BACKGROUND
Merkel cell carcinoma (MCC) is a rare neuroendocrine carcinoma of the skin, which originates most frequently in the areas of skin exposed to the sun. It can be caused by UV-induced DNA damage or by an infection with the Merkel cell polyomavirus (MCPyV).1,2 It is more prevalent in older people and people with iatrogenic or pathologic immunosuppression. The choice of treatment regimens for MCC depends on disease characteristics, such as stage, location, involvement of regional lymph node and comorbidities.1
Patients with locoregional MCC, which accounts for 65–70% of the cases at diagnosis, typically undergo surgical resection followed by adjuvant radiotherapy. Even after definitive therapy for local MCC, recurrence rates are 35% at 3 years and distant metastases develop frequently.3 In patients with localized MCC, the 5-year overall survival rate is 55.6%. In patients with advanced disease, the 5-year survival rate is 35.4% for those with regional nodal disease and 13.5% for those with distant metastases.3 Until very recently, treatment for advanced MCC was based on chemotherapeutic protocols used for small cell lung cancer, as both are cancers of neuroendocrine cells, aggressive and poorly differentiated.1
Thus, systemic chemotherapy typically includes platinum agents, such as carboplatin or cisplatin, and etoposide, anthracyclines, taxanes or topotecan, in different combinations or as a monotherapy. Although the disease can be initially sensitive to these chemotherapy regimens, responses are usually short in duration with median progression-free survival (PFS) of less than 10 months. Chemotherapy has not demonstrated significant improvement in overall survival (OS) and is often associated with significant cytotoxicity.1,2,4 In 2 real-world analyses, the median duration of response in metastatic MCC patients receiving second-line chemotherapy was only 1.9 and 1.7 months, respectively.2,4 The 12-month survival rate of these patients was 0%.2 Response rates in the second-line setting are much lower in patients with known distant metastases compared with patients with unknown metastasis sites. Regardless of the line of therapy, disease recurs in most patients by 6 months.2,4 Adjuvant chemotherapy has been associated with increased morbidity, decreased quality of life and immunosuppression, but with no clear benefit. It is therefore not recommended in clinical guidelines.1
Recent advances in our understanding of MCC has led to the development of a spectrum of therapeutic options, especially immunotherapeutic approaches. Furthermore, a number of ongoing clinical trials are currently investigating the efficacy and safety of different first- and second-line treatment alternatives in advanced MCC. Pembrolizumab, a monoclonal antibody against PD-1, was the first immune checkpoint inhibitor to demonstrate objective tumor regressions in patients with MCC. The phase II KEYNOTE-017 trial demonstrated an overall response rate (ORR) of 56%, as well as a 24% complete response rate and a 32% partial response rate, in treatment-naïve patients. Based on these results, pembrolizumab has been approved by the FDA for treatment of metastatic MCC regardless of the line of therapy. However, in the EU and Switzerland, it is approved for the treatment of other types of cancers like lung cancer and melanoma but not mMCC. Nivolumab is another monoclonal anti-PD-1 antibody being studied in clinical trials for the treatment of mMCC. The CheckMate 358 compared nivolumab in the first- and second-line settings in patients with virus-associated MCC and found that it was effective in both settings (ORR: 73% in treatment naïve patients, 50% in previously treated patients) and had a good safety profile. However, nivolumab is only recommended by NCCN but not approved by the Swiss Agency for Therapeutic Products (Swissmedic). Finally, avelumab, an immune checkpoint inhibitor (ICI) which blocks PD-L1, was approved in the USA and EU in 2017 regardless of the treatment line.5–7 Based on the Javelin Merkel 200 (JM 200) study, avelumab received approval also by Swissmedic in the same year for the pre-treated metastatic MCC.8 In January 2019, it received a first line extension in Switzerland for the treatment of metastatic MCC.
Here, we report the case of a patient with metastatic Merkel cell carcinoma which demonstrates that treatment with avelumab can be effective and manageable.
