
Current treatment landscape and unmet needs in HER2-positive metastatic breast cancer
The recognition of human epidermal growth factor receptor 2 (HER2) as an actionable oncogenic driver has revolutionized the management of breast cancer, with targeted therapies significantly improving clinical outcomes.1–3 HER2 overexpression is present in approximately 20% of metastatic breast cancers and is associated with aggressive disease biology and historically poor prognosis. Among patients with distant disease, the 5-year relative survival rates are 46.7% in HR-positive, HER2-positive subtype and 40.8% in the HR-negative, HER2-positive subtype.4 Over a decade ago, the phase III CLEOPATRA trial established taxane-based chemotherapy combined with dual HER2 blockade with trastuzumab and pertuzumab (THP) as the standard of care (SoC) for the first-line treatment of metastatic HER2-positive breast cancer, regardless of hormone receptor (HR) status.5 In this study, THP reduced the risk of death by 32% compared with trastuzumab and docetaxel alone (HR: 0.68 [95% CI: 0.56–0.84]; p<0.001), extending the median overall survival (OS) to nearly five years (56.6 months vs 40.8 months). Biomarker analyses further showed that patients carrying wild-type PIK3CA had a better prognosis than those with mutant PIK3CA.6 Median PFS was longer for patients whose tumors expressed wild-type versus mutated PIK3CA in both the control (13.8 months vs 8.6 months) and pertuzumab groups (21.8 months vs 12.5 months).
Docetaxel is recommended for at least six cycles, followed by trastuzumab–pertuzumab maintenance until disease progression, which could be combined with endocrine therapy (ET) in patients with HR-positive tumors.2 In Switzerland, taxane-based chemotherapy is generally administered for six to eight cycles to reduce toxicities and preserve quality of life (QoL), with patients transitioned to standard maintenance ideally upon “best response” plateau on imaging.
In the second line, the HER2-directed antibody–drug conjugate (ADC) trastuzumab deruxtecan (T-DXd) is the gold standard based on results from the phase III DESTINY-Breast03 trial.2,3 In this study, T-DXd showed superiority over first-in-class trastuzumab emtansine (T-DM1), with long-term data revealing a substantial clinical benefit in both progression-free survival (PFS) (median, 29.0 months vs 7.2 months) and OS (52.6 months vs 42.7 months).7–10 The impressive efficacy of T-DXd has prompted its evaluation earlier in the treatment paradigm, both in first-line (DESTINY-Breast0911) and curative-intent settings (DESTINY-Breast05,12,13 DESTINY-Breast1114), with recent positive results supporting the redefinition of current therapeutic pathways. T-DXd is also recommended for patients with active brain metastases following progression, where local intervention is not indicated.2,3 In patients with previously treated HER2-positive disease and either stable or active brain metastases, DESTINY-Breast12 demonstrated high T-DXd activity in the central nervous system (CNS), with 1-year PFS and CNS-PFS rates of 61.6% and 58.9%, respectively.15 The combination of the HER2 tyrosine kinase inhibitor (TKI) tucatinib with trastuzumab and capecitabine represents an alternative to T-DXd in this setting based on results from the phase II HER2CLIMB study.2,3 Among the 291 patients with brain metastases, the addition of tucatinib resulted in a 68% reduction in the risk of intracranial progression or death compared with trastuzumab and capecitabine alone (HR: 0.32 [95% CI: 0.22–0.48]; p<0.0001), with a 1-year CNS-PFS rate of 40.2%.16
Despite these successes, an important clinical gap remains. In the final analysis of CLEOPATRA, the OS rates with THP were 49% at five years and 37% at eight years, underscoring a considerable unmet clinical need.17 Emerging real-world data show that approximately 30% of patients never receive second-line therapy. However, prospective data are lacking, and attrition is likely influenced by difference in healthcare systems, access to anti-HER2 therapies and institutional treatment practices across countries. Furthermore, as-yet-unidentified factors may also contribute to attrition rates.18,19 A high attrition rate is particularly relevant given the availability of highly active post-progression therapies and emphasizes the need to improve upfront strategies.
Although their demonstrated clinical activity in HER2-positive metastatic breast cancer, resistance to HER2-targeted therapies remains common.20,21 Resistance to HER2-targeted therapy is biologically heterogeneous and may be de novo or acquired under therapeutic pressure, particularly in the metastatic setting. A key mechanism involves constitutive activation of the PI3K pathway, most frequently driven by PIK3CA mutations, PTEN loss or ERBB3 alterations, which can attenuate sensitivity to anti-HER2 therapies by maintaining downstream signaling independent of HER2 blockade.22,23 In addition, dysregulation of cell cycle control has been implicated in resistance biology, including genomic alterations affecting p27, cyclin E and the cyclin D/CDK4/6 axis. Importantly, these molecular alterations are not binary predictors of treatment response and do not fully explain resistance in most patients. Other contributing mechanisms include HER2 heterogeneity, activation of compensatory receptor tyrosine kinases and adaptive signaling rewiring under treatment pressure.21
Patients with HER2-positive metastatic breast cancer may present with either de novo stage IV disease or metachronous/recurrent metastases after prior treatment for early breast cancer. Compared with de novo presentation, recurrent disease is characterized by distinct clinical features and treatment patterns and is associated with less favorable outcomes. Reported proportions of de novo versus recurrent/metachronous presentation vary across studies: recurrent disease was more frequent in the PANHER study (62.5% vs 37.5%),24 while the SystHERs registry reported an almost equal distribution (49.8% de novo vs 50.2% recurrent metastases),25 and a more recent analysis found de novo metastases to be more common (60.9% vs 39.1%).18 In the SystHERs cohort, patients with recurrent disease were less likely to receive first-line THP than those with de novo disease (59.8% vs 73.3%) and had a shorter median PFS (11.9 months vs 17.7 months; HR: 0.69 [95% CI: 0.59–0.80]; p<0.0001).25 In comparison to clinical practice, almost all trials in the first-line setting across all biological subtypes include a higher number of patients with de novo disease.
