomes (median, 10.7 with regorafenib vs 7.9 months with placebo; HR: 0.61 [95% CI: 0.50−0.75]; p<0.0001), with 1-year OS rates of 45% and 29%, respectively. Of note, when OS was assessed from the time of the start of prior sorafenib, the median time to death in RESORCE was 26.0 months among regorafenib-treated and 19.2 months among placebo-treated patients.
The randomized, double-blind, phase III CELESTIAL trial investigated cabozantinib, another multikinase inhibitor, active on targets including VEGFR 1, 2 and 3, MET and AXL implicated in HCC progression and the development of resistance to sorafenib.28 In this study, 707 patients who had previously received sorafenib and had disease progression after at least one systemic treatment for HCC, underwent 2:1 randomization to receive either cabozantinib or placebo. In the second planned interim analysis, the study showed significantly longer median OS with cabozantinib than placebo (10.2 months vs 8.0 months; HR: 0.76 [95% CI: 0.63−0.92]; p=0.005), with a median PFS of 5.2 months and 1.9 months, respectively (HR: 0.44 [95% CI: 0.36−0.52]; p<0.001). Grade 3−4 adverse events occurred in 68% of cabozantinib-treated and 36% placebo-treated patients. The most common high-grade side effects were hand-foot syndrome, hypertension and increased aspartate aminotransferase level.
Ramucirumab, an IgG1 monoclonal antibody targeting VEGFR2, was investigated in advanced HCC patients with increased α-fetoprotein concentrations who had received previous treatment with sorafenib, in the randomized, double-blind, placebo-controlled, phase III REACH-2 trial.29 At a median follow-up of 7.6 months, ramucirumab versus placebo significantly improved both median OS (8.5 months vs 7.3 months; HR: 0.710 [95% CI: 0.531−0.949]; p=0.0199) and PFS (2.8 months vs 1.6 months; HR: 0.452 [95% CI: 0.339−0.603]; p<0.0001). The most common grade ≥3 treatment-emergent adverse events with ramucirumab were hypertension, hyponatremia and increased aspartate aminotransferase. Serious adverse events of any grade occurred in 35% of patients in the ramucirumab group and 29% of patients in the placebo group.
Although REACH-2 was the first positive phase III trial conducted in a biomarker-selected patient population with HCC,29 the clinical utility of different biomarkers in HCC has not yet been established (except for α-fetoprotein), mainly due to their low sensitivity.30 In the clinical setting, several potential biomarkers are currently being evaluated, such as RAS mutations, FGF19/FGFR4 pathway alterations and MET amplification. Very recently, an analysis of two phase II studies showed that refametinib, a selective MEK inhibitor, in combination with sorafenib achieved a median OS of 12.7 months in patients with RAS-mutant unresectable or metastatic HCC, suggesting a synergistic effect between sorafenib and refametinib.31 Furthermore, the MET inhibitor capmatinib demonstrated antitumor activity in a subset of patients with MET-dysregulated HCC in a phase II, open-label, single-arm study, with a manageable safety profile.32 There is also an absence of suitable biomarkers to guide the clinical development of ICIs in HCC.
Based on these positive results, regorafenib,33 cabozantinib34 and ramucirumab35 have been approved by Swissmedic as second-line treatment. Of note, regorafenib has been specifically tested in patients who tolerate sorafenib, and ramucirumab in patients with α-fetoprotein concentrations of 400 ng/mL or greater.
