
Introduction
FIRST-LINE THERAPY OPTIONS: A NEW STANDARD APPROACH
A few randomized phase II/III trials explored the role of immunotherapy for urothelial carcinoma (UC) in the first-line setting, either as monotherapy and/or in combination with chemotherapy.6–10 The open-label, phase III JAVELIN Bladder-100 study was conceived to prove the benefit of a maintenance therapy with a programmed death-ligand 1 (PD-L1) inhibitor after initial response to 4 to 6 cycles of platinum-based chemotherapy, demonstrating that maintenance with avelumab in addition to best supportive care (BSC) significantly prolonged overall survival (OS) versus BSC alone (median OS, 21.4 months vs 14.3 months; HR: 0.69 [95% Cl: 0.56−0.86]; p=0.001).7 A post hoc analysis of the trial recently assessed the efficacy of avelumab maintenance plus BSC versus BSC alone by the duration of treatment-free interval (TFI), defined as the time from completion of chemotherapy to start of first-line maintenance. Results showed that OS and PFS benefits were consistent across all TFI subgroups, including TFI: 4–<6 weeks, TFI: 6–<8 weeks, TFI: 8–10 weeks.11 The trial also provides quality of life data supporting the benefit of avelumab maintenance without deterioration of the overall health status.12
Results of IMvigor-130 and KEYNOTE-361 have failed to support the combinational use of first-line platinum-based chemotherapy and a programmed death-protein 1 (PD-1) or PD-L1 inhibitor as the frontline treatment for advanced or metastatic UC.8,9 Both trials compared atezolizumab and pembrolizumab in combination with platinum-based chemotherapy. In addition, the third arm in both trials enrolled patients to receive first-line immune checkpoint inhibitors (ICI) monotherapy compared to platinum-based chemotherapy alone, including a retrospective subgroup analysis on PD-L1 expression status. Progression-free survival (PFS) and OS were analyzed as pre-specified co-primary endpoints in both trials. Overall, the final analysis of the two trials showed a modest improvement in PFS in patients receiving combined chemotherapy and atezolizumab in IMvigor-130 (HR: 0.82 [95% CI: 0.70−0.96]; p=0.007) or pembrolizumab in KEYNOTE-361 (HR: 0.78 [95% CI: 0.65−0.93]; p=0.0033), as compared with chemotherapy alone. Results from both trials further indicated that the addition of ICI to platinum-based chemotherapy does not significantly improve OS in the first-line setting. Data from IMvigor-130, KEYNOTE-361 and DANUBE also demonstrated that although the duration of response (DoR) seen after first-line treatment with ICIs tends to be longer than with chemotherapy, only a small proportion of patients (i.e., those with high PD-1/PD-L1 expression status) experience this benefit.8–10 Notably, the initial response after a few months of treatment is superior with chemotherapy (CT) for most UC patients.
Secondary/exploratory endpoint data from IMvigor-13013 and KEYNOTE-36114 provide supportive evidence for the current EMA label for atezolizumab and pembrolizumab in platin-ineligible patients with high PD-L1 expression. In a subgroup of cisplatin-ineligible patients with high PD-L1 status (≥5%) receiving the first-line atezolizumab in IMvigor-130, the investigator-assessed overall response rate (ORR) was 38% in atezolizumab-treated patients versus 33% in platinum/gemcitabine-treated patients.13
EMERGING SECOND- AND SUBSEQUENT-LINE OPTIONS
Pembrolizumab is currently the only ICI that demonstrated a significant OS benefit as a second-line treatment in a phase III trial.15,16 After 3 years of treatment follow-up, the KEYNOTE-045 trial demonstrated an improvement in OS with pembrolizumab compared with chemotherapy in UC patients who progressed after platinum-based chemotherapy.15 Median OS with pembrolizumab was 10.1 versus 7.2 months with chemotherapy (HR: 0.72 [95% CI: 0.59–0.87]; p=0.0003). In the recently presented data at ASCO 2021, after 5 years of follow-up, pembrolizumab versus chemotherapy continued to improve the median OS (10.1 months vs 7.2 months) (Figure 1), as well as ORR (21.9% vs 11.0%) and the median DoR (29.7 months vs 4.4 months) in this patients population.17 In contrast, in the hierarchically tested and pre-specified PD-L1 positive/first endpoint populations, atezolizumab was not associated with significantly longer OS versus chemotherapy in patients with platinum-refractory metastatic UC in the phase III IMvigor211 trial.16 However, the safety profile for atezolizumab was favorable compared with chemotherapy in this patient setting.