This article reviews the persistent unmet medical needs in metastatic HER2-positive breast cancer, drawing on real-world insights into treatment patterns and sequencing, and outlines emerging data in the first-line setting.11,18,19,26,27 Together, the results highlight the importance of ensuring timely access to effective therapies to improve patient outcomes.
First-to-second-line attrition in routine clinical practice
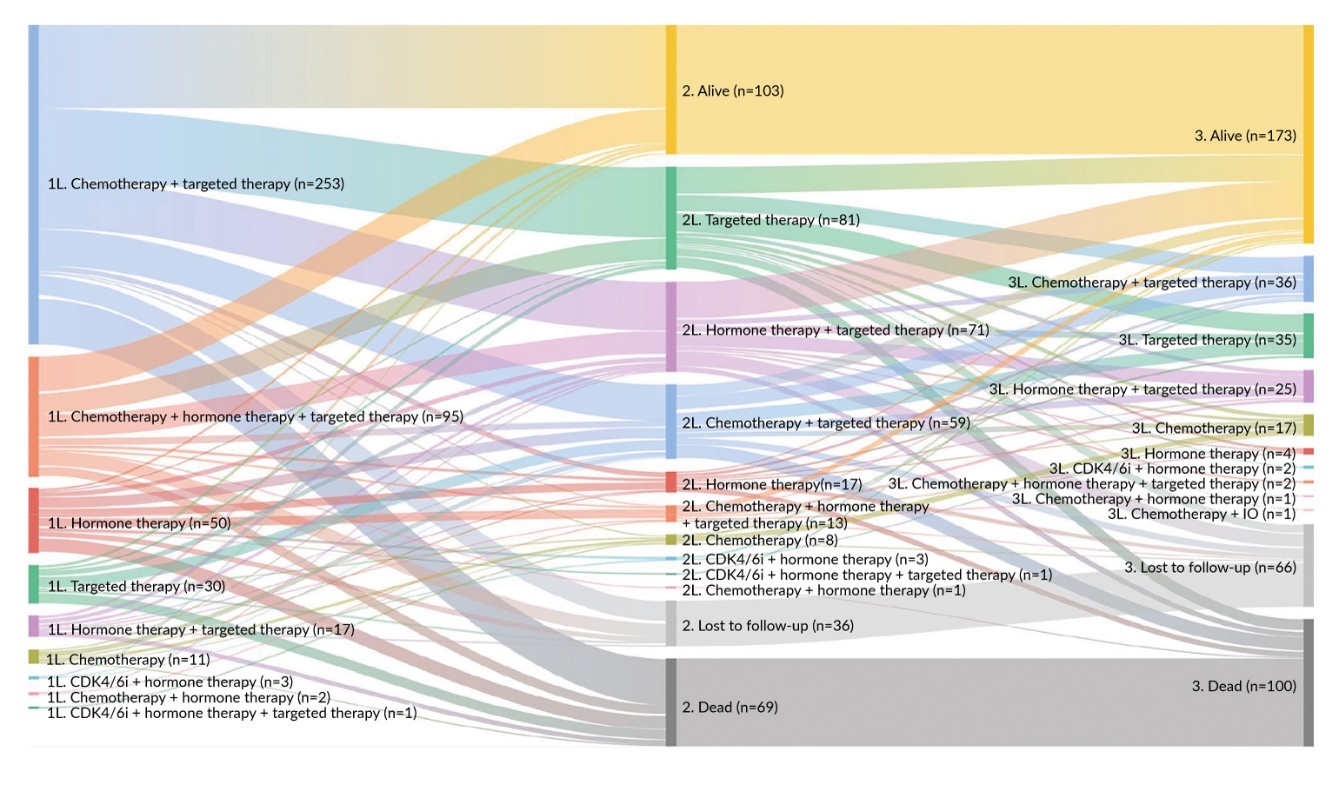
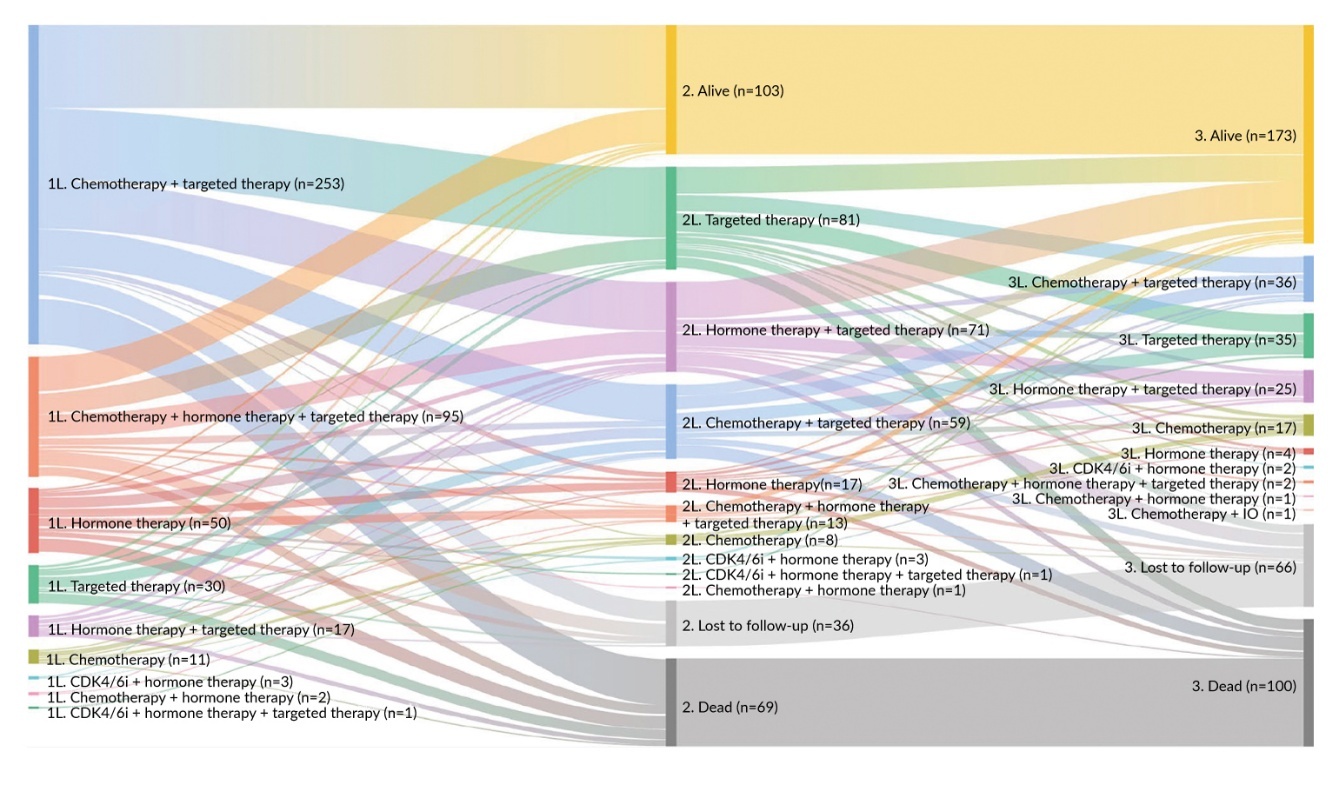
In a rapidly evolving therapeutic landscape, where novel agents are evaluated within specific therapy lines and may have overlapping indications, optimal treatment sequencing becomes challenging. A better understanding of real-world treatment patterns may help guide clinical decision-making to maximize the benefits of new therapies. A key factor influencing outcomes and complicating the evaluation of treatment effectiveness across successive therapy lines is patient attrition, which can result from non-adherence, treatment-related adverse events (TRAEs), disease progression or death. A recent retrospective study explored attrition rates in patients diagnosed with HER2-positive metastatic breast cancer between 2017 and 2021, leveraging electronic medical record data from seven hospital groups across France, Germany, Italy, Spain, and the UK.18 Attrition was defined as the proportion of patients who received one line of therapy (LOT) and showed no evidence of subsequent treatment, with the LOT algorithm aligned with the ESMO guidelines and standardized across centers. A total of 496 women were included in the analysis, with 60.9% of patients having stage IV disease at initial diagnosis. Among the 462 patients who had received at least one therapy for metastatic disease, 54.8% were treated with frontline HER2-directed therapy combined with chemotherapy (Figure 1). The median duration of first-line treatment was 8.0 months and the median PFS was 18.9 months, consistent with findings from the CLEOPATRA trial (18.7 months).5 Notably, nearly a third of patients (29.6%) failed to receive second-line therapy, with death accounting for the largest proportion of attrition (37.4%; “other” reasons, 29.9%; end-of-life palliative care, 15.0%; loss to follow-up, 14.0%).
