Introduction
Approximately 40,000 new cancer cases are registered in Switzerland each year, with more than 60% of cases involving persons older than 65 years at diagnosis. The high proportion of older individuals among cancer patients is of major clinical importance since a variety of specific aspects such as frailty, nutrition, multimorbidity, organ dysfunction, polypharmacy and mental status has to be considered when treating this demographic group.1 Furthermore, the participation of older patients in clinical studies remains disproportionally low2 and relevant clinical endpoints may differ from those in other patient populations.3 The risk of both under- and overtreatment is elevated.4 Comprehensive geriatric assessment (CGA) is a complex, multidisciplinary evaluation strategy that mainly, but not exclusively, consists of assessments of functional status, comorbidities, cognitive function, psychological status, social functioning and support, nutritional status and polypharmacy. It also includes a detailed clinical evaluation by a multidisciplinary team consisting of oncologists, geriatricians and other experts. It facilitates informed decision-making regarding appropriate treatment strategies and is a well-established instrument in geriatric oncology with a proven positive impact.5 In order to provide such care at the Cantonal Hospital Baselland (KSBL) site Liestal, a medium-sized regional hospital in northwest Switzerland, we established a geriatric oncology service with the aim of evaluating patients through CGA and collecting data in the Prospective Registry for Older Patients with Cancer (PRO-PAC) to systematically assess clinical, functional and treatment-related information about this sensitive cohort of patients.
Methods
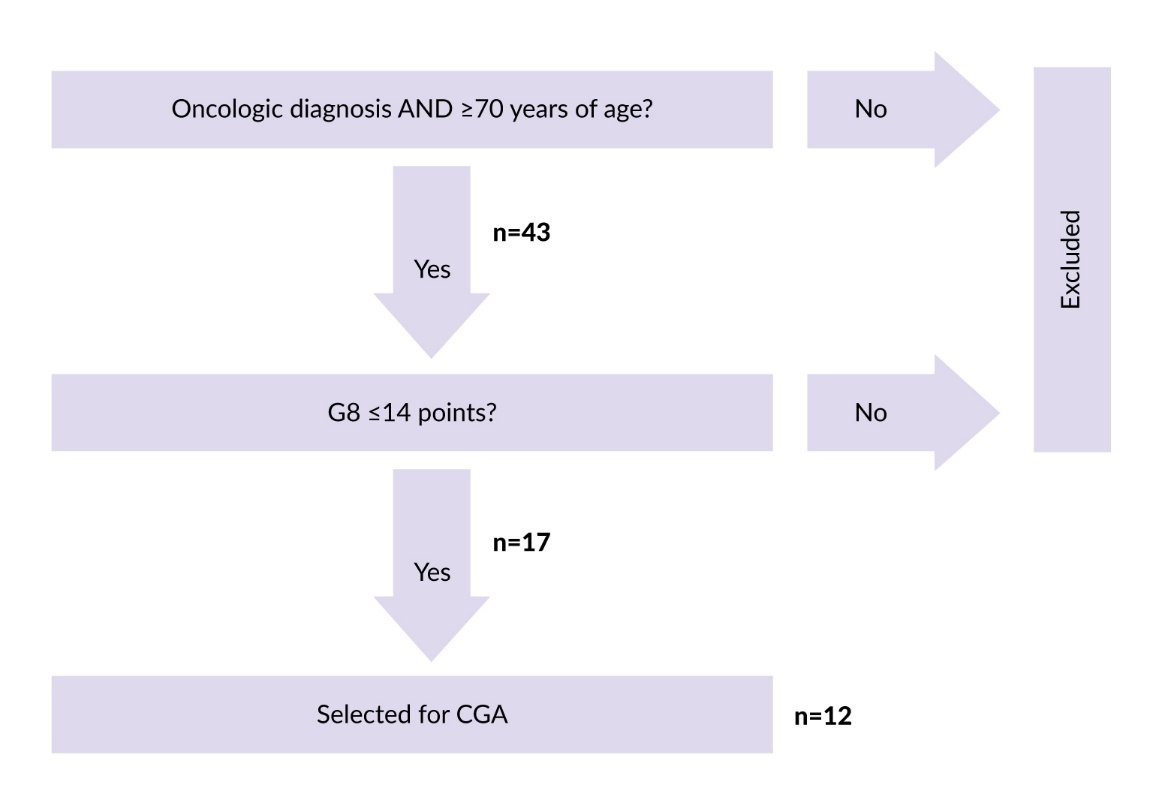
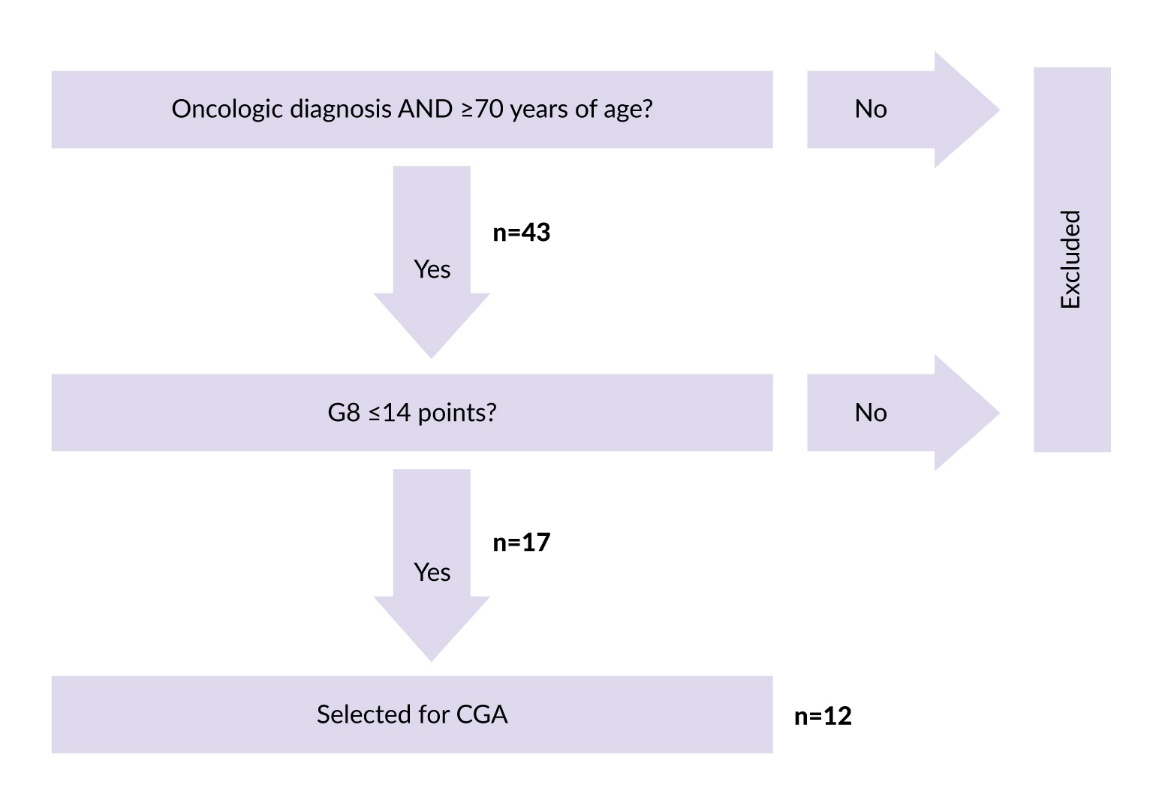
The aforementioned multidisciplinary geriatric oncology service was set up at our cancer center in January 2024, starting with a 9-month feasibility phase. In order to select patients potentially eligible for the evaluation by CGA, we assessed all patients aged ≥70 years with newly diagnosed solid tumors using the G8 screening tool (G-8).6 Those reaching a score of ≤14/17 were selected for CGA (see Figure 1 for the basic selection algorithm). These cut-off values were chosen in accordance with the current guidelines.7–10
The CGA consisted of two parts. First, the patients were evaluated by an oncology nurse, who assessed functional status (Barthel Index), physical condition and mobility (Timed “Up & Go” [TUG]), frailty level (Clinical Frailty Scale [CFS]), cognition (Mini-Cog or Mini-Mental State Examination [MMSE]), nutritional status (NRS-2002), psychological health (Geriatric Depression Scale [GDS]-4) and social situation (type of housing, social contacts, level of dependency on others, possible support from family members or other persons, etc.).11–17 The TUG score was not assessed if there was no clinical suspicion of impaired physical condition.
