Introduction
Esophageal (EC) and gastric (GC) cancers account for more than 1,200,000 deaths every year, and therefore these cancers are considered to be a global public health problem.1 Patient prognosis remains poor, although improvements have been exclusively observed with novel perioperative treatments for resectable EC, mainly due to the perioperative 5-fluorouracil (5-FU), leucovorin, oxaliplatin, docetaxel (FLOT) regimen in GC. Historically, the median overall survival (OS) for advanced EC and GC did not exceed 12 months irrespective of the applied regimen. Before 2020, in advanced stage EC and GC, the prognosis with the available systemic options was poor.2,3 Thus, the median overall survival (OS) for patients with inoperable human epidermal growth factor receptor 2 (HER2)-negative EC/GC was approximately 1 year using the systemic treatment regimens at that time.4 Thus, in this field, new treatment combinations and new strategies are urgently needed. Immune checkpoint inhibitor (ICI) monotherapies in first-line and second-line settings have had disappointing results, especially for adenocarcinoma.5,6 For HER2-positive patients, first-line treatment with trastuzumab plus platinum and 5-FU in advanced EC and GC has been defined, but the outlook for combinations in first-line and further-line treatments have remained poor.7–9
First-line ICI and chemotherapy combinations in advanced EC and GC
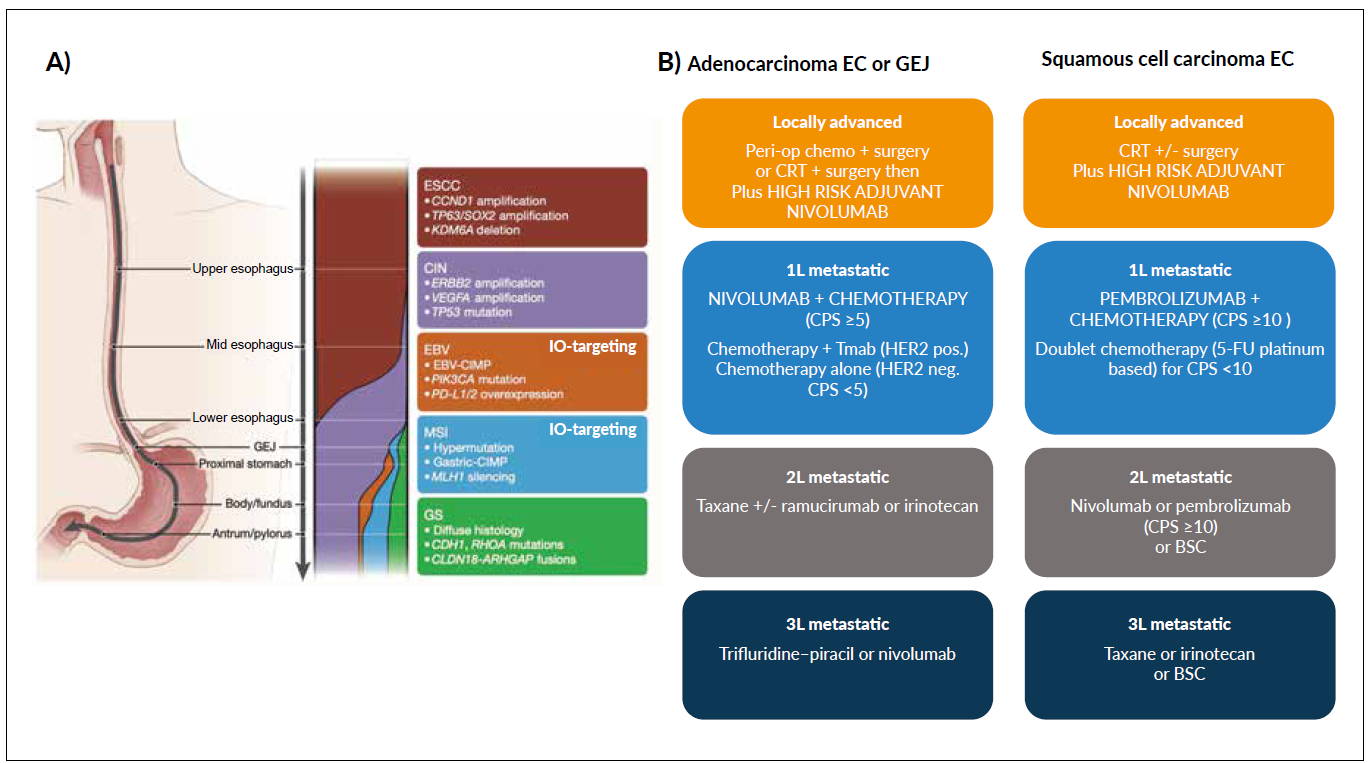
To date, the standard therapy for fit patients with advanced GC has included the first-line fluoropyrimidine–platinum doublet regimen, combined with trastuzumab in HER2-positive patients.7,10,11 The options for second-line treatment include ramucirumab,12 irinotecan,13 taxane,14 and ramucirumab monotherapy.15 Treatment plans for third-line and later line treatments can consider evidence-based options with trifluridine/tipiracil (TAS-102),16 as well as irinotecan and taxanes, if not previously used11 (Figure 1). In some Asian and American countries, immunotherapy with nivolumab17 or pembrolizumab18 would be a possible option in refractory EC or GC, whereas for the subgroup of microsatellite instability (MSI)-high or tumor mutational burden (TMB)-high tumors, pembrolizumab is available from the start, according to the FDA label.11,19–21 In general, fit patients with advanced esophageal adenocarcinoma (AEC) will be treated according to guidelines of advanced GC.22,23 The evidence for the optimal palliative treatment of advanced esophageal squamous cell carcinoma (ESCC) is missing. To date, doublet combinations for fit patients in first-line and single-agent therapies, or as best supportive care, are appropriate considerations for unfit patients.22,23 Recently, phase III studies have provided insights into the possible efficacy of ICIs with second-line nivolumab in ESCC,24 as well for pembrolizumab in programmed death-ligand 1 (PD-L1)-overexpressing ESCC or AEC.25