Another retrospective study based on the Southeast Netherlands Advanced Breast Cancer (SONABRE) registry evaluated outcomes in 330 patients diagnosed with HER2-positive disease between 2013 and 2018.28 In the first-line setting, THP was administered to 29% of HR-positive (59/101) and 73% of HR-negative patients (64/88). The respective median OS in these subgroups was not reached at 56.0 months of follow-up and 48.4 months, reflecting outcomes reported in CLEOPATRA. In this analysis, the estimated continuation rate to second-line therapy was 61–80%, depending on HR status.
A similar analysis from the United States Flatiron Health database included 2,074 patients with HER2-positive metastatic breast cancer who received first-line systemic therapy from January 2013 to January 2021.29 In the first line, 77.5% of patients received trastuzumab-based therapy, with THP being the most common regimen (38.9%). At a median follow-up of 26.0 months from first-line initiation, 55.9% of patients had received subsequent therapy and 18.1% remained on treatment, whereas 20.2% died and 5.8% discontinued treatment without transitioning to next LOT. The median real-world PFS from the start of frontline therapy was 11.5 months and the median OS was 40.3 months. Notably, the most common second-line therapy was T-DM1, not reflecting current clinical practice. Taken together, over half of the patients progressed within one year of initiating first-line treatment, while approximately one-quarter did not proceed to second-line therapy.
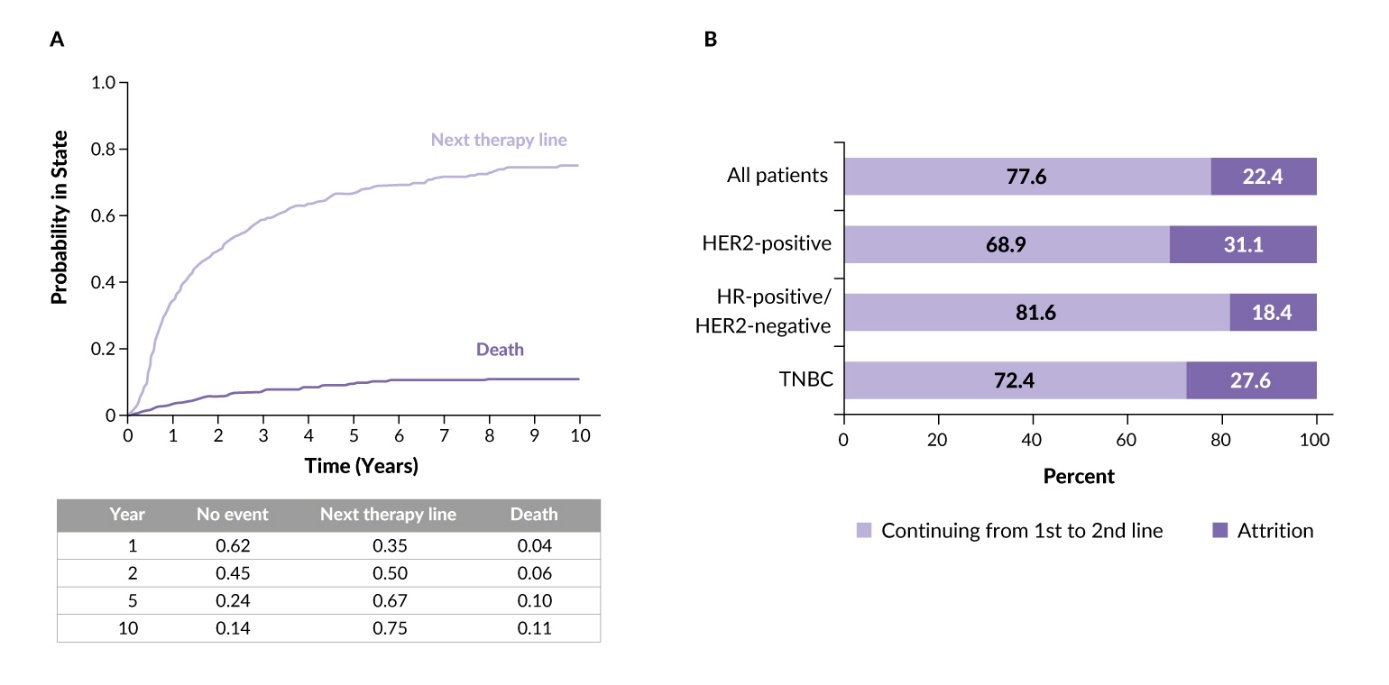
Comparable outcomes were reported from the prospective German PRAEGNANT registry.19 A total of 5,012 patients enrolled from 2012 to 2022 were analyzed to assess attrition rates across the first three therapy lines in advanced breast cancer. Among HER2-positive patients initiating first-line therapy (n=879), pertuzumab plus trastuzumab was the most frequently used regimen (57.8%). In HER2-positive disease, the probability of proceeding to second-line therapy within five years was 0.67 and the attrition rate was 31.3%, the highest observed among breast cancer subtypes (Figure 2).
