Introduction
Chronic lymphocytic leukemia (CLL) is the most common type of leukemia in the Western world, with an age-adjusted incidence of approximately 4.6 cases per 100,000 persons per year.1 Its clinical course is highly heterogeneous, ranging from an indolent disease requiring observation alone to a rapidly progressive form that necessitates systemic therapy. The treatment landscape for CLL has evolved significantly over the past decades, driven by the introduction of chemotherapy-free targeted regimens.2 Bruton’s tyrosine kinase (BTK) inhibitors, a class of targeted small-molecule agents that inhibit the B-cell receptor signaling pathway, leading to reduced proliferation and apoptosis of malignant B-cells, have assumed a central role in the management of B-cell malignancies and largely displaced chemoimmunotherapy in routine clinical practice.3,4 Second-generation BTK inhibitors, such as acalabrutinib and zanubrutinib, were developed to preserve efficacy while reducing off-target toxic effects, particularly cardiovascular toxicity frequently observed with first-generation agents.5–13 Contemporary treatment guidelines place BTK inhibitor-based therapy among the preferred first-line options for CLL and also incorporate combinations with venetoclax and CD20-targeting monoclonal antibodies, with treatment selection guided by TP53/del(17p) and IGHV mutation status, the presence of complex karyotype and patient fitness.14
Venetoclax, a selective inhibitor of the anti-apoptotic protein B-cell lymphoma 2 (BCL-2), represents another key targeted agent in CLL therapy.15,16 By restoring mitochondrial apoptosis in malignant cells, venetoclax provides potent cytoreductive activity and has enabled the development of time-limited, chemotherapy-free treatment strategies. Its use requires structured dose escalation and tumor lysis syndrome risk mitigation, but when appropriately monitored, venetoclax-based regimens offer an effective approach for achieving deep remissions while avoiding continuous therapy. The combination of BTK inhibition with venetoclax is therefore supported by a strong biological rationale, as it integrates complementary mechanisms of disease control within a fixed-duration regimen.
The phase III AMPLIFY trial provided pivotal evidence for acalabrutinib-based combinations in previously untreated CLL.17 In this open-label, multicenter study, 867 patients without del(17p) or TP53 mutation were randomly assigned in a 1:1:1 ratio to receive fixed-duration oral acalabrutinib plus venetoclax, acalabrutinib plus venetoclax and CD20-targeting monoclonal antibody obinutuzumab, or the investigator’s choice of chemoimmunotherapy (fludarabine-cyclophosphamide-rituximab or bendamustine-rituximab). At a median follow-up of 40.8 months, the study met its primary endpoint, with a 36-month progression-free survival (PFS) rate of 76.5% with acalabrutinib plus venetoclax versus 66.5% with chemoimmunotherapy (HR: 0.65 [95% CI: 0.49–0.87]; p=0.004). The triplet arm yielded a 36-month PFS of 83.1% (p<0.001 vs chemoimmunotherapy). These findings established fixed-duration acalabrutinib plus venetoclax as an effective, all-oral frontline option in CLL, defining a new treatment paradigm that combines therapeutic efficacy with a defined course of therapy. In Switzerland, the combination of acalabrutinib plus venetoclax is approved for adult treatment-naïve patients with CLL, whereas the use of the triplet regimen incorporating obinutuzumab is not currently authorized.18
Here, we describe a case of successful application of fixed-duration acalabrutinib plus venetoclax according to the AMPLIFY regimen in a patient with IGHV-mutated CLL without del(17p)/TP53 mutation and rapid disease progression after an initial watch-and-wait period.
Case presentation
Clinical presentation and diagnostic work-up
A 46-year-old man was referred to the hematology outpatient clinic in February 2023 after incidental detection of leukocytosis during a primary care evaluation for ear pain and fatigue. Mild fatigue had been present since a prior coronavirus infection approximately one year earlier and was not initially considered disease-specific. The first blood test performed on February 02, 2023, showed leukocytosis of 44.4 ×109/L with 67% lymphocytes. A repeat blood test on February 07, 2023, confirmed persistent lymphocytosis, with a leukocyte count of 29.5 ×109/L and lymphocyte count of 23.6 ×109/L. Baseline laboratory testing at the initial hematologic assessment showed hemoglobin level of 14.2 g/dL, platelet count 144 × 109/L, smudge cell count of 6.0 × 109/L, β2-microglobulin level of 2.1 mg/dL, lactate dehydrogenase (LDH) level of 226 U/L, IgG 6.78 g/L, IgA 0.75 g/L, IgM 0.52 g/L and IgG subclasses within the normal range.
