
Introduction
Cancer is the second leading cause of death in Switzerland.1 The incidence of cancer increases dramatically with advancing age,2 with a median age of onset around 65 years.3 By 2030, it is estimated that 70% of all new cancer cases will be diagnosed in patients 65 years and older.2 Unsurprisingly, cancer patients above 65 years have a 16-fold greater mortality risk than younger patients, with 70% of cancer-related deaths occurring in this age group.2,4,5 Early diagnosis and improved treatment options have led to a steady increase in the number of older adult cancer survivors in Switzerland.1,6
Physiological changes that mostly occur with aging (e.g., decreased cardiovascular, respiratory and renal function) impair the tolerance of older patients to cancer therapy.7,8 Frailty, defined as an increased vulnerability to stressors due to a multisystem reduction in reserve capacity, is considered a distinct concept linked to higher chronological age and comorbidities.9 Meanwhile, the aging process is highly heterogeneous and influenced by multiple genetic, epigenetic and environmental factors, differing at all levels from the molecular to the system level.10 Therefore, frailty alone is not sufficient as a conceptual marker for cancer management but rather biological age.11 As long as the concepts of longevity medicine are maturing and artificial intelligence (AI)-based precision oncology is at the inceptive state of entering the clinical routine, the concept of frailty versus fitness, the so-called “Frailty syndrome”, is gaining traction.9,12,13 Identifying frail cancer patients, i.e., those with high susceptibility, low functional reserve and unstable homeostasis, leads to a better estimation of individual response to therapies than looking at chronological age alone,9,13 therefore, careful consideration of each patient’s status, including frailty in the treatment decision-making process is an integral part of oncological management. However, measuring and quantifying frailty in the real-world setting remains a challenge.12
In addition to personal biological status, the optimal treatment in older cancer patients is challenged by the importance of maintaining quality of life (QoL). In routine clinical practice, the question often arises as to which treatment strategy is the right one for each patient, especially one that allows the patient to remain independent for as long as possible.14–16 Many older cancer patients are therefore at risk for both being undertreated and overtreated.14–17 Another challenge is that despite the increasing number of older people in the population and the relatively high frequency of cancer in this age group, patients 65 years of age or older are significantly underrepresented in trials of cancer treatments.18 There is limited information concerning the efficacy, tolerability, and toxicity of cancer therapies in senior adults, although the literature indicates that this trend is slowly changing.19
Clinical challenges and pitfalls in early palliative care of geriatric oncology patients
Palliative care is defined as an approach that improves the QoL of patients and their families facing the problem associated with life-threatening illness through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other physical, psychosocial and spiritual deficits.20 Evidence from the literature suggests that earlier integration of palliative care as part of a multidisciplinary team can facilitate optimum patient care.21 It should therefore be a part of the older cancer patient’s care journey throughout the trajectory of their disease, with varying levels of multidisciplinary involvement as the disease progresses. However, providing appropriate care for older cancer patients is confounded by many factors, including multiple comorbidities and polypharmacy, frailty, dementia and cognitive problems, delirium, and functional impairment.22 In addition, approximately half of cancer patients will have a formal psychiatric disorder such as depression or anxiety.23,24 Although psychiatric illnesses are common, they are often neglected, which leads to reduced QoL, lower adherence to treatment, poorer cancer survival and increased treatment costs.24 In the field of oncology, the use of palliative care has increased significantly over the past decade.21 A