_for_patients_receiving_first-line_therapy_t.jpeg)
Finally, an ongoing ambispective observational Italian study conducted between January 2000 and December 2021 in patients with metastatic breast cancer receiving first-line therapy reported substantially lower attrition rates.30 Here, attrition was defined as failure to initiate second-line treatment and death within six months of completing first-line therapy, which affects the comparability of the results. Among HER2-positive patients (n=622), 38.4% received THP and the attrition rate was 7.1%.
These findings highlight the importance of assessing real-world treatment outcomes, ideally through multi-country studies to ensure greater consistency and interpretability of the data. Importantly, the high first-to-second-line attrition of approximately 30% reported across most studies emphasizes the ongoing need to improve current therapeutic strategies in the first-line HER2-positive metastatic breast cancer.
Mechanisms of HER2-targeted resistance
Resistance to anti-HER2 therapies may arise through various mechanisms.1 HER2-activating mutations such as L755S and generation of truncated (p95HER2) or splice variants (Δ16HER2) can sustain downstream signaling and confer resistance to trastuzumab, which might be overcome with second-generation TKIs (neratinib, afatinib). Acquired resistance to tucatinib, which is highly selective for HER2 but spares epidermal growth factor receptor (EGFR), often involves EGFR amplification, which can be mitigated by pan-HER TKIs (neratinib, pyrotinib or poziotinib).31,32 PIK3CA mutations are also well-recognized mechanism of resistance to HER2-targeted therapies, including tucatinib, in HER2-positive breast cancer.22 Dual blockade with phosphatidylinositol 3-kinase (PI3K) inhibitors may be another effective approach in tumors harboring PIK3CA mutations or co-occurring HER3 mutations, which result in enhanced PI3K-AKT signalling.1,33 Activation of other compensatory pathways, including the ER signaling pathway and the cyclin D1–cyclin-dependent kinase 4 and 6 (CDK4/6) axis, has been demonstrated to drive resistance in preclinical studies.34,35 Immune-mediated mechanisms such as impaired antibody-dependent cell-mediated cytotoxicity (ADCC) may further limit efficacy and combining HER2-targeted therapy with CD47 blockade (magrolimab) to enhance macrophage activity has shown encouraging results.36 Finally, incomplete HER2 inhibition with monoclonal antibodies or HER2 tumor heterogeneity may be addressed with ADCs carrying potent payloads such as T-DXd, which show activity in tumors with low or ultra-low levels of HER2 expression.37,38
Overall, integrating ADCs, TKIs, CDK4/6 inhibitors and immunomodulatory strategies offers a path to overcome multiple mechanisms of HER2-targeted therapy resistance.
Towards a new first-line standard
DESTINY-Breast09: Frontline trastuzumab deruxtecan
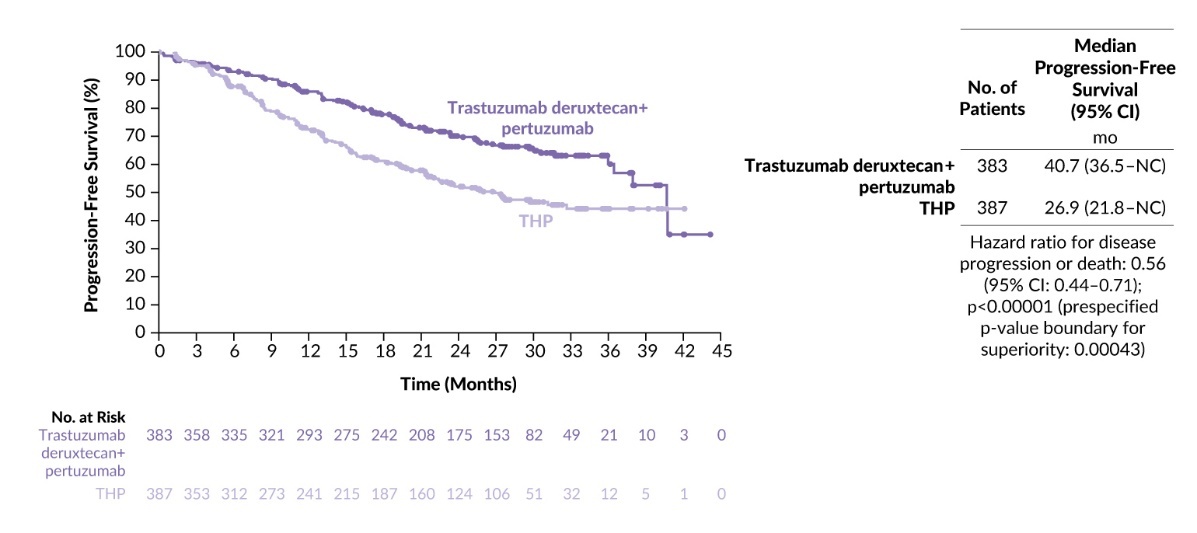
The phase III DESTINY-Breast09 trial evaluated the efficacy and safety of first-line T-DXd regimens for HER2-positive advanced or metastatic breast cancer.11 Patients who had not received previous chemotherapy or anti-HER2 therapy for metastatic disease were randomized in a 1:1:1 ratio to receive T-DXd plus pertuzumab (n=383), T-DXd plus placebo (n=387) or THP (n=387). Patients with HR-positive disease could receive concurrent ET after discontinuing taxane or completing six cycles of T-DXd. The primary endpoint was PFS by blinded independent central review. Patients were stratified according to newly diagnosed or recurrent disease, HR status and the presence or absence of PIK3CA mutation. Secondary outcomes included investigator-assessed PFS, OS, objective response rate (ORR), duration of response (DoR) and safety. Available data are from the prespecified interim analysis comparing the T-DXd plus pertuzumab with THP at a median follow-up of 29.2 months. Results for the T-DXd plus placebo arm remain blinded until the final PFS analysis.
