
Genitourinary oncology is entering a new era of clinical care, marked by rapid therapeutic development, earlier use of systemic treatments and a growing focus on personalized treatment. Several studies presented at the recent major oncology congresses are expected to influence daily practice in prostate, bladder, kidney and germ cell cancers. This article summarizes the most relevant recent data with the potential to inform clinical practice in these malignancies.
Prostate cancer
The systemic treatment landscape in prostate cancer continues to evolve, with a shift toward earlier treatment intensification and more precise, biomarker-informed decision-making.1,2 While localized disease, depending on the risk, is still mainly treated with prostatectomy or radiotherapy with or without androgen-deprivation therapy (ADT) and/or androgen receptor pathway inhibitor (ARPI), systemic therapy is playing an increasingly important role, particularly in high-risk biochemical recurrence and metastatic hormone-sensitive prostate cancer (mHSPC).
EMBARK: Enzalutamide plus leuprolide significantly improves OS in high-risk biochemically recurrent prostate cancer
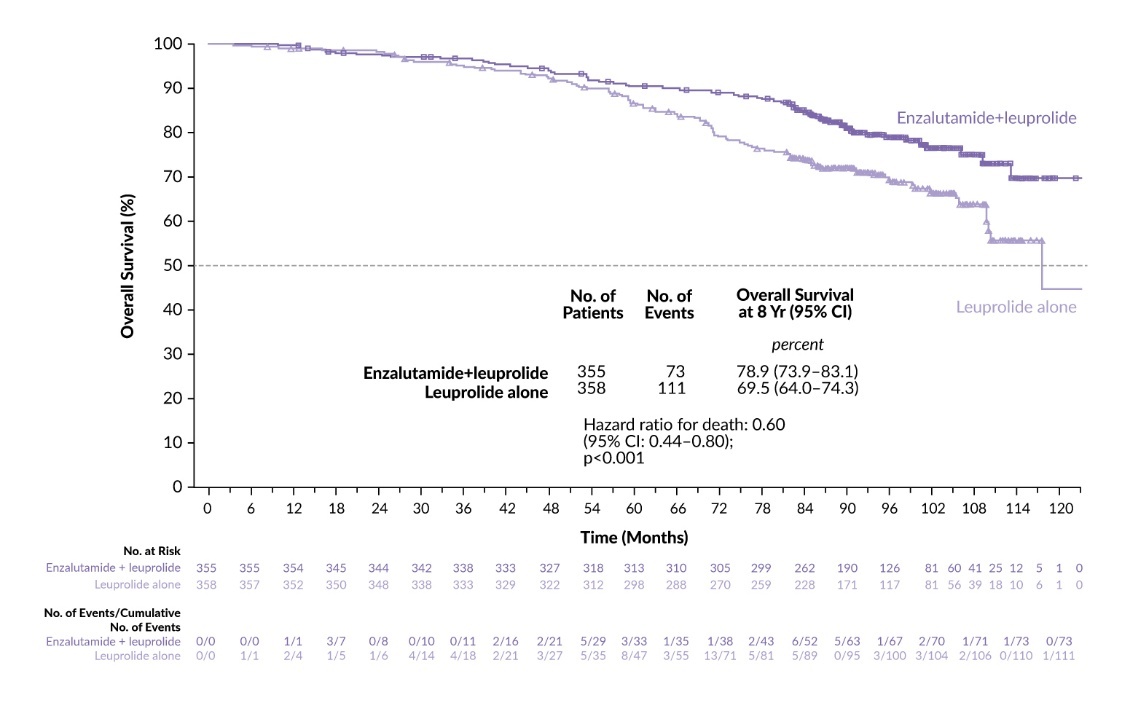
A major update in the high-risk biochemically recurrent setting came from the phase III EMBARK trial, which randomized 1,068 men with castration-sensitive biochemical recurrence and no metastases on conventional imaging to receive either enzalutamide plus leuprolide acetate, placebo plus leuprolide or enzalutamide monotherapy.3 Previously reported data showed significantly improved metastasis-free survival with both enzalutamide plus leuprolide (HR: 0.42 [95% CI: 0.30–0.61]; p<0.001) and enzalutamide monotherapy (HR: 0.63 [95% CI: 0.46–0.87]; p=0.005) compared with leuprolide alone.