Peripheral blood immunophenotyping performed on February 16, 2023, showed a typical CLL phenotype, with a B-cell population expressing moderate levels of CD5, CD200, HLA-DR and CD43, and weak levels of CD23, CD20 and CD25, with partial CD11c positivity. The cells were negative for sIgM, FMC7, CD79b, CD10, CD38, CD103 and CD22. Surface and cytoplasmic light chain restriction was consistent with kappa clonality. The Matutes score was 5/5.
Abdominal ultrasound performed on February 13, 2023, revealed a spleen size of 13.9 cm with no hepatomegaly or abdominal lymphadenopathy. Subsequent sonographic assessment of the abdominal and peripheral lymph nodes on February 27, 2023, demonstrated several small bilateral cervical and axillary lymph nodes with cortical thickening measuring 8–10 mm, while the splenic size remained at 13.9 cm.
Diagnosis and treatment recommendations
Based on persistent lymphocytosis and a characteristic peripheral blood immunophenotype, the patient was diagnosed with CLL. The key diagnostic and therapeutic milestones are listed in Table 1. The diagnosis was confirmed at the institutional hematology tumor board on March 15, 2023, and a watch-and-wait strategy was recommended. Bone marrow examination was deferred given no indication for treatment at that time. The disease was classified as Binet stage A/Rai stage 0, consistent with the absence of anemia, clinically significant thrombocytopenia, bulky lymphadenopathy or CLL-related constitutional symptoms. The small cervical and axillary lymph nodes detected sonographically were not considered clinically significant.
Because of the patient’s relatively young age, the tumor board recommended additional prognostic characterization despite the absence of an immediate treatment indication. Molecular testing performed in September 2023 demonstrated mutated IGHV status, no TP53 mutation and no del(17p); del(13q) was reported as a favorable prognostic feature. The International Prognostic Score for for Asymptomatic Early-Stage CLL (IPS-E) was 2, indicating a high-risk disease.
Surveillance and disease progression
The patient remained on active surveillance through 2024 and early 2025. During this period, lymphocyte counts increased steadily; the patient remained largely asymptomatic, with no B symptoms apart from persistent fatigue, no palpable lymphadenopathy or infectious complications. Splenic enlargement became evident on interval imaging, reaching 18 cm by February 2024. Laboratory evaluation on March 10, 2025, showed disease progression with a leukocyte count of 344 × 109/L, lymphocyte count of 237 × 109/L, Gumprecht’s umbra 72 × 109/L, hemoglobin level of 12.2 g/dL and platelet count of 85 × 109/L. Repeat testing again showed no del(17p) or TP53 mutation.
Therapeutic interventions and outcome
Given the rapid disease kinetics with evolving anemia and thrombocytopenia, the case was reviewed at the institutional tumor board on March 12, 2025. Considering the patient’s young age, presence of mutated IGHV, absence of high-risk molecular markers and the patient’s preference for an oral-only treatment regimen, fixed-duration acalabrutinib plus venetoclax per the AMPLIFY regimen17 was recommended as first-line therapy. A reimbursement request was submitted on March 13, 2025, and approved five days later.
The treatment was initially scheduled for May 2025 at the patient’s request but was initiated earlier due to hospitalization from April 19 to 25, 2025, for fever of unknown origin accompanied by a generalized maculopapular rash. Following the exclusion of specific infections, the symptoms were attributed to a mixed viral/inflammatory syndrome in the setting of active CLL. A drug-induced exanthema due to allopurinol, which had been administered 7–10 days before the onset, was also considered a differential diagnosis. Fever and rash subsided following a short course of prednisone. An abdominal ultrasound performed on April 23, 2025, showed further splenic enlargement with a size of approximately 20.5 cm and a splenic volume of 1,550 mL, without hepatomegaly or intra-abdominal lymphadenopathy.