CASE PRESENTATION
The 60-year old patient was admitted in September 2017 to the emergency unit of a cantonal hospital. He had been suffering from worsening pain, initially in the left upper abdomen, then shifting to the left flank, as well as mild constipation for several days. The patient had diabetes mellitus and hypothyreosis of unclear cause and with no history of thyroid surgery. He also had a myocardial infarction in 2013, which resulted in the implantation of 2 stents. In July 2017, he had also suffered from urolithiasis. A CT scan found a retroperitoneal mass (15 cm x 10 cm x 10 cm) and displacement of the aorta, left iliac vessels and the left ureter with consecutive grade 2 congestion in the left-side pelvicalyceal system. The day after he was admitted to the hospital, retrograde ureteropyelography was performed and a tumor stent was implanted. Ten days later, a CT-guided biopsy of the retroperitoneal mass was performed. Histology revealed a necrotic, neuroendocrine carcinoma with a Ki-67 level of 60%. Immunohistochemistry showed a positive reaction to pan-cytokeratin, CK-20, CK-8/18, chromogranin A and synaptophysin, and a negative reaction to TTF-1, GATA-3, CDX-2, CK-7 and vimentin. The PCR test was positive for polyomavirus and therefore the diagnosis of Merkel cell carcinoma was concluded.
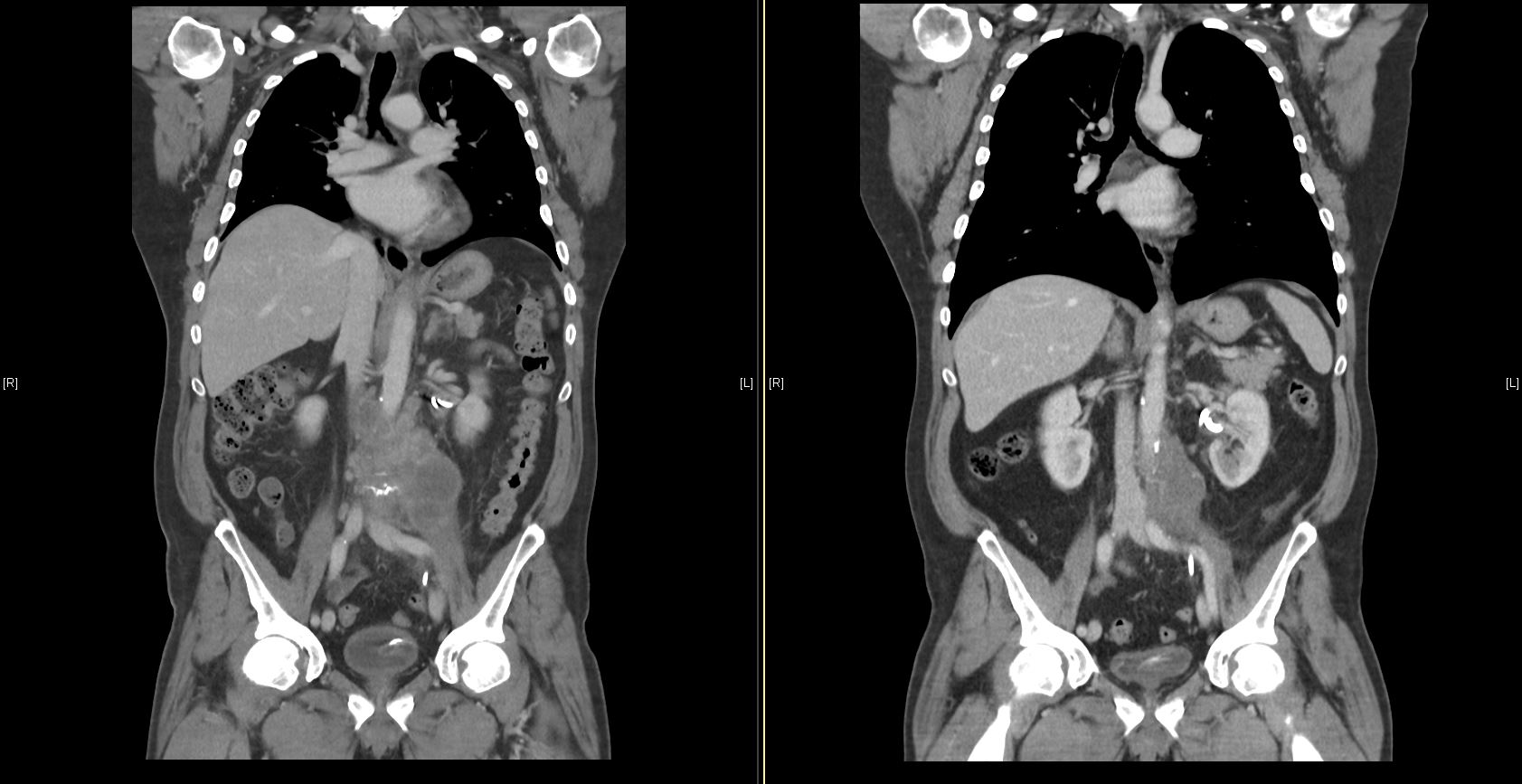
A PET-CT performed at the end of September 2017 revealed that the retroperitoneal tumor was progressing rapidly in size (Figure 1). In addition, it had also metastasized to multiple abdominal lymph nodes, including retroperitoneal, mesenteric, posterior inferior mediastinal and left retroclavicular localizations. Palliative chemotherapy (carboplatin and etoposide) was initiated in order to slow down the rapid tumor growth. It was continued for 2 cycles in the following 6 weeks, which led to a mixed response in the patient. The chemotherapy regimen was continued for further 6 weeks, as the patients achieved a partial response with a regression of the clinically significant lesions. In addition, between December 2017 and January 2018, palliative radiotherapy was conducted due to incipient vena cava infiltration. The subsequent CT showed a regression of the irradiated retroperitoneal tumor regions, whereas a progression of the tumor was evident in the supraclavicular, paraoesophageal and tonsillar regions.
__ct_scan_after_avelu.jpg)
In February 2018, treatment with avelumab (10 mg/kg body weight IV) was initiated. After 3 months of treatment, the disease had stabilized and partial remission was achieved after 9 months (Figure 1). The patient tolerated the regimen very well, showing no adverse effects. In March 2019, due to a localized tumor growth, the paratracheal lymph node was treated with radiation therapy. Afterwards, a local complete response and a systemically ongoing partial response was achieved (-51.3% of the total tumor volume according to iRECIST criteria).