With longer follow-up of approximately 94 months, EMBARK has demonstrated a statistically significant OS advantage for enzalutamide plus leuprolide.4,5 The 8-year OS rate was 78.9% with combination therapy versus 69.5% with leuprolide alone (HR: 0.60 [95% CI: 0.44–0.80]; p<0.001) (Figure 1), with benefit consistent across prespecified subgroups. Enzalutamide monotherapy achieved an 8-year OS rate of 73.1% (HR: 0.83 [95% CI: 0.63–1.10]; p=0.19), indicating a numerical improvement without statistical significance.
_with_enzalutamide_plus_leuprolide_versus_leuprolide_alone_in_the_emb.jpeg)
Beyond OS, the combination of enzalutamide and leuprolide also significantly improved secondary outcomes compared with leuprolide monotherapy, including time to first new antineoplastic therapy, time to prostate-specific antigen (PSA) progression, time to first symptomatic skeletal event and progression-free survival (PFS) on first subsequent therapy (PFS2).4,5 Similar benefits were observed with enzalutamide monotherapy compared with leuprolide alone. The trial was not powered to compare enzalutamide versus ADT plus enzalutamide; therefore, enzalutamide should be recommended in this indication combined with ADT.
A post hoc analysis further demonstrated that approximately one in 25 patients (4%) treated with enzalutamide plus leuprolide for nine months maintained a PSA <0.2 ng/mL alongside testosterone recovery (>250 ng/dL) three years after therapy.6 In comparison, this outcome was observed in only 1% of patients receiving leuprolide alone or enzalutamide monotherapy. These findings suggest that durable remissions may be achievable following a nine-month course of combination therapy.
Long-term safety outcomes remained consistent with prior reports, with grade ≥3 treatment-emergent adverse events (TEAEs) occurring in 52.4% of patients in the combination arm, 49.4% in the leuprolide monotherapy arm and 57.3% in the enzalutamide monotherapy arm.4,5 The incidence of serious TEAEs was under 10% in all groups, at 8.5% versus 2.5% and 7.6%, respectively.
The AMPLITUDE trial met its primary endpoint of improved radiographic PFS in patients with mHSPC
In mHSPC, systemic therapy has progressed from ADT alone to ADT-based doublets with ARPIs, such as abiraterone, enzalutamide, apalutamide and darolutamide, and further to triplets that also incorporate docetaxel.7–10 A key recent development is the emergence of biomarker-driven triplets, in which ADT plus an ARPI is combined with a targeted agent selected according to tumor biology. One such example is niraparib, a potent and selective PARP inhibitor that is currently indicated in