The baseline characteristics were well-balanced between the T-DXd plus pertuzumab and THP arms.11 The median patient age was 54 years, roughly half of the study population had a newly diagnosed disease (52%) and HR-positive status (54%). Overall, 43.5% of patients received prior adjuvant or neoadjuvant therapy, including chemotherapy (40.4%) trastuzumab (28.3%), and pertuzumab (7.1%).
T-DXd plus pertuzumab resulted in a statistically significant and clinically meaningful reduction in the risk of progression or death of 44% compared with THP (HR: 0.56 [95% CI: 0.44–0.71]; p<0.00001), with a 2-year PFS rate of 70.1% versus 52.1%, respectively.11 The median PFS was 40.7 months with T-DXd plus pertuzumab versus 26.9 months with THP, corresponding to an absolute gain of over one year (Figure 3). This PFS benefit was consistent across most patient subgroups and was observed regardless of disease status at baseline (newly diagnosed, HR: 0.49 [95% CI: 0.35–0.70]; recurrent, HR: 0.63 [95% CI: 0.46–0.87]), PIK3CA mutation status (detected, HR: 0.52 [95% CI: 0.35–0.77]); not detected, HR: 0.57 (95% CI: 0.43–0.77) or previous exposure to anti-HER2 therapies (yes, HR: 0.55 [95% CI: 0.36–0.83]); no, HR: 0.56 (95% CI: 0.42–0.74). PFS favored T-DXd plus pertuzumab over THP in patients with HR-positive disease (HR: 0.61 [95% CI: 0.44–0.84]), despite nearly threefold higher use of concurrent ET in the THP arm (38.3% vs 13.5%); the hazard ratio in the HR-negative subgroup was 0.52 (95% CI: 0.37–0.73). Notably, patients with brain metastases also derived a PFS benefit (n=47; HR: 0.30 [95% CI: 0.12–0.68]), consistent with data from the phase IIIb/IV DESTINY-Breast12 trial.15
The ORR numerically favored T-DXd plus pertuzumab over THP (85.1% vs 78.6%; odds ratio: 1.59 [95% CI: 1.09–2.32]), with a median DoR of 39.2 months and 26.4 months, respectively.11 Complete responses (CR) were achieved by 15.1% of patients in the T-DXd combination arm versus 8.5% in the THP arm, corresponding to a nearly twofold increase with the T-DXd regimen. Time to second progression or death (PFS2) numerically favored T-DXd plus pertuzumab over THP (HR: 0.60 [95% CI: 0.45–0.79]), with the median not reached versus 36.5 months, respectively. Following discontinuation of study treatment, fewer patients received second-line therapy in the T-DXd plus pertuzumab arm than in the THP arm (32.4% vs 46.8%), with targeted therapy favored over chemotherapy in both groups. In the T-DXd combination arm, trastuzumab and/or pertuzumab-containing regimens predominated (34.2%) and 3.4% of patients received anti-HER2 ADC (T-DXd or T-DM1) in the second line. In the THP arm, 22.0% of patients received trastuzumab and/or pertuzumab-containing regimens, with 22.2% receiving an anti-HER2 ADC.
Overall safety was consistent with the established profiles of the individual agents, with no new safety signals identified.11 Treatment duration was longer in the T-DXd plus pertuzumab arm than in the THP arm, with a median of 21.7 months (T-DXd, 20.0 months) versus 16.9 months (taxane, 4.4–5.5 months). Despite this, the two groups had comparable incidences of grade ≥3 (54.9% vs 62.3%) and serious treatment-emergent adverse events (TEAEs) (27.0% vs 25.1%). The T-DXd combination regimen was more frequently associated with AEs leading to dose reductions (45.9% vs 19.9%) and interruptions (68.8% vs 49.0%), whereas treatment discontinuations were more common with THP (28.3% vs 20.7%). In terms of drug-related toxicity, patients who received T-DXd plus pertuzumab experienced nausea most often (71.1%) versus diarrhea with THP (54.2%). The most frequent grade ≥3 TRAE was neutropenia in both groups (23.9% vs 33.2%), followed by hypokalemia (10.2%) and anemia (8.4%) in the T-DXd plus pertuzumab arm and leukopenia (17.5%) and diarrhea (5.2%) in the THP arm (Table 1). Grade 5 TEAEs occurred in 3.4% of patients in the T-DXd plus pertuzumab arm and 0.8% of patients in the THP arm, with five and one deaths, respectively, considered treatment-related. In the T-DXd plus pertuzumab arm, treatment-related fatal events included pneumonitis as assessed by the investigator, sepsis, septic shock, febrile neutropenia and dyspnea (one case each). Accordingly, interstitial lung disease/pneumonitis remains an adverse event of clinical relevance, warranting appropriate patient monitoring. Adjudicated drug-related interstitial lung disease/pneumonitis occurred in 12.1% (n=46) of patients with T-DXd plus pertuzumab (grade ≤2, n=44; grade 5, n=2) and 1.0% (n=4) with THP (grade ≤2 in all patients).