_gradations_of_molecular_subclasses_of_gastroesophageal_carcinoma._schematic_representin.png)
However, the big breakthrough of ICIs for EC and GC in 2020, was based on positive results from four randomized phase III trials (Table 1). These investigated chemo-immunotherapy in the first-line setting of EC/GC. In the global phase III CheckMate 649 study,28 patients with previously untreated advanced or metastatic HER2-negative gastric, gastroesophageal junction (GEJ), or esophageal adenocarcinoma were randomized into three arms (1:1:1): nivolumab plus chemotherapy (XelOx or FOLFOX), nivolumab plus ipilimumab, or chemotherapy alone. During ESMO 2020, the authors presented the first results of the co-primary endpoints of progression-free survival (PFS) and OS in the PD-L1 combined positive score (CPS) ≥5 group for the nivolumab plus chemotherapy versus chemotherapy arms. Overall, 1581 patients were randomized to the nivolumab plus chemotherapy and chemotherapy arms, and 60% had PD-L1 CPS ≥5. PFS and OS for the nivolumab plus chemotherapy arm were significantly improved compared with chemotherapy alone for patients with PD-L1 CPS ≥5 (median PFS: 7.7 months vs 6.0 months; HR: 0.68 [95% CI: 0.56–0.81]; p<0.0001; median OS: 14.4 months vs 11.1 months; HR: 0.71 [95% CI: 0.59–0.86], p<0.0001). OS was improved in patients with PD-L1 CPS ≥1, and for all randomized patients. The overall response rate (ORR) in PD-L1 CPS ≥5 was 60% for the nivolumab plus chemotherapy arm versus 45% for the chemotherapy arm (p<0.0001). The frequency of grade 3–4 treatment-related adverse events (TRAEs) was higher in the Nivolumab plus chemotherapy arm (59% vs 44%). During ESMO 2021,29 a 24-month update of CheckMate 649 revealed continued survival benefits for the addition of nivolumab to chemotherapy as a first-line treatment. The nivolumab-ipilimumab arm was the smallest of the three because the Data Monitoring Committee recommended an early stop due to higher mortality and toxicity rates in this arm than for the other two arms. Comparing 234 patients treated with nivolumab plus ipilimumab with 239 who received chemotherapy alone revealed no significant OS benefit for nivolumab-ipilimumab in the CPS ≥5 group or across all of the randomized patients. As a result, further analyses were not evaluated for significance. Although response rates were lower with nivolumab-ipilimumab, this combination therapy resulted in a longer duration of response (DOR). Once again in the CheckMate 649 study, patients with MSI-high tumors appeared to benefit more from the ICI combination of nivolumab plus ipilimumab therapy.
