INTRODUCTION
Non-small cell lung cancer (NSCLC) accounts for 85% of all lung cancer cases,1 of which approximately 10−20% harbor epidermal growth factor receptor (EGFR) mutations. In the Asian population, this number can reach up to 50% amongst patients with lung adenocarcinoma, particularly in women and non-smokers.2,3 EGFR mutation rate is higher in lung adenocarcinoma with papillary, acinar or lepidic component than with solid or mucinous one.
Identification of a possible “druggable” mutation has become the standard of care after the diagnosis of metastatic NSCLC. The most frequently mutated gene is the EGFR gene. Several types of mutations within the EGFR gene have been described, and the response to the targeted therapy with one of the tyrosine kinase inhibitors (TKIs) such as erlotinib, gefitinib, afatinib, dacomitinib and osimertinib may depend on the type of mutation.
Osimertinib is a third-generation irreversible EGFR TKI that is approved as a first-line agent in the treatment of patients suffering from metastatic NSCLC and harboring the most common genetic alterations. It is also approved for patients with progressing lung tumor under first-generation TKIs and with an additional mutation T790M responsible for the resistance. On the other hand, there is still no mature data concerning osimertinib’s clinical efficacy in uncommon mutations because of their high molecular heterogeneity and low prevalence.
Here, we present the case of a patient with two simultaneous very rare EGFR mutations in exon 21 (p.L833V and p.H835F) who showed a satisfactory response to osimertinib.
CASE PRESENTATION
The patient was a 55-year-old female with no comorbidities. She had a smoking history of 10 patient-years (py) and stopped smoking more than 25 years ago.
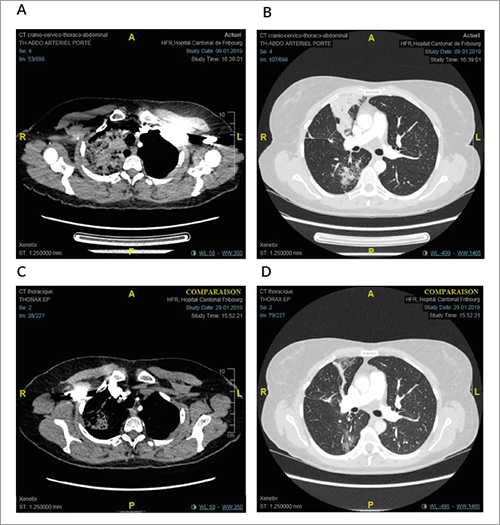
Multiple diffuse bilateral alveolar condensations with air bronchogram, predominately in the right lung (Figure 1A and 1B), were incidentally discovered on a cervical magnetic resonance imaging (MRI) performed to investigate cervical discomfort. Patient was symptomatic with respiratory wheezing, dyspnea stage I and significant fatigue. Complete pulmonary function tests showed nonobstructive or restrictive ventilation disorder, a normal carbon monoxide diffusion capacity and normal airway resistance.
**_and**b)**images_of_the_initial_ct_scans_performed_prior_to_treatment_with_osimert.png)
A bronchoscopic biopsy and endobronchial ultrasound bronchoscopy (EBUS) led to the diagnosis of a mixed mucinous and non-mucinous stage IVA (bilateral pulmonary tumor involvement) adenocarcinoma with the composition of 60% lepidic, 20% solid, 10% acinar, and 10% micropapillary. Unfortunately, the obtained biopsy material was not enough to perform a molecular analysis such as next-generation DNA sequencing (NGS).
In order to obtain a sufficient tissue sample, a diagnostic unilateral, extra-anatomical partial resection of the upper and middle right lobe and station 4 right lymph node dissection was performed. The histopathological analysis confirmed the diagnosis of the adenocarcinoma of the lung, and the NGS analysis (Ion AmpliSeqTM Oncomine Focus, Ion Torrent S5) showed two simultaneous EGFR mutations in exon 21 (p.L833V and p.H835F). Furthermore, no other mutations (BRAF, KRAS, PIK3CA, MEK1, AKT1, ERBB2, TP53) or translocations (ALK, RET, ROS1) were detected. As assessed by immunohistochemistry, the expression of the programmed death-ligand 1 (PD-L1) was very low (<1%).