QoL outcomes were broadly comparable between the treatment arms with respect to overall treatment tolerability, pain deterioration, and fatigue.39 T-DXd plus pertuzumab was associated with numerically higher rates of certain gastrointestinal symptoms than THP (nausea, vomiting, constipation, and appetite loss; diarrhea was unaffected), whereas arm- and other breast cancer-specific symptoms were less frequent.
Overall, these findings indicate a favorable benefit–risk profile for T-DXd plus pertuzumab in first-line HER2-positive advanced or metastatic breast cancer.10,40,41 Notably, this regimen does not require a taxane maintenance phase, as T-DXd has demonstrated sustained long-term tolerability across DESTINY-Breast01,40 DESTINY-Breast0241 and DESTINY-Breast0310 trials, enabling maintenance of maximal therapeutic activity, whereas taxanes are often limited by cumulative toxicity.42 At two years, over two-thirds of patients remained free of disease progression (70.1% vs 52.1% with THP), indicating a sustained benefit in the first-line setting.42 OS data remained immature, with approximately 16% maturity, but show a favorable trend (HR: 0.84 [95% CI: 0.59–1.19]).
In this context, a planned trial of the Swiss Cancer Institute (SCI) may provide an important future perspective. Patients who complete six cycles of T-DXd will be randomized to either continue T-DXd or switch to trastuzumab plus pertuzumab maintenance therapy.
PATINA: Adding palbociclib to first-line maintenance therapy
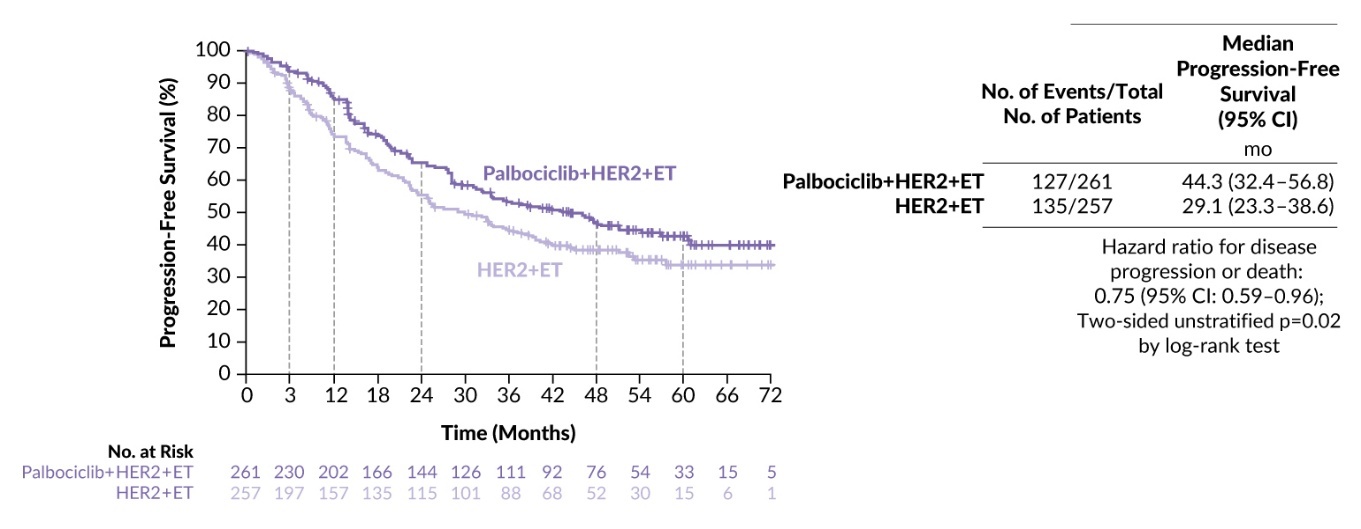
Given the practice-changing potential of T-DXd plus pertuzumab, the role of first-line maintenance is yet to be defined. Expanding the range of available therapies could, however, provide greater flexibility in long-term management and individual patient needs. Dual inhibition of HER2 and CDK4/6 has demonstrated synergistic effects on cell proliferation in preclinical models, with CDK4/6 blockade showing the potential to re-sensitize tumors to HER2-directed therapies.35 Based on this rationale, the phase III PATINA trial evaluated the value of incorporating palbociclib into first-line maintenance in patients with HR-positive, HER2-positive metastatic breast cancer.26
In this study, 518 patients with no evidence of disease progression after completing 6–8 cycles of induction therapy (including trastuzumab with or without pertuzumab and taxane/vinorelbine) were randomized 1:1 to receive either palbociclib combined with trastuzumab (with or without pertuzumab) and ET or maintenance alone; the non-pertuzumab regimen was permitted but restricted to up to 20% of the study population.26 Stratification factors included pertuzumab use (yes vs no), prior anti-HER2 therapy in the (neo)adjuvant setting (yes vs no), response to induction therapy by investigator assessment (CR or partial response [PR] vs stable disease [SD]) and type of endocrine therapy (fulvestrant vs aromatase inhibitor).
Baseline demographic and clinical characteristics were well balanced between the two treatment arms.26 The median age was approximately 53 years and patients received a median of six cycles of induction therapy. More than 97% of patients were treated with pertuzumab and 91% received an aromatase inhibitor as ET. Prior anti-HER2 therapy in the (neo)adjuvant setting was administered to 71% of patients.