US-based observational study found that patients who received palliative care experienced significantly less aggressive care, lower rates of hospitalization, increased use of hospice, and fewer invasive procedures near the end of life than patients that did not.21 Furthermore, negative public views and misconceptions about palliative care still exist within the community; for example, palliative care is often falsely equalized with end-of-life care and hospice care and thus death.25 This may partly be due to the fact that many elderly cancer patients prefer supportive symptom management and refuse further aggressive treatments such as chemotherapy routinely given to younger patients.26 Another challenge is the lack of literature that specifically addresses geriatric palliative care across the domains of palliative care.27 Additional barriers to ensuring older cancer patients receive appropriate palliative care provision include the fact that some elderly patients lack capacity as a result of confusion and delirium, they may have limited social and family support, i.e., older patients tend to live further away from families and have fewer friends to support them, and have a lack of psychosocial support to combat loneliness and depression, especially since many older people tend to live alone.28
Age-related factors influencing treatment of elderly cancer patients
Treatment decisions for older cancer patients must be made alongside other medical conditions such as cognitive impairment, depression, polypharmacy secondary to multiple comorbidities.29 Over the years, a lack of clinical data has led to a paucity of appropriate treatment guidelines and absence of a standard approach in this population.19 Since older adults with cancer represent a diverse cohort of patients with other comorbidities that may have an equal impact on survival and QoL as the diagnosis of malignancy itself, a competing risk approach design for clinical trials has been proposed.30,31
Immune checkpoint inhibitors are a well-established treatment for all types of cancers and are generally better tolerated than cytotoxic chemotherapy.32 Treatment with anti-programmed cell death protein 1 (PD-1)/programmed death-ligand 1 (PD-L1) agents is, therefore, an attractive option for elderly patients with multiple comorbidities.33 Pooled data on elderly patients (aged 75 years and above) with PD-L1-positive advanced non-small-cell lung cancer (NSCLC) from three landmark cancer trials were recently analyzed.34 Results demonstrated that immunotherapy improved overall survival in these patients compared with chemotherapy, and results were comparable to the overall population results in the individual studies.34 Moreover, the older NCSLC patients treated with immunotherapy experienced fewer treatment-related adverse events (TRAEs) than those that received chemotherapy (grade 3−4 TRAEs: 24.2% versus 61.0%).34 Similarly, in a real-life study of the anti-PD-L1 inhibitor nivolumab, reported by Grossi et al. (2019), almost half of the NSCLC participants (N=1588) were elderly patients aged 70 or above (n=754). In a subgroup analysis, elderly patients receiving immunotherapy with nivolumab achieved outcomes similar to the overall study population, with an overall survival rate of 43% at 12 months.35
It is widely known that an aging immune system (immunosenescence) may affect outcomes for cancer patients.32,36 The main hallmarks of immunosenescence include a reduced ability to respond to new antigens, the accumulation of memory T cells and the lingering level of low-grade inflammation.37 For example, in patients receiving immunotherapy for melanoma, older adults may experience worse progression-free survival due to reduced levels of tumor-infiltrating lymphocytes.32,38,39 Understanding immune-regulatory functions is critical to implementing effective targeted immunomodulatory strategies for elderly patients.37
Furthermore, age-related genetic differences such as single nucleotide variants (SNVs) and copy number variants (CNVs) have also been observed in older cancer patients.40 In patients with squamous cell carcinoma of the lung, Meucci et al. (2018) showed that the defective DNA mismatch repair (MMR)-related signature 6 (SI6) was negatively correlated with patient age.40 Another step towards targeted, personalized medicine for older cancer patients would be to use gene expression profiling to improve prognostication and thus more appropriate treatment selection.41