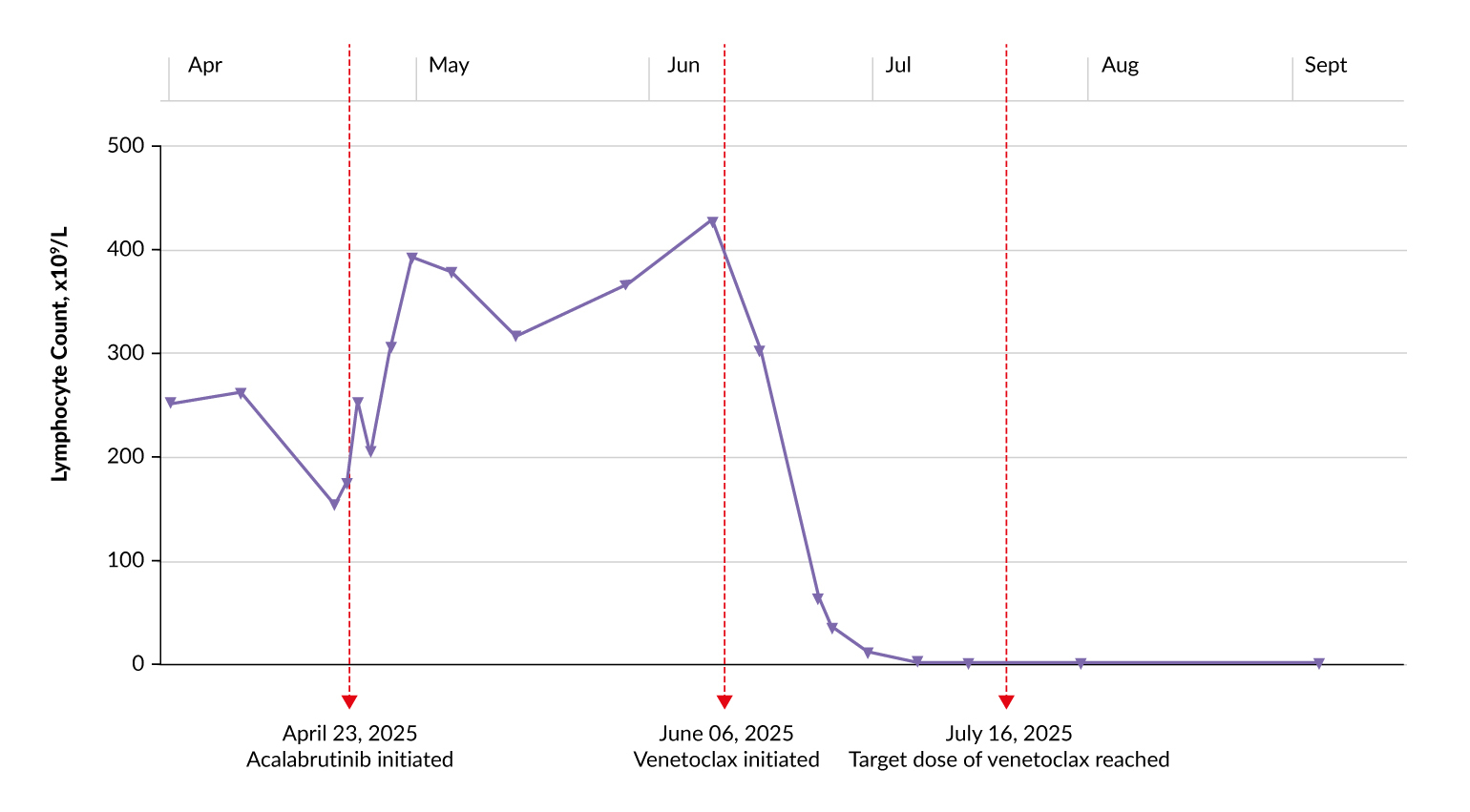
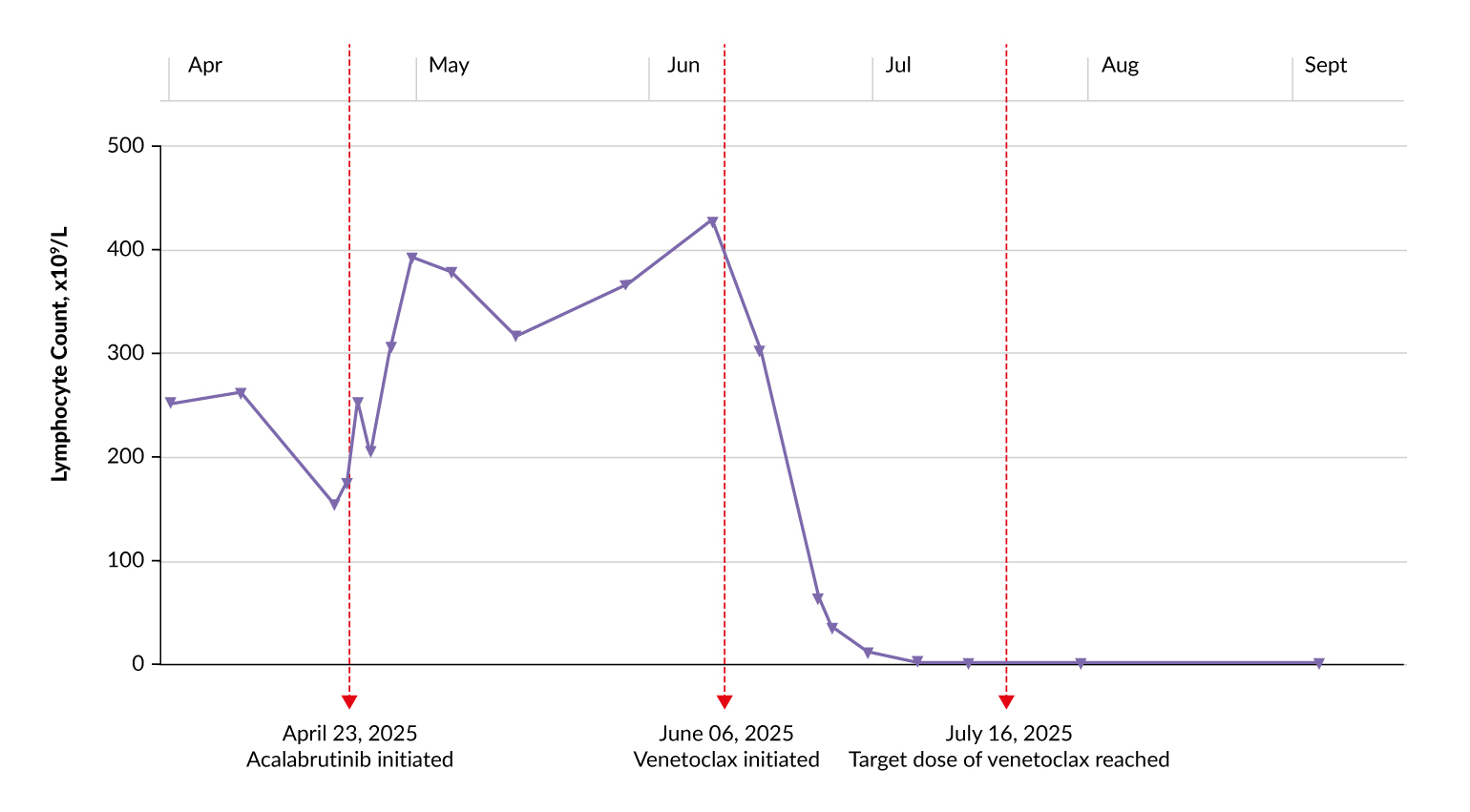
Acalabrutinib was initiated on April 23, 2025, at a dose of 100 mg twice daily for 28-day cycles 1–14. Venetoclax was administered once daily during cycles 3–14, including a 5-week ramp-up from 20 mg to the target dose of 400 mg once daily.
As expected with BTK inhibitor treatment, the early response was marked by transient redistribution lymphocytosis: the absolute lymphocyte count rose from 237 × 109/L on March 10, 2025, to 397 × 109/L on April 25, 2025, peaked at 414 × 109/L on June 11, 2025, and subsequently normalized rapidly upon venetoclax ramp-up (Figure 1).
The treatment was well tolerated, with no treatment interruptions or further hospitalizations due to treatment-related adverse events. No laboratory or clinical evidence of tumor lysis syndrome (TLS) was observed despite the discontinuation of allopurinol due to pruritus and eczema, and no relevant infectious complications were reported. A brief episode of dizziness occurred after venetoclax initiation. Organ function remained preserved overall, with stable renal parameters, no biochemical liver injury, normal LDH and no suspected intra-abdominal lymphadenopathy. Hemoglobin levels progressively improved from mild anemia at treatment initiation to the normal range by July 2025, with partial improvement in thrombocytopenia. At the time of the last follow-up (December 2025), the patient remained on ongoing therapy, with cycle 9 planned.