Treatment after progression on platinum-based chemotherapy and ICI is challenging due to limited treatment options. New therapeutic agents are therefore warranted. Erdafitinib is a novel fibroblast growth factor receptor (FGFR) kinase inhibitor used to treat advanced UC patients with susceptible FGFR3 or FGFR2 genetic alterations. In an international open-label phase II trial, 99 patients with FGFR-altered UC were treated with an optimized dosing schedule of once-daily erdafitinib (8 mg).18 All study participants had progressed after or during ≥1 line of prior platinum-based CT; notably, prior treatment with a prior ICI was allowed. The primary endpoint of ORR was 40%, with 3% of patients achieving a complete response and 37% a partial response.19 Stable disease (SD) occurred in 39% of patients. These data show that erdafitinib provides unprecedented response rates, even in patients with visceral metastases. After a median follow-up of 24 months, the overall median PFS and OS for all patients were 5.52 months and 11.3 months, respectively.20 Although most patients progressed by 18 months, such an additional survival benefit is valuable in the third-line setting. While erdafitinib is a convenient oral medicine to administer with a promising clinical activity, this agent was associated with any-grade adverse events (AEs) such as hyperphosphatemia (72%) as well as skin, nail and ocular-related events (all up to 50%).18,19 Encouraging data in combination with a checkpoint inhibitor in cisplatin-unfit patients has recently been presented from a phase Ib study by Powles and colleagues at the 2021 ESMO meeting and warrants further investigation in future trials.21
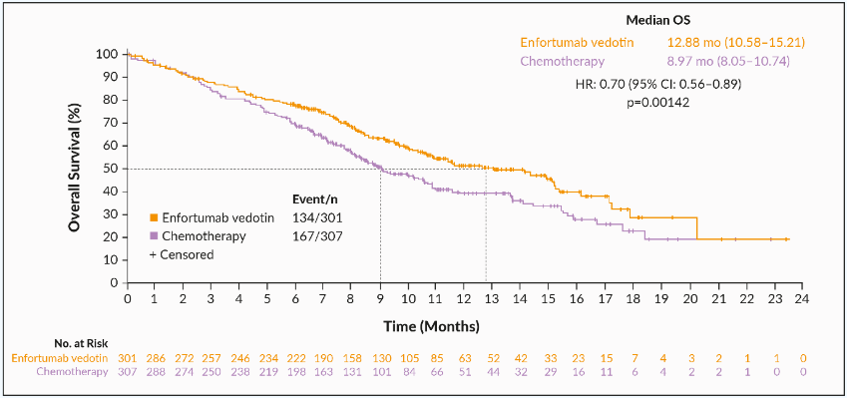
Enfortumab vedotin, an antibody-drug conjugate (ADC) comprised of a fully human monoclonal antibody and the microtubule-disrupting agent monomethyl auristatin E, is another emerging new UC treatment being investigated in clinical trials in the third-line setting. This agent targets nectin-4, which is highly expressed in UC. The open-label, phase II EV-301 trial evaluated enfortumab vedotin in patients who had progressed following PD-1/PD-L1 therapy and who had received a prior platinum-containing regimen.22 The primary endpoint was OS, which was improved following treatment with enfortumab vedotin versus chemotherapy (12.88 months vs 8.97 months; HR: 0.70 [95% CI: 0.56−0.89]; p=0.00142) (Figure 2). Notably, treatment can be held and restarted in case if AEs of special interest, such as neuropathy, skin reactions or hyperglycemia, are experienced. However, enfortumab vedotin is generally well-tolerated, with most treatment-relevant AEs of special interest reported as mild or moderate. In the single-arm 2-cohort, EV-201 study, enrolled platinum-naive, cisplatin-ineligible patients with prior anti-PD-1/L1 treatment with locally advanced or metastatic urothelial carcinoma. The first previously presented analysis results of EV-201 Cohort 2 showed an ORR of 52% with a CR rate of 20% and a median DoR of 10.9 months.23 The updated results with an additional 3 months follow-up were consistent with those of the primary analysis with an ORR of 51%, CR of 22% and a median DoR of 13.8 months.24 Based on the results of phase II EV-301 trial, the FDA recently granted regular approval to enfortumab vedotin for patients with locally advanced or metastatic UC, who have received a PD-1 or PD-L1 inhibitor and platinum-containing chemotherapy or are ineligible for cisplatin-containing chemotherapy and have previously received ≥1 prior lines of therapy in the neoadjuvant/adjuvant, locally advanced or metastatic setting.