DISCUSSION AND LITERATURE REVIEW
Immunotherapy uses the intrinsic immune system to fight cancer. A common strategy in immunotherapy – first established for melanoma - is to inhibit immune checkpoint proteins, like programmed cell death protein (PD-1) and programmed death-ligand 1 (PD-L1). Avelumab, a humanized monoclonal antibody, is an immune checkpoint inhibitor (ICI) which blocks PD-L1 and is now commonly used to treat advanced stage MCC. In 2017, it became the first drug to be approved for MCC in the USA and EU regardless of the treatment line, and in Switzerland avelumab was approved for the second-line treatment of metastatic MCC.5–7
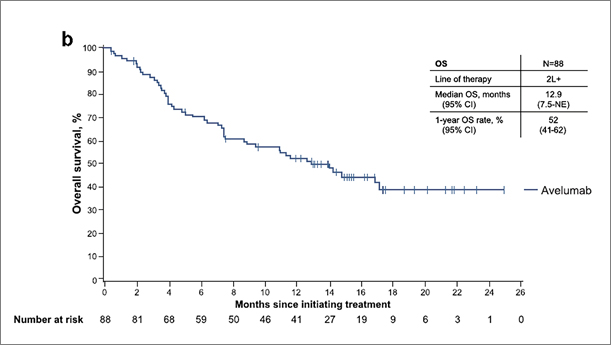
JM 200 is an international, open-label, single-arm, multicenter phase II clinical trial that was designed in 2 parts (Part A and B) to assess the safety and efficacy of avelumab in patients with metastatic MCC (mMCC).8 Part A included patients with mMCC whose disease had progressed after at least one line of chemotherapy.8,9 Part B is ongoing and includes patients with histologically confirmed mMCC who were treatment-naïve to systemic chemotherapy.10 The study showed that pre-treated MCC patients experienced durable responses after avelumab therapy. With a median follow-up of 10.4 months, 32% of the patients have achieved an objective response. 11.4% of the patients achieved complete response (CR), and 21.6% partial response (PR). The duration of response was ranging from 2.8 to at least 23.3 months.11,12 The median PFS was 2.7 months. Two-year data from JM 200 for pre-treated patients confirmed the 1-year objective response rate (ORR) (33%).9 Median overall survival (OS) was 12.9 months and the 2-year survival rate was 36% (vs 52% at 1 year) (Figure 2). In addition, PFS rate was durable: 29% at 12 months and 26% at 24 months.9 No new safety signals were identified for avelumab with a minimum follow-up of 2 years.9
_in_patients_with_metastatic_merkel_cell_car.jpg)
Furthermore, in treatment-naïve patients (Part B) from JM 200, objective response was achieved in 62% patients (n=29), with 14% of the patients experiencing CR and 48% of patients experiencing PR. The 3-month PFS was 67%, and the median PFS was 9.1 months.10
A real-world experience showed that the efficacy and safety of avelumab in pre-treated mMCC patients was consistent with results from the JM 200 study.13 Patients in a global expanded access program (EAP) could have, in contrast to JM 200, Eastern Cooperative Oncology Group (ECOG) Performance Status (PS) of 0–2, treated brain metastases or immunosuppressive conditions. Avelumab was associated with an ORR of 52.5% patients, including 3 immunocompromised patients who achieved CR and 1 patient who achieved PR.14