Combining VEGF inhibitors with immune checkpoint inhibitors
Over the past years, different combinations with immunotherapies have been investigated, including angiogenesis inhibitors plus ICIs and dual ICIs, with promising results in clinical trials. The rationale to combine anti-vascular endothelial growth factor (VEGF) and ICI therapies has been based on the fact that anti-VEGF agents could reduce immunosuppression by decreasing the infiltration of immunosuppressive cells such as myeloid-derived suppressor cells (MDSC) and regulatory T cells (Tregs) in the tumor environment and increasing the infiltration of CD8+ T and dendritic cells, thus inducing increased and more durable responses to ICIs.3,36
This led to the initiation of a phase Ib study of atezolizumab, a monoclonal antibody that targets programmed death-ligand 1 (PD-L1), plus bevacizumab, an anti-VEGF antibody, which showed an acceptable safety profile and promising antitumor activity, with an ORR of 36% and a median PFS of 7 months in patients with untreated unresectable HCC.37 This combination was further assessed in the global, open-label, phase III IMbrave 150 trial, which established atezolizumab plus bevacizumab as the current standard of care for the first-line treatment of unresectable or metastatic HCC (Figure 1).14,36 In this study, patients were randomized 2:1 to receive either atezolizumab plus bevacizumab (n=336) or sorafenib (n=165) until unacceptable toxicity or disease progression.36 The primary analysis showed that the trial met both of its primary endpoints, with a median OS not reached with the combination therapy and 13.2 months with sorafenib (HR: 0.58 [95% CI: 0.42−0.79]; p<0.001) and a median PFS of 6.8 months and 4.3 months, respectively (HR: 0.59 [95% CI: 0.47−0.76]; p<0.001). No difference in the rate of grade 3 or 4 adverse events was reported (56.5% with atezolizumab plus bevacizumab; 55.1% with sorafenib). In the recent updated analysis, atezolizumab plus bevacizumab continued to demonstrate a clinically relevant improvement in survival outcomes.38 After an additional follow-up of 12 months, the median OS was 19.2 months with atezolizumab-containing regimen versus 13.4 months with sorafenib (HR: 0.66 [95% CI: 0.52−0.85]; p=0.0009) and the median PFS was 6.9 months versus 4.3 months, respectively (HR: 0.65 [95% CI: 0.5−0.81]; p=0.0001).
According to RECIST 1.1, the confirmed ORR was 30% in the atezolizumab plus bevacizumab arm and 11% in the sorafenib arm, including a complete response (CR) rate of 8% and <1%, respectively; the median duration of response (DOR) was 18.1 months and 14.9 months, respectively. This combination has been approved by Swissmedic39 as the first-line option, owing to evidence of efficacy.
Lenvatinib is another multikinase inhibitor that was investigated in combination with an ICI in the advanced HCC setting. Besides its ability to target VEGFR 1−3, lenvatinib also inhibits fibroblast growth factor receptors (FGFR) 1–4, RET and PDGFR.40 Data showed that the immunomodulatory effect of lenvatinib on tumor microenvironments may contribute to antitumor activity when combined with programmed cell death protein 1 (PD-1) inhibitors in patients with HCC.41 In an open-label, multicenter, phase Ib trial, frontline lenvatinib plus pembrolizumab, an anti-PD-1 monoclonal antibody, induced a confirmed ORR of 46.0% by modified RECIST, with a median DOR of 8.6 months.42 After a median follow-up of 10.6 months, the median PFS was 9.3 months and the median OS was 22 months. Grade ≥3 treatment-related adverse events occurred in 67% of patients, with no new safety signals identified.
Single-agent and combination immunotherapies for advanced HCC
Despite several available therapies for HCC, the prognosis remains poor, particularly for patients with advanced HCC. In recent years, studies have focused on immunotherapy for HCC, showing its potential therapeutic effects for advanced HCC.
Following the positive signals from the phase II KEYNOTE-224 trial,43 the randomized, double-blind, phase III KEYNOTE-240 further assessed pembrolizumab plus best supportive care (BSC) versus placebo plus BSC as second-line therapy in patients with advanced HCC previously treated with sorafenib.44 Although the OS (median, 13.9 months vs 10.6 months; HR: 0.781 [95% CI: 0.611−0.998]; p=0.0238) and PFS (3.0 months vs 2.8 months; HR: 0.718 [95% CI: 0.570−0.904]; p=0.0022) did not reach statistical significance per specified criteria, the results supported a favorable risk-to-benefit profile of pembrolizumab in this patient population. Consistent data were obtained in the recent updated analysis of KEYNOTE-240 with an additional 18 months of follow-up.45
Nivolumab is another anti-PD-1 antibody that has shown encouraging clinical efficacy and safety in patients with advanced HCC who were previously treated with sorafenib. In CheckMate 040, an open-label, non-comparative, phase I/II dose escalation and expansion trial, nivolumab achieved durable objective responses with a manageable safety profile in this group of patients.46 CheckMate 040 also investigated nivolumab in combination with ipilimumab, an anti-cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) antibody, in 148 sorafenib-pretreated patients with advanced HCC.47 At a median follow-up of 30.7 months, investigator-assessed ORR was 32% among patients who received nivolumab 1 mg/kg plus ipilimumab 3 mg/kg (every 3 weeks; a total of 4 doses), followed by nivolumab (240 mg every 2 weeks) (arm A), 27% among those who received nivolumab 3 mg/kg plus ipilimumab 1 mg/kg every 3 weeks (4 doses), followed by nivolumab (240 mg every 2 weeks) (arm B) and 29% among those who received nivolumab 3 mg/kg every 2 weeks plus ipilimumab 1 mg/kg every 6 weeks (arm C), with a median DOR of not reached, 15.2 months and 21.7 months, respectively. Based on the results from this study, the FDA granted accelerated approval for the arm A regimen in 2020.48 Very recently, long-term data confirmed the clinically meaningful responses and durable survival benefit of second-line nivolumab plus ipilimumab in advanced HCC.49 At a minimum follow-up of 44 months, the median OS remained at 22.2 months in arm A, 12.5 months in arm B and 12.7 months in arm C, with 36-month OS rates of 42%, 26% and 30%, respectively.