_in_phase_iii_ev-301_trial.png)
CURRENT TREATMENT LANDSCAPE IN SWITZERLAND
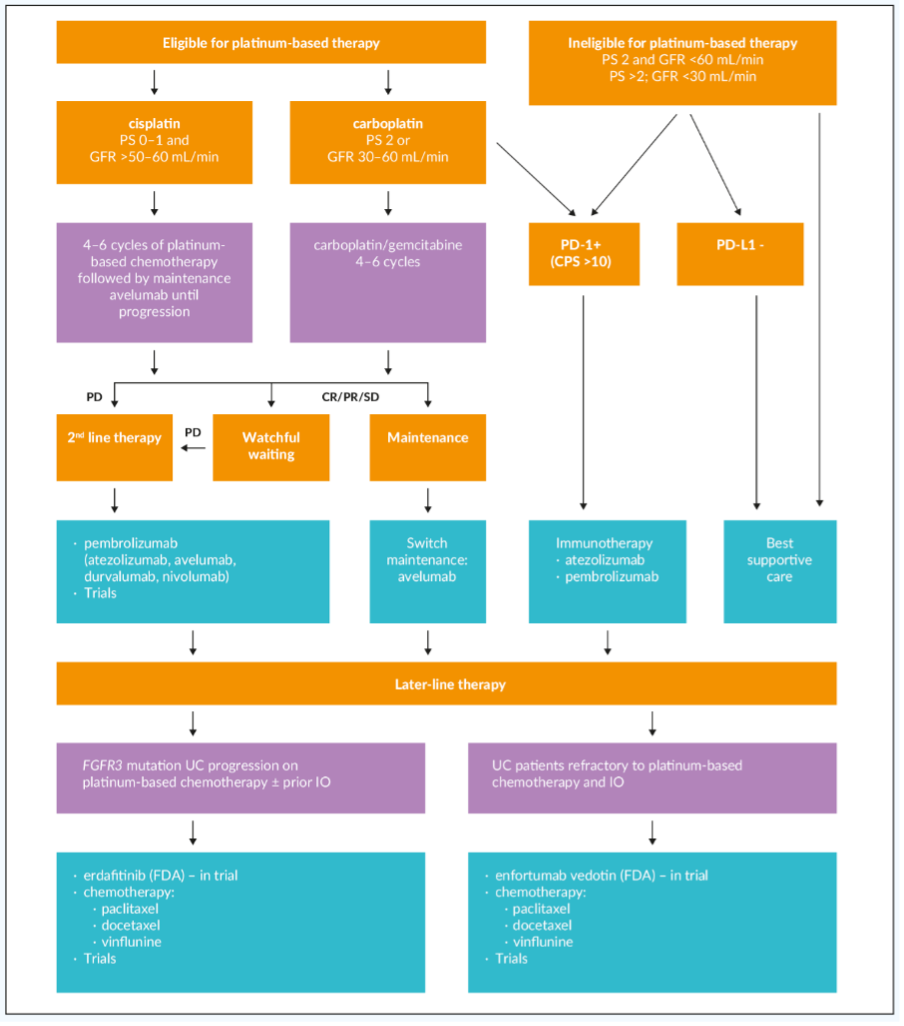
PD-1/PD-L1 inhibitors have redefined the standard of care for bladder cancer in different ways and treatment lines (Figure 3). Three of these agents, atezolizumab, nivolumab and pembrolizumab, are approved in Switzerland for the treatment of adult patients with locally advanced or metastatic UC who have received prior platinum-containing chemotherapy of those pembrolizumab has the highest evidence from a randomized phase III trial.3–5 Recently, avelumab was approved by EMA25 and Swissmedic26 as monotherapy for first-line maintenance therapy in patients with locally advanced or metastatic UC whose disease has not progressed on first-line platinum-based induction chemotherapy. First-line atezolizumab and pembrolizumab are also approved in advanced UC patients who are considered cisplatin-ineligible and whose tumors have high PD-L1 expression, although with low evidence from single-arm phase II trials.17 In Switzerland, pembrolizumab is currently the only ICI approved in advanced UC patients with PD-L1-positive tumors and who are cisplatin-ineligible.27 Erdafitinib for patients with FGFR2,3 or some other alterations and enfortumab vedotin are not yet approved in Europe or Switzerland but have already entered guideline recommendations due to positive phase II and III trials. In Switzerland, erdafitinib and enfortumab vedotin can be offered to patients through a compassionate use program.