ATTRACTION-430 was a double-blind, placebo-controlled randomized phase III study conducted in Asian patients. This trial included patients with unresectable advanced or metastatic HER2-negative GC or GEJ adenocarcinoma who had no prior treatment for advanced disease. In total, 724 patients were randomized 1:1 to receive either nivolumab plus chemotherapy (S-1 plus oxaliplatin [SOX] or capecitabine plus oxaliplatin [CapeOX]), or placebo plus chemotherapy. The co-primary endpoints were PFS and OS, and the prespecified primary objective was to meet at least the PFS endpoint. Two-thirds of patients received second-line systemic treatment, and 27% of patients in the control arm received post-trial immunotherapy. In addition, 84% of patients had <1% PD-L1 expression on tumor cells. During ESMO 2020, the interim analysis after a median follow-up of 11.6 months showed improved PFS in the nivolumab plus chemotherapy arm (median PFS: 10.4 months vs 8.3 months; HR: 0.68 [95% CI 0.51–0.90]; p=0.0007). However, after a median follow-up of 26.6 months, the final analysis of OS showed no improvement in the combination compared with chemotherapy alone (median OS: 17.4 months vs 17.1 months; HR: 0.90 [95% CI 0.75–1.08]; p=0.257).34 Thus, analysis of the results of CheckMate 649 and ATTRACTION-4 indicated that both trials improved ORR and PFS with the addition of nivolumab to chemotherapy. However, the meaningful 3-month OS benefit in the CPS ≥5 patients in CheckMate 649 was not seen for the ATTRACTION-4 population. Possible explanations for the missing benefit in ATTRACTION-4 could be that the latter study was conducted only in Asian patients. In addition, these patients more often received second-line and third-line therapies compared to a Western population, along with the high-frequency use of immunotherapy in the second-line and third-line in Asia (i.e., post-trial use of immunotherapies). Another explanation for the lack of significance of the OS data might be the heterogeneity of the tumor patients. Thus subgroups achieving the greatest benefit need to be identified and carried out. Based on its positive efficacy endpoints and maintaining high QoL, nivolumab plus chemotherapy has become the new standard of care for first-line treatment of patients with CPS ≥5 esophagogastric adenocarcinoma.35 Although OS was improved in the CPS ≥1 subgroup, and in all patients in CheckMate 649, these groups were enriched with highly immunogenic CPS ≥5 tumors. There is thus the need to wait for further analysis of biomarker-selected subgroups to understand the value of the addition of nivolumab to chemotherapy for patients with CPS >1 to CPS <5.
The third study in this field is KEYNOTE-590,31 a global, double-blind, placebo-controlled, randomized, phase III trial of the first-line treatment of locally advanced unresectable or metastatic squamous cell carcinoma (SCC) or adenocarcinoma (AC) of the esophagus or GEJ Siewert type I. In total, 749 patients were randomized 1:1 to pembrolizumab plus chemotherapy (5-FU plus cisplatin) versus placebo plus chemotherapy. The co-primary endpoints of the trial were PFS and OS. The trial population comprised 50%, Asian patients and 73% of the total cohort presented with ESCC. About 50% of the tumors had PD-L1 CPS ≥10. After minimum follow-up of 13 months, OS was superior for pembrolizumab plus chemotherapy in all prespecified analyses: ESCC PD-L1 CPS ≥10 (13.9 months vs 8.8 months; HR: 0.57 [95% CI: 0.43–0.75]; p<0.0001); all ESCC (12.6 months vs 9.8 months; HR: 0.72 [95% CI: 0.60–0.88]; p=0.0006); all patients (SCC and GEJ) with PD-L1 CPS ≥10 (13.5 months vs 9.4 months; HR: 0.62 [95% CI: 0.49–0.78]; p<0.0001); all patients (12.4 months vs 9.8 months; HR: 0.73 [95% CI: 0.62–0.86]; p<0.0001). Prolonged PFS was also observed with pembrolizumab plus chemotherapy in all of the prespecified analyses (HR for all patients: 0.65 [95% CI: 0.55–0.76]; p<0.0001). The ORR for the immune-chemotherapy combination was significantly improved compared to chemotherapy alone (45% vs 29.3%). The number of grade 3 TRAEs was slightly higher (but not statistically significant) for this combination compared with chemotherapy alone (71.9% vs 67.6%), resulting in an effective and safe ICI and chemotherapeutic combination.
Although ESCC CPS ≥10 derived the most benefit in KEYNOTE-590, a meaningful OS benefit was detected in all of the ESCC patients. In March 2021, the FDA approved pembrolizumab with chemotherapy (5-FU with platinum-based) regardless of CPS for patients with ESCC, whereas the European Medicines Agency (EMA) approved pembrolizumab only for the ESCC CPS ≥10 population.