As the patient was doing well and there was no absolute indication to start chemotherapy, we decided to initiate targeted therapy with osimertinib (80 mg/day cont.). Four weeks later, the patient suffered from mild dyspnea. In order to exclude a pulmonary embolism, a chest CT scan was performed (Figures 1C and 1D). This exam showed no evidence of an embolism but a very good partial response with marked reduction in bilateral pulmonary infiltrates. The mild dyspnea resolved within few days and the response was maintained with an excellent quality of life.
Nine months after osimertinib therapy had been initiated, the CT scan in October 2019 revealed disease progression in the upper right lobe with a new mediastinal lymph node metastasis. Clinically, the patient remained asymptomatic. At this stage, treatment with osimertinib was stopped, and platinum-based chemotherapy (cisplatin with pemetrexed) was initiated. Prior to chemotherapy, an NGS analysis was repeated (by ultrasound-guided transbronchial biopsy) and showed the same uncommon exon 21 EGFR mutations (p.L833V and p.H835F). In addition, the analysis revealed an exon 5 TP53 alteration (p.R181H), which was not detected initially and could potentially explain the acquired resistance to osimertinib.
DISCUSSION
Here we report the case of a patient with advanced NSCLC harboring an uncommon mutation in exon 21 who was responding to osimertinib for 9 months and developed resistance due to an acquired TP53 mutation.
Roeper et al. (2020) demonstrated that TP53 co-mutations are frequent in EGFR mutated lung adenocarcinoma.4 In addition, the study showed that the TP53 mutations were independent of the type of EGFR mutation. The TP53/EGFR mutation profile was associated with reduced overall response rates (ORRs) as well as poor progression-free survival (PFS) and overall survival (OS). Of note, those patients develop cerebral metastases more often than patients with an EGFR mutation and unmutated TP53. In a retrospective, multicenter study of lung cancer patients who had developed resistance to osimertinib, Zhao et al. (2020) show that pathogenic mutations of TP53 were negatively related to the efficacy of osimertinib.5
The mutations reported in our patient (p.L833V and p.H835F) have already been described in coexistence with a third mutation (E709K) in a 70-year-old male former smoker (30 pack-years) who quit smoking 26 years before the diagnosis of lung cancer was made.6 The patient suffered from a metastatic lung adenocarcinoma with a pleural carcinomatosis and liver metastases. Treatment with afatinib (40 mg daily) led to a partial response two months after treatment initiation. The duration of response was not reported.