combination with ADT and prednisone or prednisolone for the first-line treatment of asymptomatic or mildly symptomatic adult patients with metastatic castration-resistant prostate cancer (mCRPC) with BRCA gene alterations and without visceral metastases, in whom chemotherapy is not clinically indicated, based on the phase III MAGNITUDE trial.11 In the mHSPC setting, niraparib combined with abiraterone acetate plus prednisone (APP) was further assessed in patients with alterations in homologous recombination repair (HRR) genes in the phase III AMPLITUDE trial. Findings from this study were presented at the 2025 ASCO Annual Meeting and recently published.12,13
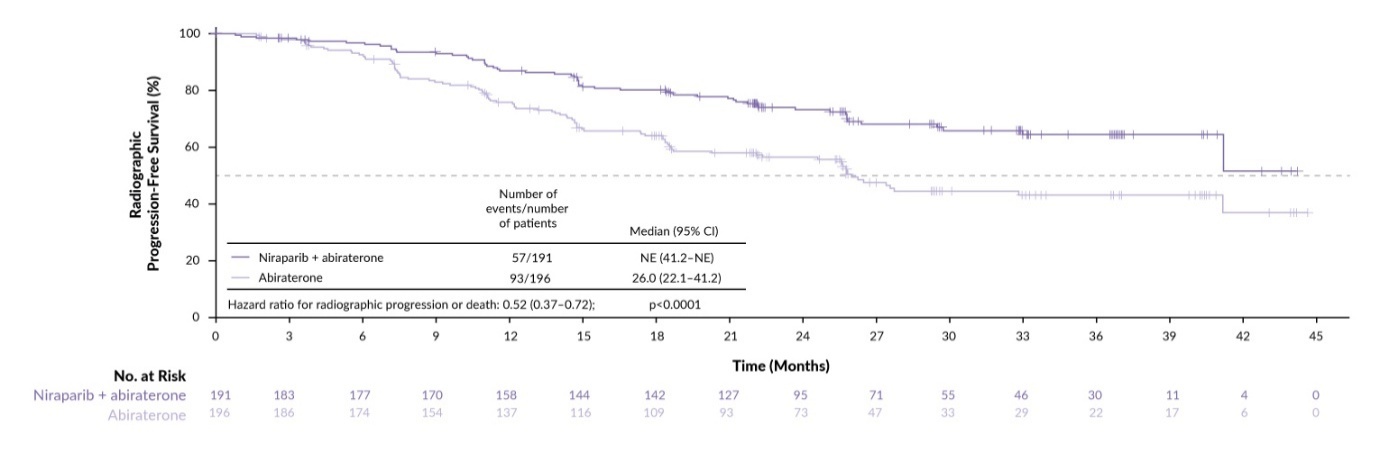
AMPLITUDE met its primary endpoint of radiographic PFS (rPFS), showing median rPFS of not estimable with niraparib versus 29.5 months with placebo in all randomized patients (HR: 0.63 [95% CI: 0.49–0.80]; p<0.0001) and not estimable versus 26.0 months in a subgroup of patients with BRCA1/2 alterations (BRCAm) (HR: 0.52 [95% CI: 0.37–0.72]; p<0.0001) (Figure 2).12,13 OS was not statically significant at this analysis, either in the overall study population (HR: 0.79 [95% CI: 0.59–1.04]; p=0.10) or the BRCAm group (HR: 0.75 [95% CI: 0.51–1.11]; p=0.15). However, the OS data were still immature, as fewer than 50% of the required events have occurred in either group. Further results showed that niraparib significantly reduced the risk of symptomatic progression by 50% in the broader study population (HR: 0.50 [95% CI: 0.36–0.69]; p<0.0001) and by 56% in the BRCAm group (HR: 0.44 [95% CI: 0.29–0.68]; p=0.0001).
Toxicity profile demonstrated known PARP inhibitor effects, with anemia reported in 52% (grade ≥3 in 29%) versus 24% (grade ≥3 in 5%) and hypertension in 45% versus 33% (grade ≥3 in 27% versus 18%) of patients in the niraparib versus placebo arms.12,13 Notably, despite early decline in quality-of-life measures, patient-reported outcomes suggested that overall health-related (HRQoL) was maintained without clinically meaningful long-term deterioration.14
CAPItello-281: Capivasertib combination prolongs rPFS in PTEN-deficient mHSPC
A biomarker-defined approach is also emerging for PTEN-deficient mHSPC, a subgroup in which AKT pathway activation is associated with poorer outcomes.15,16 Capivasertib is a potent selective inhibitor of all three AKT isoforms and has been investigated in the CAPItello-281 trial in patients with PTEN-deficient de novo mHSPC.17,18 In this phase III study, patients were randomized 1:1 to receive either capivasertib plus abiraterone or placebo plus abiraterone, both on an ADT backbone.