The second part involved medical evaluation by an oncologist and a geriatrician. The physicians issued recommendations with respect to scheduled therapy based on a variety of factors, including the results of the first CGA part, the oncological diagnosis and its stage, the therapy previously recommended by the tumor board, including an evaluation of the related risks, the comorbidities including their quantification using the Charlson Comorbidity Index (CCI)18 and the medications taken (see Supplementary Table 1 at https://onco-hema.healthbooktimes.org for a comprehensive list of the evaluated parameters).
Based on the CGA results, the physicians issued recommendations regarding the scheduled therapy. For the purposes of this study, “modification of therapy” was defined as any change to the treatment recommendation originally issued by the tumor board. Specific modifications included dose adjustment, optimization of co-medication, nutrition support and pre-rehabilitation.
All data were entered into the PRO-PAC registry, which was built using Research Electronic Data Capture (REDCap) tools hosted at the KSBL. REDCap is a secure, web-based software platform designed to support data capture for research studies, providing 1) an intuitive interface for validated data capture; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for data integration and interoperability with external sources.19,20
Results
In order to determine the feasibility of the concept and analyze the baseline characteristics of the enrolled patient population, we decided to withhold new registry entries after nine months (September 2024). The patients were followed up until March 02, 2025.
Patients aged ≥70 years with solid tumors underwent G8 screening at the first or second consultation. Among 43 screened patients, approximately 40% had a G8 score ≤14 out of 17 points. In total, 17 patients were enrolled in the feasibility phase. Among them, 58.8% were female and the mean age of the cohort was 79.4 ± 6.2 years (range, 61.8–87.2). In the majority of cases (12 patients, 70.6%), the patients were referred to the service based on a combination of age over 70 years and G-8 score of ≤14. One patient who appeared very frail despite being 61.8 years old was referred based on a pathologic G-8 score alone (11/17); the remaining four cases were direct internal referrals of frail-appearing patients aged ≥70 years. All patients were referred because of a solid tumor, with colorectal cancer being the most common diagnosis (three patients, 17.6%), followed by pancreatic cancer (two patients, 11.8%). All other diagnoses occurred once each. The majority of patients (16 patients, 94.1%) presented with locally advanced or metastatic disease, the sole exception being localized melanoma of the vaginal introitus.
Regarding symptom burden, the most common complaints were weight loss and reduced mobility, each reported by seven patients (41.2%), followed by pain (five patients, 29.4%), insomnia and impaired appetite (four patients each, 23.6%). Four patients reported no complaints. The patients were also highly polymorbid,21 with a mean CCI of 8.8. The most frequent comorbidity was hypertension (13 patients, 76.5%), followed by chronic kidney disease (nine patients, 52.9%) and arrhythmia (five patients, 29.4%). Only one patient presented with arterial hypertension as the sole comorbidity.
Consistent with these findings, the rate of polypharmacy (≥5 medications22) was also elevated (12 patients, 70.6%), with an average of 7.2 medications taken daily (range, 0–14; SD, 4.4). Angiotensin II receptor blockers were the most prevalent drug class (eight patients, 47.1%), followed by statins and beta-blockers (seven patients each, 41.2%), pain killers and diuretics (five patients each, 29.4%). One patient (5.9%) was not taking any medication at the time of assessment. In terms of functional status, the population presented with a significant handicap in the activities of daily living, with a mean Barthel Index of 57.3.23 Despite this, acceptable mobility was maintained, with a mean TUG of 13.4 seconds, and the proportion of patients with cognitive impairment was notably low (two patients, 12.5%). Screening for depression was positive in two patients (12.5%) and 12 patients (75%) were at risk of malnutrition. Regarding the planned treatment, 11 patients (64.7%) were scheduled to receive chemotherapy, while immunotherapy and targeted therapy were each planned for four patients (23.6%) and hormonal therapy for three patients (17.6%). A curative approach was intended in only two individuals (11.8 %), reflecting the advanced disease state in this cohort.