How to fight diagnostic and therapeutic nihilism in elderly cancer patients
Geriatric screening and assessment
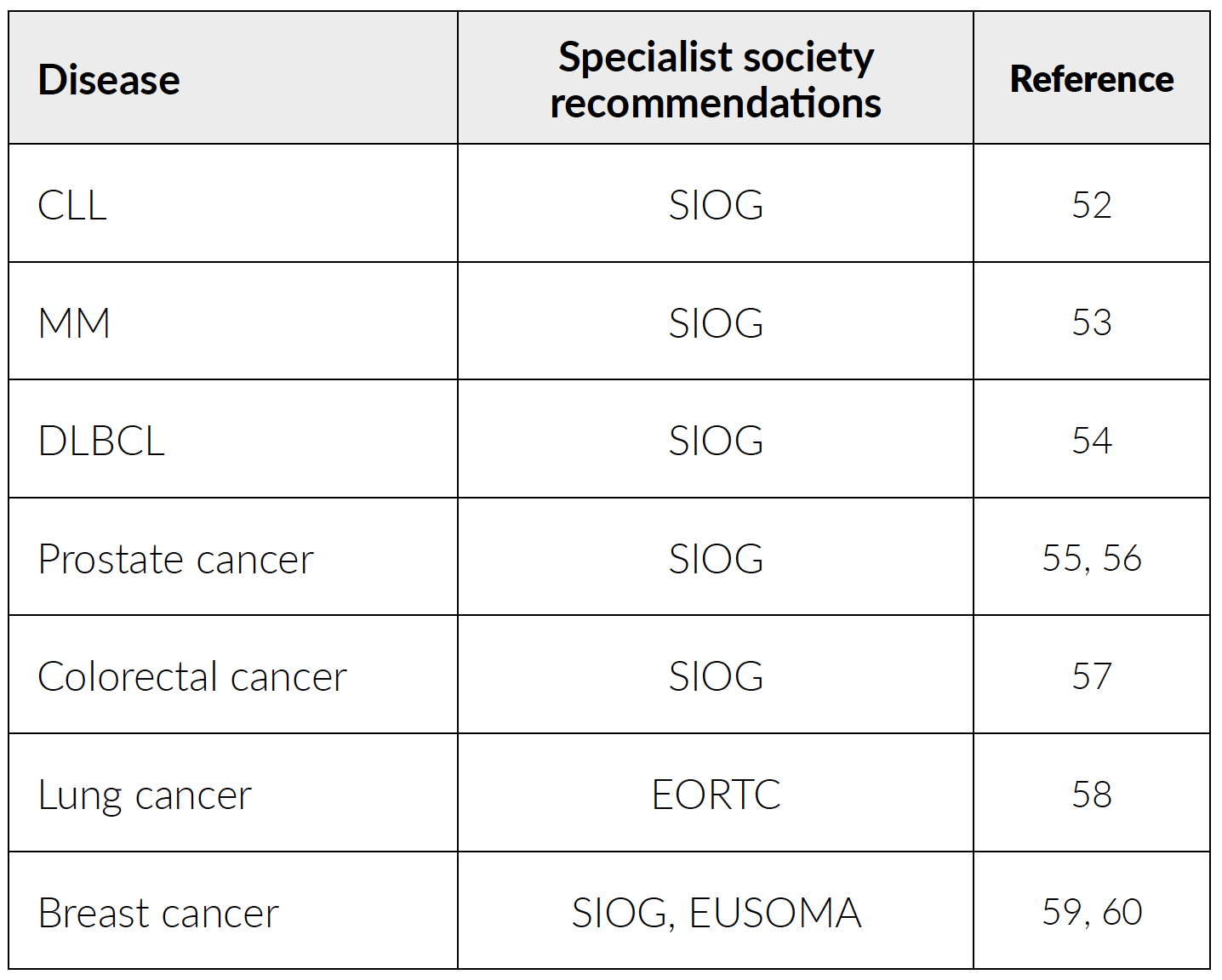
One of the most commonly applied assessment tools for frailty is the comprehensive geriatric assessment (CGA) which evaluates functional status, comorbid medical conditions, cognition, nutritional status, psychological state, social support and the patient’s medication.42 CGA is a systemic evaluation tool, which, if correctly implemented, can help identify and optimize age-related vulnerabilities, reduce over- and under-treatment, and guide treatment recommendations in older patients.43,44 International consensus guidelines on the management of older patients with various cancers recommend the use of CGAs, e.g., the International Society of Geriatric Oncology (SIOG),45 American Society of Clinical Oncology (ASCO),46 and the National Comprehensive Cancer Network (NCCN) guidelines (Table 1).47 Table 2 shows examples of scales that can be assessed as part of the CGA. The 9-point validated Clinical Frailty Scale (CFS) evolved from the Canadian Study of Health and Aging and is one of the broadest and most commonly used scales in Switzerland and worldwide.48 It summarizes the level of fitness or frailty of an older adult after evaluation by a healthcare professional from 1 (“very fit”) to 9 (“terminally ill”).48 However, CGAs such as the CFS are not consistently implemented, and more prospective studies are needed to confirm their impact in guiding treatment decisions in elderly patients with cancer.49,50
.png)
The major barrier to completing the CGA is the length of time required to complete the entire assessment (approx. two hours).61,62 In other settings, a lack of awareness or expertise may limit its application. In settings where CGA is not feasible or resources are limited, shorter geriatric assessment (GA) tools have been developed. Screening using the relatively quick and easy-to-apply GA tests can help identify vulnerable patients most likely to benefit from a full CGA assessment before starting treatment; therefore, GA screening tests can help preserve clinical time and personnel resources.63,64 Validated GA screening tools in the evaluation of physical fragility include the Geriatric 8 (G8) questionnaire,65 abbreviated Comprehensive Geriatric Assessment (aCGA),66 Triage Risk Screening Tool (TRST),67 and Vulnerable Elders Survey-13 (VES-13), many of which can be completed in less than six minutes.64,68,69 GA screening can also be targeted, e.g., to older cancer patients. Nowadays, cancer-specific GA screening tools have been developed, including the Cancer Aging Research Group (CARG)70,71 and the Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH),72,73 which estimate toxicity risk in older patients receiving chemotherapy. Healthcare professionals can use cancer-specific GAs to develop treatment plans and tailor management strategies to improve QoL for older patients with cancer.74 To meet the needs of underserved older adults with cancer in rural communities or to minimize infection risk in highly susceptible populations (e.g., from Covid-19), adaptation and delivery of a GA via telehealth is being evaluated as a potential GA tool.75 GAs are currently available for many different outcome measures such as frailty, nutritional status, comorbidity and cognition.76
Cancer patients with pre-existing cognitive impairment may be at great risk for cognitive decline with therapy and are potentially at increased risk for treatment-related adverse events.77 Cognitive assessment has not historically been routinely incorporated into the evaluation and management of older adults. Several short cognitive screening tools have now been evaluated in cancer patients specifically,77 including the Montreal Cognitive Assessment (MoCA),78 the Mini-Mental Status Exam (MMSE),79 the Mini-Cog80 tests. For example, the Mini-Cog is a short (<3 minutes) cognitive screening tool for dementia that combines a delayed recall item and a clock-drawing test.77