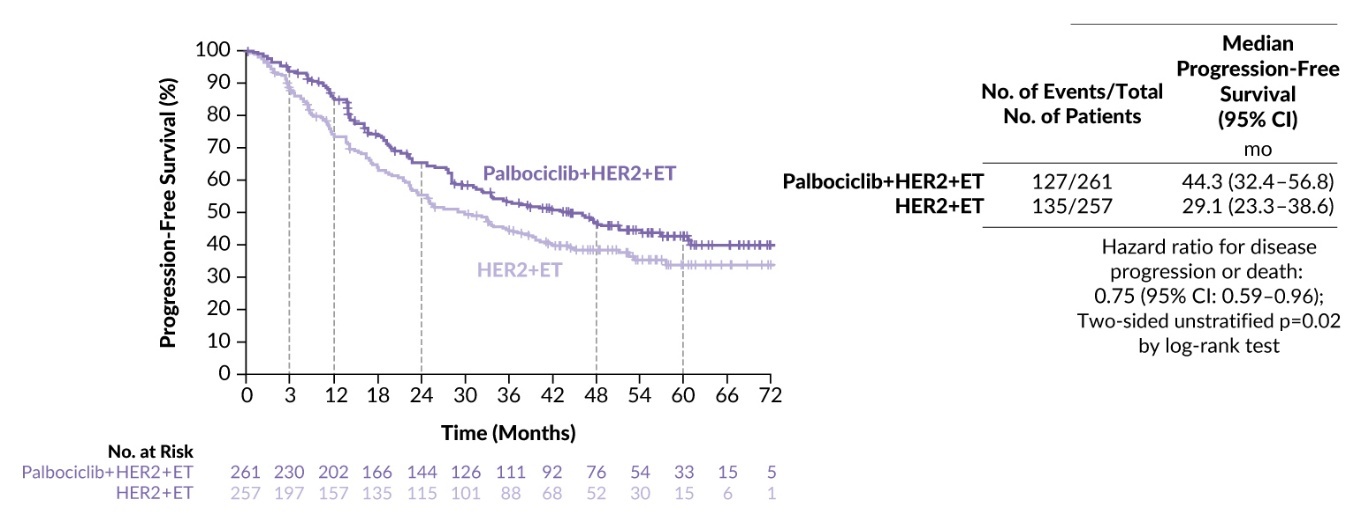
At a median follow-up of 53.5 months, palbociclib significantly delayed disease progression (HR: 0.75 [95% CI: 0.59–0.94]; p=0.02), corresponding to an absolute improvement in median PFS of 15.2 months (44.3 months vs 29.1 months) (Figure 4).26 The PFS benefit was consistent across prespecified subgroups, including prior anti-HER2 therapy (yes, HR: 0.76 [95% CI: 0.57–1.01]; no, HR: 0.68 [95% CI: 0.543–1.07]) and best response to induction (CR/PR, HR: 0.76 [95% CI: 0.57–1.02]; SD, HR: 0.72 [95% CI: 0.47–1.12]).
The addition of palbociclib also improved secondary endpoints, including ORR (29.9% vs 22.2%; p=0.046) and clinical benefit rate (89.3% vs 81.3%; p=0.01).26 At the interim analysis, median OS was not estimable in the palbociclib arm and was 77 months in the control arm (HR: 0.86 [95% CI: 0.60–1.24]), with 3-year OS rates of 87.0% versus 84.7% and 5-year OS rates of 74.3% versus 69.8%, respectively.
The safety profile of palbociclib plus anti-HER2 therapy and ET was manageable, with no new safety signals identified.26 The most frequent grade 3–4 AEs in the palbociclib-containing arm were neutropenia (67.8% vs 4.4% in the control arm), decreased white blood cell count (11.9% vs 0.0%) and diarrhea (11.1% vs 1.6%). The incidence of grade ≥4 AEs was similar across study arms (12.3% vs 8.9%; p=0.21). No treatment-related deaths were reported. Treatment discontinuation due to AEs were reported in 7.5% of patients in the palbociclib arm.
In conclusion, the addition of palbociclib to first-line therapy resulted in a clinically meaningful improvement in PFS with a manageable safety profile. These findings support the biological rationale of targeting CDK4/6i to overcome resistance to anti-HER2–based therapy.
HER2CLIMB-05: Adding tucatinib to the first-line maintenance therapy
More recently, the phase III HER2CLIMB-05 trial of tucatinib in addition to first-line maintenance therapy with trastuzumab plus pertuzumab reported positive outcomes regardless of HR status.27 Patients with stable disease after four to eight cycles of induction therapy with THP were randomly assigned at a 1:1 ratio to receive either tucatinib (n=326) or placebo (n=328) plus trastuzumab and pertuzumab with or without ET.
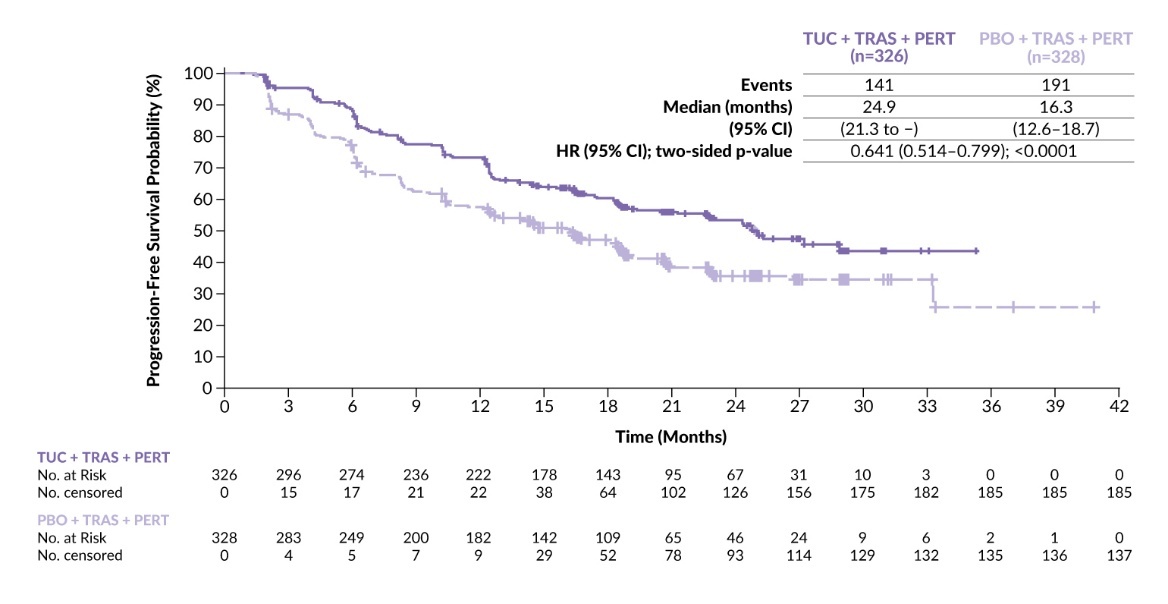
PFS favored the tucatinib regimen over SoC (HR: 0.64 [95% CI: 0.51–0.80]; p<0.0001), with a median PFS of 24.9 months versus 16.3 months, respectively (Figure 5).27 All prespecified patient subgroups demonstrated a consistent PFS benefit with tucatinib plus trastuzumab and pertuzumab, including those with HR-positive (median, 24.9 months vs 12.6 months; HR: 0.554) and HR-negative (median, 25.0 months vs 18.1 months; HR: 0.725) disease. Patients with baseline brain metastases derived a comparable PFS benefit (HR: 0.64), with a numerical improvement in CNS-PFS (median, 8.5 months vs 4.3 months; HR: 0.72 [95% CI: 0.41–1.27]).