Based on the CGA results, recommendations to modify the scheduled therapy were issued in most cases (10 patients, 58.8%), the most common being optimization of co-medication (seven cases, 41.2%) and nutrition support (five cases, 29.4%), as well as dose adjustment and pre-rehabilitation (three cases each, 17.6%).
The therapies ultimately administered were chemotherapy (eight patients, 47.1%), immunotherapy (five patients, 29.4%), surgery (four patients, 23.6%), radiotherapy and hormonal therapy (three patients each, 17.6%). In one case (5.9%), involving the patient with vaginal melanoma, no oncological therapy was administered, in accordance with both the tumor board and the CGA recommendations.
Regarding patient outcomes, disease progression was observed in six cases (35.3%), whereas death, stable disease and partial remission were each registered in one case (5.9%). Notably, no deaths occurred during the course of oncological therapy. The single death was reported in a patient who was already preterminal at the time of CGA and was scheduled for best supportive care by both the tumor board and CGA. At the data cut-off, eight patients were still receiving therapy. For an overview of the collected data, see Supplementary Table 1 (https://onco-hema.healthbooktimes.org).
From an organizational perspective, additional personnel resources were necessary. The CGA required approximately 30–45 minutes of nursing time per patient, corresponding to approximately 10% of a full-time equivalent (FTE) per week for a geriatric oncology nurse under our implementation conditions. In addition, physicians spent approximately 15 minutes per patient per week reviewing and integrating the CGA findings into clinical decision-making. The service also resulted in a slight increase in workload for administrative personnel. Nevertheless, it could still be incorporated into the center’s routine workflow without major issues, and no service-related incidents were observed.
Discussion
The geriatric oncology service and prospective data collection in the PRO-PAC registry were successfully established at our hospital. All tasks required for the proper functioning of this service were seamlessly integrated into the center’s regular operations. The selection and recruitment of patients, their evaluation using CGA and the final issuing of recommendations now occur in a standardized, safe manner and without presenting a challenge to the center’s budget and/or other duties. Correspondingly, based on the general impression of the investigators, the service is highly valued by patients, families and collaborating clinicians.
Since the service was completely new to our hospital, it underwent certain developments during the feasibility phase. This was particularly notable in the case of cognitive status evaluation, where the initial plan was to evaluate all patients using the MMSE; however, this proved to be unnecessary laborious in this population with infrequent cognitive impairment. Therefore, we switched to an evaluation using the Mini-Cog and reserved the MMSE for cases with a high clinical suspicion of impaired cognitive function. Consequently, we have a Mini-Cog record for some patients and an MMSE record for others, which unfortunately makes comparisons more difficult. It should also be mentioned that, while the threshold for Mini-Cog is given (<3 points indicate cognitive impairment), we had to agree on an adequate cut-off value for the MMSE. Finally, we decided to use a threshold of ≤26, a value well supported by evidence, especially in our target age group.24 Similarly, a cut-off point of ≥13.5 seconds in the TUG was chosen to identify impaired mobility.25 At this point, it should be stressed again that the TUG was not performed in patients without a suspicion of mobility impairment. While this measure was intended to avoid unnecessary testing, it unfortunately introduces an additional difficulty with regard to standardization and reproducibility.
The CGA workflow also evolved throughout the course of the feasibility phase. Originally, the nursing assessment was directly followed by simultaneous medical evaluation by the oncologist and geriatrician and all professionals discussed their results afterwards in an interdisciplinary conference. Over time, we changed this scheme so that the nurse discussed the results of the assessments with the physicians prior to the medical evaluation. This structural re-sequencing allowed the physicians to enter the evaluation with a better understanding of the patient’s situation, enabling them to ask more specific questions or perform additional tailored examinations, which, in turn, allowed the team to issue even more personalized recommendations. Theoretically, this sequence could introduce a risk of confirmation bias, as the physician might be inadvertently influenced by the nurse’s preliminary findings. However, in the context of an established interprofessional CGA team, this influence is not viewed as bias per se but rather as an intended and valuable information flow. Clinicians remain aware of this potential and use the nurse’s input to generate targeted hypotheses, thereby preserving the benefits of collaborative assessment.