Nivolumab was also tested as a frontline therapy for the treatment of patients with advanced HCC. In the phase III CheckMate 459 trial, 743 patients were randomized to receive either nivolumab (n=371) or sorafenib (n=372), with a minimum follow-up of 22.8 months.50 Although the OS benefit did not meet the predefined threshold of statistical significance, there was a trend towards improvement in OS outcomes with nivolumab versus sorafenib (median, 16.4 months vs 14.7 months; HR: 0.85 [95% CI: 0.72−1.02]; p=0.0752). This OS benefit was observed across key subgroups, including hepatitis infection status and the presence of vascular invasion and/or extrahepatic spread.
Another promising approach for the treatment of advanced HCC has been combining tremelimumab, an anti-CTLA-4 antibody, with durvalumab, an anti-PD-1 antibody. This combination was investigated in a phase Ib/II study in patients with advanced HCC who progressed on or were not eligible for treatment with sorafenib.51 The study hypothesized that a combination of a single, priming dose of tremelimumab and durvalumab every 4 weeks may provide the benefit of tremelimumab combination therapy while minimizing associated toxicity. Overall, 332 patients were randomized to receive either tremelimumab (300 mg) plus durvalumab (1,500 mg) every 4 weeks, followed by durvalumab (1,500 mg once every 4 weeks) (n=75), durvalumab monotherapy (1,500 mg once every 4 weeks) (n=104), tremelimumab monotherapy (750 mg once every 4 weeks for 7 cycles and then once every 12 weeks) (n=69) or tremelimumab (75 mg once every 4 weeks) plus durvalumab (1,500 mg once every 4 weeks) (4 doses in total) followed by durvalumab 1,500 mg once every 4 weeks (n=84). The combination of tremelimumab 300 mg plus durvalumab achieved favorable efficacy across the four treatment arms (confirmed ORR, 24.0%, 10.6%, 7.2% and 9.5%, respectively) and an acceptable safety profile, with rates of grade ≥3 treatment-related adverse events of 37.8%, 20.8%, 43.5%, and 24.4%, respectively. The median OS was 18.7 months with tremelimumab 300 mg plus durvalumab, 13.6 months with durvalumab alone, 15.1 months with tremelimumab alone and 11.3 months with tremelimumab 75 mg plus durvalumab. Data also indicated that the clinical response was induced by the expansion of a population of CD8+Ki67+ lymphocytes which occurred early during treatment (day 15). Tremelimumab 300 mg plus durvalumab was associated with the highest level of CD8+ T-cell production, which was consistent with improved clinical response and efficacy with this regimen.
Based on these results, the phase III HIMALAYA trial aimed to further assess durvalumab 1,500 mg alone or in combination with tremelimumab 300 mg every 4 weeks versus sorafenib.52 The study enrolled a total of 1,324 patients with unresectable, advanced HCC who had not been treated with prior systemic therapy and were not eligible for locoregional therapy. Data showed that a single, high priming dose of tremelimumab added to durvalumab resulted in a statistically significant and clinically meaningful OS benefit versus sorafenib in this patient population. In addition, durvalumab as monotherapy was non-inferior to sorafenib in terms of OS, with a numerical trend in favor of durvalumab. Durvalumab also had an improved tolerability profile versus sorafenib.
Currently, there are several ongoing phase III randomized clinical trials investigating single-agent or combination immunotherapies for the first- and second-line treatment of HCC (Table 1). Regarding the second-line treatment for patients progressing on the standard of care atezolizumab plus bevacizumab, different immunotherapy plus tyrosine kinase inhibitor combinations have been explored, including atezolizumab plus lenvatinib/sorafenib, camrelizumab plus rivoceranib and regorafenib plus pembrolizumab (Table 1). As the optimal therapy sequence after disease progression on atezolizumab plus bevacizumab is not fully clear, a recent retrospective study investigated clinical outcomes of advanced HCC patients who received subsequent systemic therapy after progression on atezolizumab plus bevacizumab.53 Data showed comparable efficacy and manageable toxicities of the two multikinase inhibitors sorafenib and lenvatinib in this patient setting.