_in_the_intention-to-tr.jpeg)
In the primary analysis, OS data were immature, with 20.2% of the required events observed.27 Median OS was not reached in either treatment arm (HR: 0.539 [95% CI: 0.303–0.957]). Overall, 35.0% of patients in the tucatinib arm and 54.3% of patients in the placebo arm received at least one subsequent anticancer therapy, most commonly an HER2 inhibitor (32.2% vs 47.6%), including T-DXd (16.3% vs 24.7%) and trastuzumab (12.3% vs 15.9%).
In terms of safety, the most frequent TEAEs in the tucatinib arm were diarrhea (72.7%), nausea (33.1%), elevated alanine aminotransferase (ALT) (28.2%), elevated aspartate aminotransferase (AST) (25.8%), arthralgia (20.6%) and fatigue (20.6%).27 In the control arm the most common TEAEs were diarrhea (51.2%), nausea (23.5%) and arthralgia (23.1%). Grade ≥3 TEAEs occurred in 42.3% of patients in the tucatinib arm and 24.4% of patients in the control arm. The most frequent grade ≥3 TEAEs with tucatinib were elevated ALT (13.5% vs 0.6% in control arm), elevated AST (7.1% vs 0.6%) and diarrhea (6.1% vs 4.0%).
Serious TEAEs were reported in 16.9% of patients in the tucatinib arm and 8.0% in the control arm.27 In the tucatinib arm, the most commonly reported serious TEAEs were elevated ALT (1.5% vs 0%) and drug-induced liver injury (1.2% vs 0%). TEAEs leading to treatment discontinuation occurred in 13.8% of patients receiving tucatinib and 4.6% of those receiving placebo.
In summary, the primary analysis of HER2CLIMB-05 demonstrated that adding tucatinib to trastuzumab and pertuzumab as first-line maintenance therapy significantly improved PFS in patients with HER2-positive metastatic breast cancer with no evidence of progression after completion of induction THP therapy, with PFS benefit sustained across all patient subgroups, regardless of the presence of baseline brain metastases or HR status.27
Conclusions
Despite major therapeutic advances, metastatic HER2-positive breast cancer remains an incurable disease and important unmet needs persist. Real-world evidence consistently shows that up to one-third of patients do not receive subsequent lines of therapy after first-line treatment due to disease progression, toxicity or clinical deterioration.18,19,29 This highlights the importance of optimizing early treatment strategies to achieve durable disease control while maintaining quality of life.
Recent phase III trials are expanding treatment options in the first-line setting. The DESTINY-Breast09 study demonstrated that T-DXd combined with pertuzumab can achieve prolonged disease control in the initial treatment of HER2-positive metastatic breast cancer.11 Importantly, as crossover to T-DXd was not mandated in the THP arm, it remains unclear whether sequential treatment with THP followed by T-DXd would achieve outcomes comparable to upfront T-DXd. Furthermore, the PATINA trial showed that incorporating CDK4/6 inhibition with palbociclib into anti-HER2 maintenance therapy can improve outcomes in patients HR-positive disease.26 The HER2CLIMB-05 study further supports the role of HER2-targeted tyrosine kinase inhibition, demonstrating clinical benefit when tucatinib is added to trastuzumab- and pertuzumab-based maintenance therapy.27 Although OS data are still immature, these three studies support a more individualized treatment approach based on patient and disease characteristics, including HR status and the presence or history of brain metastases.
Taken together, these studies highlight the rapid evolution of first-line management and expand the range of available strategies for patients with HER2-positive metastatic breast cancer.
Conflict of interest
Jens Huober received honoraria for lectures from Lilly, Novartis, Roche, Pfizer, AstraZeneca, MSD, Seagen, Gilead and Daiichi Sankyo; honoraria for consulting/advisory board from Lilly, Novartis, Roche, Pfizer, AstraZeneca, MSD, Daiichi Sankyo and Gilead; and travel grants from Roche, Pfizer, Daiichi Sankyo and Gilead. Marcus Vetter received honoraria for consultancy from GSK, Roche, Novartis, ExactSciences, Pfizer, Stemline, AbbVie and ASC Oncology. Christian Kurzeder reported honoraria from Tesaro, GSK, Astra Zeneca, Novartis, PharmaMar, Genomic Health, Roche, Eli Lilly S.A., Pfizer and Daichi; consulting or advisory role for Tesaro, GSK, Astra Zeneca, Novartis, PharmaMar, Genomic Health, Roche, Eli Lilly S.A., Merck MSD and Pfizer; and travel and accommodation expenses from GSK, Astra Zeneca and Roche. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way.
Funding
The preparation of this article was financially supported by AstraZeneca and Daiichi-Sankyo. These funding entities had no decision-making role in the development of the manuscript and did not influence its content in any way.
Authors contributions
The authors created and approved the final manuscript.
AI use
The authors declared that no generative artificial intelligence (AI) or AI-assisted technologies were used in the preparation of this manuscript. All content was produced entirely by the authors who take full responsibility for the accuracy, integrity and originality of the work.