FUTURE PERSPECTIVES
Adjuvant treatment strategies for muscle-invasive bladder cancer have been limited to those being Cisplatinum-fit and have not received neoadjuvant treatment. For those not being able to receive cisplatin, no specific adjuvant treatment is recommended. The beneficial role of PD-1 and PD-L1 inhibitors in advanced or metastatic UC has given rationale for conceptualizing clinical trials with these drugs also in the adjuvant setting. Although IMvigor-010 with atezolizumab versus placebo observation did not meet its primary endpoint, data from an exploratory analysis showed that patients with muscle-invasive bladder cancer (MIBC) who had detectable circulating tumor DNA (ctDNA) were more likely to benefit from treatment with adjuvant atezolizumab monotherapy, compared with those without ctDNA negative ones (median disease-free survival [DFS], 5.9 months vs 4.4 months).29 At an interim analysis, OS was superior favoring atezolizumab versus observation in the ctDNA-positive population (median, 25.8 months vs 15.8 months; HR: 0.59 [95% CI: 0.41–0.86]). These data further improve our understanding of the disease and will inform a new phase III study in patients with ctDNA-positive MIBC.
In the double-blind CheckMate-274 trial, nivolumab treatment for up to 12 months following radical surgery in patients with high-risk MIBC resulted in a statistically significant and clinically meaningful improvement in the first endpoint DFS in this setting (21.0 months vs 10.9 months with placebo; HR: 0.70 [95% CI: 0.54−0.89]; p<0.001).30 DFS in the subgroup of patients with PD-L1-positive tumors was also improved with nivolumab; however, the median was not yet reached by the time of analysis. In terms of secondary endpoint, non-urothelial tract recurrence-free survival (NUTRFS) was also improved with nivolumab versus placebo in both intention-to-treat (ITT) population (24.6 months vs 13.7 months; HR: 0.72 [95% CI: 0.58−0.89]) and in patients with PD-L≥1% (not reached vs 10.9 months with placebo; HR: 0.54 [95% CI: 0.38−0.77]). Finally, OS data are still immature and most likely have to be awaited to announce before adjuvant nivolumab would become a truly practice-changing standard of care. Furthermore, the results from the ongoing AMBASSADOR Alliance trial will help broaden our understanding of the role of adjuvant immunotherapy, in particular, how pembrolizumab given post-cystectomy might improve survival outcomes in patients with high-risk MIBC.31
Recent trials showing a pathological response with immunotherapy in the neoadjuvant setting include the phase II ABACUS32 and PURE-0133 studies, which demonstrated promising results with atezolizumab and pembrolizumab in pre-surgical UC patients. Combination regimens of chemotherapy and immunotherapy agents in the neoadjuvant setting are also being evaluated in phase II clinical trials (e.g., BLASST-134).
For the time being, classic neoadjuvant chemotherapy will remain the standard of care for patients for MIBC patients from T2 muscle-invasive disease who are cisplatin-fit. The VESPER phase III trial recently presented at the ESMO meeting showed superiority in terms of metastatic PFS at 3 years and OS and an impressive pathological complete response (pCR) rate of 6 cycles of dose-dense methotrexate, vinblastine, doxorubicin and cisplatin (MVAC).35 Therefore, dose dense MVAC should be considered the regimen of choice in the neoadjuvant setting for those patients fit enough to receive this potentially more effective, thus toxic treatment.
Conclusions
-
Based on recent practice-changing trials, platinum-based chemotherapy followed by an immune checkpoint inhibitor (ICI) as a switch maintenance concept, in patients not progressing on chemotherapy, responding or stable disease has become the current gold standard of care for patients with advanced or metastatic urothelial cancer (UC).
-
First-line ICI such as pembrolizumab or atezolizumab is an option for cisplatin-ineligible patients who have high PD-L1 expression, while second-line ICI immunotherapy offers an additional option for patients progressing during or after initial platinum-based chemotherapy.
-
Several factors such as FGFR mutational status, comorbidities and adverse events should be established taken into consideration for the decision of third-line treatment of advanced UC patients with erdafitinib or enfortumab vedotin. These agents, although are not yet approved in Switzerland, but available through a compassionate use program.
-
The use of ctDNA and other biomarkers will provide further insights and enable a more individualized treatment approach, provided large ongoing prospective trials will confirm their utility.
CONFLICT OF INTEREST
The author declares that the study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Author Contributions
The author crafted and approved the final manuscript.