Neoadjuvant and adjuvant treatment options
These combination strategies are not only reshaping the treatment landscape for advanced HCC but are also being integrated into (neo)adjuvant settings, although there is currently no recommended systemic therapy for neoadjuvant or adjuvant treatment of HCC. The rationale is that, since most HCC are unresectable at diagnosis, and more active combinations are now available, with response rates up to 30%, improved outcomes in this patient population might be achieved by neoadjuvant therapy, which has the potential to reduce tumor volume. In this context, cabozantinib and nivolumab have been recently investigated as neoadjuvant therapy in patients with borderline resectable or locally advanced HCC.54,55 In this single-arm, phase I study, patients received cabozantinib 40 mg daily for 8 weeks plus nivolumab 240 mg every 2 weeks, followed by restaging and possible surgical resection. The trial met its primary endpoint, as no patients experienced a treatment-related adverse event that precluded timely surgical assessment. Of 15 patients enrolled, 12 (80%) underwent successful margin-negative resection and 5 of 12 (42%) resected patients had a major or complete pathological response. At a median follow-up of 12 months, 4 of 5 pathologic responders were without recurrence. In-depth profiling of the surgical resection biospecimens showed enrichment in effector T cells, as well as tertiary lymphoid aggregates, and a distinct spatial arrangement of B cells in responders versus nonresponders, indicating an organized B-cell contribution to antitumor activity.
Several ongoing randomized clinical trials are currently assessing postoperative adjuvant therapy with immune checkpoint inhibitors versus placebo, including nivolumab (CheckMate 9DX),56 pembrolizumab (KEYNOTE-937),57 atezolizumab plus bevacizumab (IMbrave050)58 and durvalumab alone or in combination with bevacizumab (EMERALD 2).59 At the ASCO 2021 annual meeting, the results were already presented from the single-arm phase II NIVOLVE study of nivolumab as adjuvant therapy for HCC patients after surgical resection or radiofrequency ablation, demonstrating a 1-year recurrence-free survival (RFS) rate of 76.7% with a median RFS of 26.0 months.60 Furthermore, exploratory biomarker analysis in patients who underwent hepatectomy showed that copy number gains in WNT/β-catenin-related genes, WNT/β-catenin pathway activating mutations, the presence of Foxp3+ cells and a low CD8+ tumor-infiltrating lymphocyte count were significantly correlated with high recurrence risk.
Conclusions
-
In the past years, the therapeutic armamentarium of HCC has been expanding, with a significant improvement in survival outcomes of patients with advanced disease. All the approved drugs have been developed within phase III clinical trials with well-established selection criteria, such as the use of the Barcelona Clinic Liver Cancer (BCLC) staging system, Child-Pugh A liver function and Eastern Cooperation Oncology Group (ECOG) performance status (PS) of 0 or 1. The systemic treatment for patients with a Child-Pugh B liver function or an ECOG PS of 2, however, remains an unmet need.
-
In patients with advanced-stage HCC, sorafenib was the only available standard of care for a decade. Lenvatinib was proven to be non-inferior to sorafenib, but with a different toxicity profile: higher grade hypertension and proteinuria occurring with lenvatinib and increased hand-foot skin reaction occurring with sorafenib. Both drugs are associated with asthenia, anorexia, diarrhea and weight loss, with a greater incidence with lenvatinib.
-
The combination of atezolizumab and bevacizumab was the first regimen to improve OS compared with sorafenib.
-
Currently, regorafenib, cabozantinib and ramucirumab are approved for the treatment of advanced HCC after progression on sorafenib, according to guidelines. In contrast, after atezolizumab plus bevacizumab and after lenvatinib, there are no second-line treatment options that have been published so far, but several trials are currently ongoing. In the meantime, the general view is that all drugs can be recommended after failure of either an IO-based combination or lenvatinib.
-
In the future, due to the availability of more active regimens providing high response rates, systemic therapies will move to earlier treatment lines or earlier stages of HCC. For example, in the case of patients with large tumors that are not the perfect candidate for transarterial chemoembolization (TACE), a “neoadjuvant” systemic therapy could be started, aimed at a tumor downsizing. Phase III trials with newer immunotherapy agents (alone or in a combination) in the adjuvant setting after curative resection or ablation and in combination with locoregional therapies are also ongoing. Shifting these highly active agents into earlier lines of therapy and for patients with earlier disease stages holds the promise of curative treatment for more patients.
Conflict of interest
The author declares that the study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Author Contributions
All authors contributed to and approved the final manuscript.