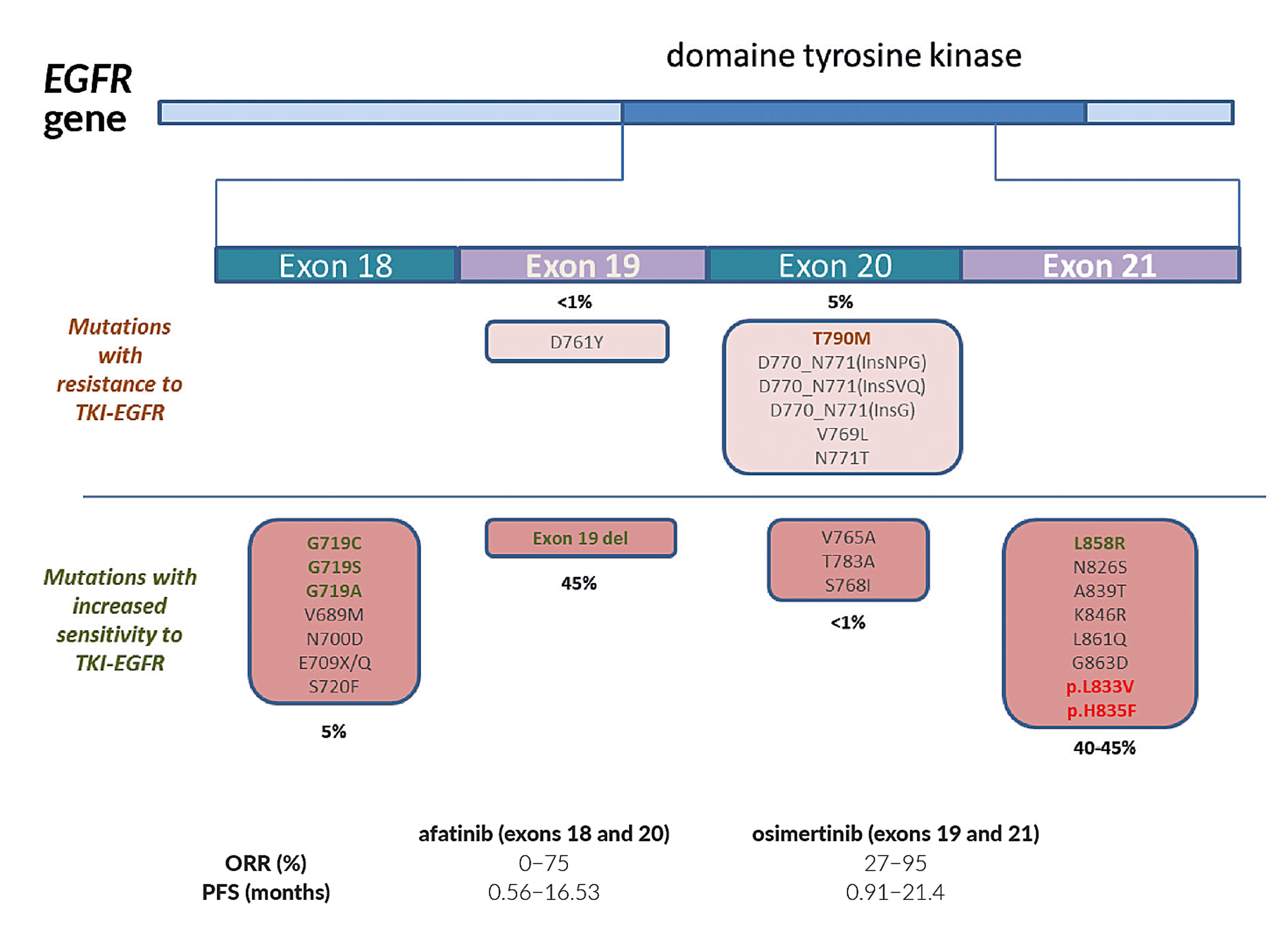
A number of studies have demonstrated the high activity of TKIs in tumors with exon 19 deletions and exon 21 L858R substitutions, leading to a median PFS of 12−18 months and a significant improvement in quality of life.7,8 On the other hand, patients with uncommon EGFR mutations respond less frequently, with responses and survivals being worse.9–11 In fact, tumors with uncommon EGFR mutations, like G719X (exon 18), S768I (exon 20), L861Q (exon 21), substitutions or exon 20 insertions, showed lower rates of responses to reversible TKIs, including gefitinib and erlotinib (Figure 2). However, irreversible pan-human EGFR inhibitors such as afatinib improved overall responses but not OS.12–14

When treated with a TKI, patients with a common and an uncommon EGFR mutation have shown shorter PFS as compared with patients with only one common mutation.21–25 On the other hand, chemotherapy and checkpoint inhibitors seem to be more active in this patient population.26,27 Today, no globally accepted therapeutic strategy has been established. Treatment of patients with uncommon EGFR mutations remains a subject of debate in the era of considerable progress in targeted therapies and immunotherapy.26,28–31
CONCLUSIONS
To our knowledge, this is the first presentation of a patient with a lung cancer harboring a combination of two rare, uncommon EGFR mutations in exon 21 and showing a response to osimertinib with a PFS of 9 months. However, the development of a TP53 mutation under treatment led to osimertinib resistance. Thus, the role of osimertinib in patients with uncommon EGFR mutations should be further studied.
TAKE-HOME MESSAGES
-
Patients with metastatic NSCLC harboring uncommon and compound mutations (including a rare one) in the EGFR gene show a lower tumor response rate to first generation TKIs, as well as a shorter progression-free survival (PFS) compared with those with common exon 19 and 21 mutations.
-
Second (afatinib) and third (osimertinib) generation TKIs should be considered in those cases.
-
In this patient presentation we show response to osimertinib in a NSCLC patient with two uncommon EGFR mutations in exon 21 (p.L833V and p.H835F).
-
The presence of a TP53 co-mutation detected in the relapsing tumor was responsible for resistance development.
Informed Consent
General written consent was obtained from the patient for the publication of this case report and any accompanying images.
COI
The authors declare that the study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Author Contributions
All authors contributed to and approved the final manuscript.