Another aspect to discuss is that, due to the nature of the CCI, patients with tumors in general almost inevitably reach high comorbidity scores, which may make the disease burden of our patients appear high even though several individuals presented with a relatively low absolute number of diseases. Nevertheless, since a score of ≥7 predicts a 0% survival rate in the next 10 years, we apparently work with a population with a low life expectancy. This should be borne in mind when deciding on future therapy (especially when considering chemotherapy), since treatment approaches avoiding chemotherapy may be more beneficial for such individuals.26 It is also important to point out that even after CGA, the administered therapy could have been modified, which was indeed the case in the majority of our patients (nine individuals, 52.9%). However, it should be noted that the high number of patients with advanced disease in this cohort was not an intentional selection criterion but rather a consequence of the small sample size. Consequently, these findings should not be taken to imply that CGA is relevant only to palliative populations; on the contrary, they underscore the need to evaluate its utility in curative settings as well.
In terms of the baseline characteristics of the studied population, we can conclude that despite some heterogeneity in several aspects (notably age, symptoms, comorbidities and medications), we recruited a population of generally older and polymorbid oncologic patients suffering from polypharmacy and functional disabilities, thus corresponding well to our targeted group. It should be noted that the inclusion of a 61.8-year-old patient represents a deviation from our study protocol and further increases the heterogeneity.
Due to the lack of a control group, small sample size and variability of the situation after “intervention” (CGA) among other factors, the present study cannot make any specific statements, e.g. on survival outcomes and quality of life, which, importantly, was not the aim of the feasibility phase. Furthermore, no conclusions can be made about the effect of CGA on patients with hematologic malignancies, since at the current stage, patients with hematologic malignancies have been excluded from the registry. However, we plan to include these patients at a later time point as the registry matures and data collection processes are further standardized. This expansion will enable more comprehensive subgroup analyses and enhance the overall scientific value of the registry allowing it to generate more granular, diagnosis-specific insights into treatment adaptations in geriatric oncology.
Despite this limitation, our preliminary results suggest that CGA may help avoid unnecessary and potentially harmful treatments (such as chemotherapy) in patients who are unlikely to benefit from them. As such, and taking into account that CGA represents an additional, thorough evaluation of this vulnerable patient group prior to the initiation of potentially harmful therapeutic modalities, the service appears to be generally beneficial for the involved patients.
With respect to the collection of data in the PRO-PAC registry, our database built on the REDCap platform proved user-friendly and effective for this task, allowing us to register patients’ data easily. In particular, the cloud-based nature of this tool made record sharing very efficient.
In terms of approximate personnel requirements, we acknowledge that our estimates mentioned above are based on our local workflow and may vary depending on institutional structures and experience. Nevertheless, we believe that they provide a useful reference point for planning and resource allocation in similar settings.
Conclusions
We successfully implemented a geriatric oncology service in the oncology department of a medium-sized Swiss regional hospital using the CGA as the evaluation approach.
The service has been effective in enrolling individuals from the target group and, insofar as can be assessed in this small and heterogeneous initial patient cohort, appears to provide additional benefit.
We also established a mechanism for collecting and storing data from CGA evaluations through the PRO-PAC registry built on an online database. As the service continues, more data will be gathered in the registry, enabling more complex analyses, including detailed studies of the service’s benefits, to better inform therapeutic decision-making for geriatric oncology patients.
Ethics approval
This study was approved by the Ethics Committee of Northwest and Central Switzerland under the project ID 2025-01070.
Consent for publication
General written informed consent was obtained from the patients for the publication of this study.
Availability of data and materials
All patient data that support the current study are included in an anonymized form in the published article.
Conflict of interest
Marcus Vetter received honoraria for consultancy from GSK, Roche, Novartis, Exact Sciences, Pfizer, Stemline, AbbVie and ASC Oncology. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way. The other authors declared that the manuscript was written in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The study was entirely funded from the internal research budget of the KSBL.
Author contributions
M.S. and E.D.C. designed the study and were responsible for trial registration and the Ethics committee application. A.E. conducted the nursing part of CGA. D.W., H.U. and M.V. conducted the medical part. D.H. analyzed the data and wrote the manuscript under the supervision of D.W. and M.V. All authors read and approved the final manuscript.
AI use
The authors declared that no generative artificial intelligence (AI) or AI-assisted technologies were used in the preparation or writing of this manuscript. All content was produced entirely by the authors who take full responsibility for the accuracy, integrity and originality of the work.