Discussion
This case illustrates the successful frontline application of fixed-duration acalabrutinib plus venetoclax in a patient with IGHV-mutated CLL who exhibited rapid disease progression following an initial observation period. While the patient’s initial Binet stage A disease justified observation, subsequent evolution characterized by progressive lymphocytosis, splenomegaly and the development of anemia and thrombocytopenia required therapeutic intervention. Contemporary treatment guidelines prioritize targeted agents over chemoimmunotherapy, particularly for younger patients who may require long-term disease management.14 The choice of acalabrutinib plus venetoclax was aligned with the patient’s molecular profile (mutated IGHV, absence of del(17p) and TP53 mutation) and clinical priorities, which included the desire for an all-oral, time-limited treatment course to minimize cumulative toxicity and preserve future therapeutic options.
The efficacy of the regimen is supported by the phase III AMPLIFY trial, which established fixed-duration acalabrutinib plus venetoclax as a standard-of-care frontline option in CLL.17 Our case translates these clinical trial findings into a real-world context, demonstrating a deep and rapid response in a patient with a high tumor burden. The observed treatment course was consistent with the known on-target response pattern observed with BTK inhibitor-based therapy followed by venetoclax-mediated debulking. After initiating acalabrutinib, the patient showed transient redistribution lymphocytosis, followed by a rapid decline in lymphocyte counts after venetoclax introduction and ramp-up, with normalization of the lymphocyte count during ongoing therapy.
The safety and tolerability of the combination observed in this case are particularly notable. Despite the patient’s high lymphocyte count at baseline, there was no evidence of TLS even after discontinuation of allopurinol, highlighting the feasibility of administering this regimen with careful TLS risk assessment and monitoring. The absence of treatment interruptions or serious adverse events, such as cardiovascular toxicity or major infections, contrasts favorably with the historical toxicity profiles of chemoimmunotherapy and first-generation BTK inhibitors. This favorable safety profile is consistent with the literature evidence demonstrating that acalabrutinib-based regimens are associated with lower rates of atrial fibrillation and hypertension than regimens based on the first-generation BTK inhibitors.7,8,10,11,13
Furthermore, this case illustrates the operational feasibility of this treatment strategy within the Swiss healthcare system and provides relevant practical information regarding access to this regimen in routine care. In particular, approval of the reimbursement request within five days underscores that fixed-duration acalabrutinib plus venetoclax can be implemented in a timely manner when the clinical indication is well documented and aligned with available trial evidence and national authorization status. Although the reimbursement process described here reflects a single case, and approval pathways, timelines and outcomes may vary in other situations, this aspect may be of particular value for clinicians managing patients with rapidly progressive CLL who require prompt treatment initiation and for whom administrative delays could compromise optimal disease control. By documenting the clinical rationale, molecular eligibility, treatment urgency and successful reimbursement process, this case may serve as a useful real-world reference for comparable future requests, representing an important translational step between regulatory approval and actual patient access to innovative targeted therapy. The patient’s preference for an oral-only regimen, which was accommodated, also reflects the growing emphasis on patient-centered care in oncology, where treatment choices are increasingly balanced with quality-of-life considerations.
Conclusions
In summary, this case reinforces the role of fixed-duration acalabrutinib plus venetoclax as a potent, safe and logistically feasible frontline therapy for patients with IGHV-mutated CLL. These data demonstrate how the application of targeted agents, guided by molecular diagnostics and supported by robust clinical trial data, can yield rapid disease control in patients with aggressive disease kinetics while minimizing the treatment burden.
Ethics approval and consent to participate
Written consent was obtained for the use of patient data.
Consent for publication
Consent for publication was obtained.
Availability of data and materials
All patient data that support this case report are included in anonymized form in the published article.
Conflict of interest
Adrian Schmidt declared receiving fees from Takeda, Janssen, Celgene, Sobi, Roche, Sanofi, Amgen, Beigene, Novartis, Incyte and Bayer. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way. Young-Lan Song declared that the study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The preparation of this article was financially supported by AstraZeneca. AstraZeneca had no decision-making role in the development of the manuscript and did not influence its content in any way.
Authors contributions
The authors created and approved the final manuscript.
AI use
The authors declared that no generative artificial intelligence (AI) or AI-assisted technologies were used in the preparation or writing of this manuscript. All content was produced entirely by the authors who take full responsibility for the accuracy, integrity and originality of the work.