Cancer-specific GA can be used to guide interventions. Targeted interventions may improve treatment tolerance, adherence, physical function and QoL.81,82 The randomized GAIN trial evaluated whether geriatric assessment-driven intervention could reduce chemotherapy-related toxic effects among older cancer patients compared with standard-of-care. The trial included 613 cancer patients with a solid tumor who had started chemotherapy between 2015 and 2019. The median age of the study participants was 71 years (range 65−91). Results from GAIN revealed that implementation of multidisciplinary GA-driven interventions reduces grade 3−5 chemotoxicities in older adults with cancer. Moreover, the trial also showed that GA-driven interventions improved the completion of advance directives.83 Future research should focus on the validation of GA screening tools in older patients. GA-driven interventions aimed at optimizing treatment should also be applied for this patient population.76
Tackling underdiagnosis and undertreatment
Since aging is the single most important risk factor for the development of cancer, it is important to overcome ageism in this field.84 Professional subjective assessments might lead to older people receiving a reduced range of treatment options, e.g., elderly cancer patients are considered less likely to recover from aggressive therapies and interventions than younger patients.85 Lower risk and less aggressive treatments may be chosen based on the misconception that it will avoid patient morbidity and mortality;85 however, studies show that such undertreatment leads to a reduced five-year survival for older cancer patients.85,86 A recent study showed that 34% of geriatric patients are overtreated while 15% are undertreated.87 Overtreatment may involve administering standard-of-care to patients who may not gain any clinical benefit.88 In older patients, overtreatment can lead to more grade 3 and 4 toxicity than treatment appropriately adapted to fragility.87 In contrast, many studies show that elderly patients often do not receive standard therapy compared to their younger counterparts.89 Older patients are often considered “frail” and have multiple comorbidities and other characteristics that cause hesitance to prescribe standard regimens.29,90 Indeed, although recent studies show that most older patients can benefit from and tolerate intensive cancer therapies, similar to younger patients, there is still a reluctancy to aggressively treat elderly patients, even those without comorbidities.91 Undertreatment may partly be attributed to common misperceptions about life expectancy, therapeutic benefit and treatment risks.5,92 In a study of 397 geriatric patients, 43% received less intensive chemotherapy treatment than the standard-of-care.87 Assumptions about a patient’s ability to tolerate treatment, QoL, or personal preference should therefore not be based on chronological age.93 In recent years, the SIOG has begun to address the age-based disparities in research and treatment by advocating assessments of older patients with cancer.93 Other stakeholders, including the elderly and their caregivers, nurses, palliative healthcare professionals also have an important role to play if the treatment landscape for older cancer patients is to change.
Conclusions and future directions
With an aging population and improvement of life expectancy, managing older people with cancer is a growing burden in Switzerland and worldwide. As newer agents become available and new combinations tested, dedicated studies to identify age-related factors, i.e., immune profiling or predictive/prognostic biomarkers for elderly patients, are warranted.94 Developing local protocols and guidelines of care for older people with frailty is crucial. Multidisciplinary optimization of personalized treatment plans is required, involving oncology/geriatrics/palliative care/psycho-oncologist/internal medicine/supportive care specialists. Furthermore, establishing a patient registry in the field of geriatric oncology would enable a Switzerland-wide survey of cancer, screening and comparative, comprehensive omics testing, as well as complete tumor profiling, ultimately leading to better survival outcomes and QoL for older cancer patients.95
Conflict of interest
The author declares that the study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Author Contributions
All authors contributed to and approved the final manuscript.