The fourth study was the three-arm, double-blind CheckMate 648 study.32 A total of 970 patients with metastatic and untreated ESCC underwent 1:1:1 randomization to receive nivolumab plus chemotherapy (5-FU plus cisplatin), or the combination of nivolumab (3 mg/kg, once every 2 weeks) plus ipilimumab (1 mg/kg, once every 6 weeks), or chemotherapy alone. The co-primary endpoints were PFS and OS in the tumor cell PD-L1 ≥1% population. Superiority for OS was seen for nivolumab plus chemotherapy compared to chemotherapy alone in the tumor cell PD-L1 ≥1% population (15.4 months vs 9.1 months; HR: 0.54 [95% CI: 0.37–0.80]; p<0.0001), and significant PFS benefit was seen for the tumor cell PD-L1 ≥1% population (6.9 months vs 4.4 months; HR: 0.65 [95% CI: 0.46–0.92]; p=0.0023). For the secondary endpoints (OS and PFS in all PD-L1 groups), a trend for OS benefit (without statistical significance) was seen for the nivolumab plus chemotherapy arm versus chemotherapy alone arm (13.2 months vs 10.7 months; HR: 0.74 [95% CI: 0.58–0.96]; p<0.0001). However, neither ipilimumab + nivolumab nor nivolumab plus chemotherapy showed any significant PFS versus the chemotherapy alone group. During ASCO 2021, the data for the combination arm of nivolumab plus ipilimumab compared with chemotherapy alone were presented. Although a statistical significance for OS was seen for the tumor cell PD-L1 ≥1% population (13.7 months vs 9.1 months; HR: 0.64 [95% CI: 0.46–0.90]; p<0.0010), there was no PFS benefit for the PD-L1 ≥1% population or for all randomized patients in the ipilimumab plus nivolumab arm. Moreover, the curves of the immuno-oncology (IO)-combination with the chemotherapy group crossed twice in the early phase, which challenges the interpretation of the data. Compared to chemotherapy alone group, similar toxicities were noted for the immunotherapy combination. The authors stated that there might be a chemotherapy-free option with ipilimumab and nivolumab. However, considering all of the nonsignificant PFS data, further biomarker analyses must be carried out to identify the right subgroup for an immune combination in the first line. At this time (September 2021), neither the FDA nor the EMA has made a decision regarding the approval of this combination.
New systemic concepts in perioperative, first-line as well in previously treated HER2-positive (immunohistochemistry [IHC] 3 positive or IHC2 positive 2/fluorescence in situ hybridization [FISH] positive) advanced EC and GC
During ASCO 2020, the results of the DESTINY-Gastric01 trial were presented and simultaneously published in the New England Journal of Medicine.33 The patient population included those pretreated (with ≥2 lines, including trastuzumab) as HER2-positive GC or GEJ adenocarcinoma. Within this phase II trial, 187 patients were randomized 2:1 to receive trastuzumab deruxtecan – an antibody-drug conjugate of an anti-HER2 antibody and a cytotoxic topoisomerase I inhibitor – or the physician’s choice of irinotecan or paclitaxel chemotherapy. The primary endpoint was ORR, and the key secondary endpoint was OS. ORR was significantly higher in the trastuzumab deruxtecan arm compared with the physician’s choice of chemotherapy (51% vs 14%; p<0.0001). Median OS was 12.5 months in the trastuzumab deruxtecan group and 8.4 months in the physician’s choice group (HR: 0.59 [95% CI: 0.39–0.88]; p<0.01). Grade 3 TRAEs with trastuzumab deruxtecan were more common compared with the control group (69.2% vs 53.2%), as well as treatment discontinuations (15.2% vs 6.5%) and interruptions (62.4% vs 37.1%). The most common grade 3 TRAEs were either hematological or gastrointestinal. Of note, 9.6% of patients in the experimental arm had trastuzumab deruxtecan-related interstitial lung disease/pneumonitis, which is a known risk with this drug. Even though the trial had limitations as it included limited ethnic diversity and a relatively small sample size, treatment with trastuzumab deruxtecan led to a significantly higher percentage of patients with an objective response and to a longer OS than conventional chemotherapy among patients with HER2-positive, advanced GC. Confirmation of the activity of trastuzumab deruxtecan in a preferably global phase III trial is necessary before this treatment can be considered as a new standard of care for previously treated patients with HER2-positive advanced GC.