Thus, recent progress in immunomodulatory therapies have provided effective treatment alternatives for patients with advanced MCC. Avelumab has shown promising results in clinical trials including patients with metastatic, MCPyV-positive and -negative MCC. Based on these results, it is recommended by the 2019 NCCN guidelines for treatment for distant mMCC.15,16 In addition, among other ICIs available for treating patients with mMCC, including pembrolizumab and nivolumab, only avelumab is approved by the U.S. Food and Drug Administration (FDA), European Medicines Agency (EMA) and Swissmedic.5–7 Recently, it received approval for treatment in the first-line setting also in Switzerland. Thus, the introduction of avelumab has significantly improved the therapeutic armamentarium of metastatic Merkel cell carcinoma.
Conclusion
MCC is an immunogenic tumor and clinical data suggest that patients with unknown primary tumor and lymph node involvement have a better prognosis than patients with a known primary tumor at the same stage IIIB, suggesting that the immune system plays a role in tumor growth control. However, efficacy of chemotherapy in stage IV, as described in this patient, has been very limited even in the absence of a primary tumor. Based on the clinical study data summarized above, ICI first-line therapy can be considered as a practice-changing development for mMCC, irrespective of the polyomavirus status of the tumor. The safety profile of ICIs is well known, with up to 20% of the patients experiencing adverse events of grade 3 or higher. Most importantly, the typical toxicity of this class of drugs is manageable in experienced hands. Furthermore, it has also been shown that early ICI treatment is associated with better outcome. Thus, PD1/PD-L1 inhibitors are the new standard of care for mMCC and avelumab has been approved for first-line treatment in Switzerland. Based on the therapeutic success of ICI in mMCC, several adjuvant and neoadjuvant clinical studies are currently ongoing. So far, the results of these studies have shown negative results for ipilimumab in the adjuvant setting and a positive signal for neoadjuvant treatment with nivolumab. Further results are pending. The definition of predictive factors for the effect of ICI therapy and the search for possible combination partners will be important study goals for the future of MCC treatment.
Informed Consent
General written consent was obtained from the patient for the publication of this case report and any accompanying images.
COI
The authors declare that the study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
This publication is supported by an unrestricted educational grant from Merck (Schweiz) AG and Pfizer AG.
Author Contributions
All authors contributed to and approved the final manuscript.