Preliminary results for KEYNOTE-811 in previously untreated metastatic HER2-positive adenocarcinomas of GC and GEJ were presented at ASCO 2021.36 In this double-blind, phase III trial, 692 patients were randomized 1:1 to either pembrolizumab plus trastuzumab plus chemotherapy (5-FU plus cisplatin or capecitabine plus oxaliplatin) or to the control arm of trastuzumab plus chemotherapy. The dual primary endpoints are PFS and OS, with secondary endpoints of ORR, safety, and DOR. At this early stage analysis, the data for 264 patients were presented. A high ORR of 74.4% was seen for the study arm, compared with 51.9% in the control arm (p=0.0006), which translated into a 22.9% ORR difference in favor of the combination of pembrolizumab plus trastuzumab plus chemotherapy. The best responses presented were complete remission (CR) for 11% and partial remission (PR) for 64% in the study arm, compared with 4% and 69%, respectively, in the standard arm. We must await the complete data, including the survival assessment before an evaluation for HER-2 treatment of advanced GC takes place. At this stage, this promising trial highlights the synergistic benefit of programmed cell death protein 1 (PD-1) blockade with anti-HER2 treatment in addition to chemotherapy in HER2-positive GC or GEJ. Thus, in May 2021, the FDA granted accelerated approval for the combination of pembrolizumab plus trastuzumab plus chemotherapy in HER2-positive metastatic GC and GEJ cancers.37
Does immunotherapy move into an adjuvant and perioperative setting for EC and GC?
For clinical stage beyond T1N0 and resectable gastric adenocarcinoma, the standard of care includes combined modality treatments. The timing and choice of treatment modalities differ according to geographic region. In Europe, perioperative FLOT38 is the preferred treatment option, whereas surgery followed by adjuvant chemoradiotherapy is mostly used in the USA, and surgery followed by adjuvant chemotherapy is the common practice in Asia.10,39 Targeting the tumor in this perioperative and adjuvant setting is currently the aim of several clinical trials. The results of the randomized phase III trial CheckMate 577 were presented at ESMO Congress 2020.40,41 This study included 794 patients with stage II-III esophageal or GEJ squamous cell or adenocarcinoma with residual pathologic disease (≥ypT1 or ≥ ypN1) after neoadjuvant chemoradiation and R0 surgical resection. Patients underwent 2:1 randomization to adjuvant nivolumab or placebo for up to 1 year. Most patients had <1% PD-L1 expression on tumor cells. The primary endpoint was disease-free survival (DFS), and after median follow-up of 24.4 months, median DFS was significantly improved, with 22.4 months in the nivolumab arm compared to 11.0 months in the placebo arm (HR: 0.69 [95% CI: 0.56–0.86]; p=0.0003). In general, nivolumab was well tolerated and mostly caused grade 1–2 TRAEs. According to patient-reported outcome analyses, nivolumab treatment was not associated with deterioration of their overall health status compared to placebo. The CheckMate 577 trial addressed the important issue of how to improve outcomes in the poor-risk group of patients with residual pathologic disease after neoadjuvant chemoradiation. Thus, adjuvant nivolumab treatment should be the new standard of care for these patients and has already been approved by the FDA,42 EMA,43 and Swissmedic.44 However, for patients with esophageal or GEJ adenocarcinoma, this study does not answer the question of whether neoadjuvant chemoradiation (with the potential addition of adjuvant nivolumab) is a better treatment strategy than perioperative chemotherapy. Other studies in this field for definitive radiochemotherapy followed by additive pembrolizumab are awaited (e.g., KEYNOTE 975; NCT04210115), as well a focus on additional use of ICIs during and after perioperative treatment for GC and GEJ, which will be investigated in the KEYNOTE 585 trial (NCT04882241) as well as the AIO/SAKK phase II DANTE trial (NCT03421288).
Conclusions
A new era in esophageal-gastric cancer has arrived with ICIs added to chemotherapy in the first-line setting of metastatic and advanced tumors. Even in the adjuvant setting, ICIs can improve the status of patients with this disease. Targeting combinations with immune therapies in the field of HER2-positive adenocarcinomas is promising. Nevertheless, better identification and classification of predefined biomarkers are needed for selective responses to such immuno-chemotherapy combinations. Finally, this will provide a better understanding of responses as well as the mechanism of resistance.
Conflicts of interest
They are as follows.
Scientific consultancy roles
AdvancedAcceleratorApp, Amgen, Bayer, BMS, Eisai, Lilly, MSD, Novartis, Pfizer, Servier, Sanofi
Research grants
Ipsen
Principal investigator (ISS)
Ipsen
Author Contributions
All authors contributed to and approved the final manuscript.