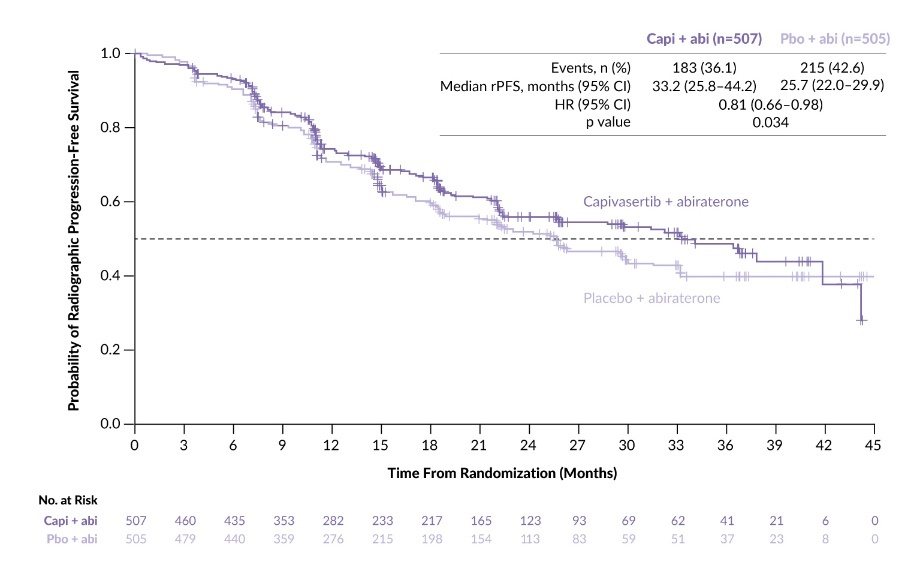
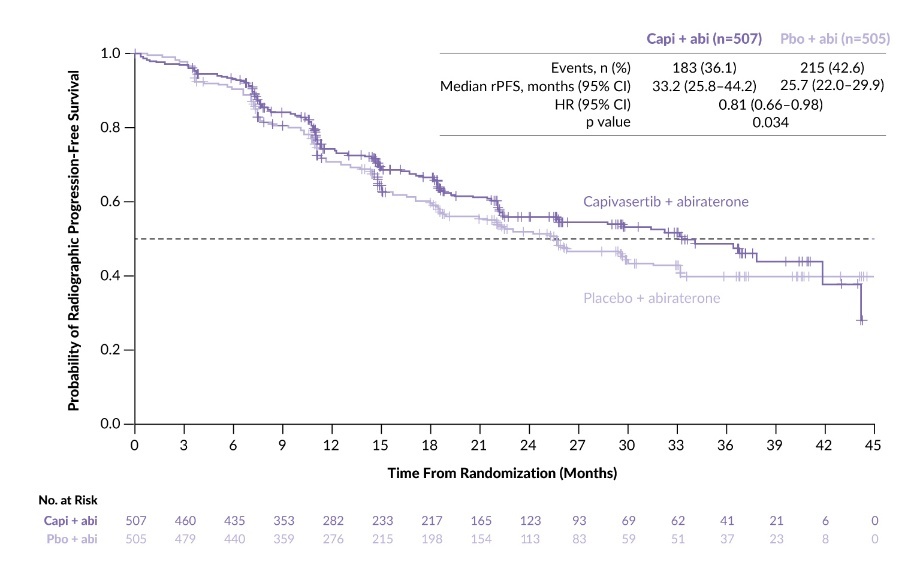
Primary analysis of the trial presented at the ESMO Congress 2025 by Prof. Karim Fizazi showed a statistically significant improvement in median rPFS to 33.2 months with capivasertib versus 25.7 months with placebo (HR: 0.81 [95% CI: 0.66–0.98]; p=0.034) (Figure 3), with consistency across most prespecified subgroups. OS did not reach statistical significance (HR: 0.90 [95% CI: 0.71–1.15]; p=0.401), with data remaining immature (26% maturity).17,18 Clinically relevant delays were observed in time to castration resistance, with a median of 29.5 months with capivasertib compared with 22.0 months with placebo (HR: 0.77 [95% CI: 0.63–0.94]; nominal p=0.009). Adding capivasertib to abiraterone plus ADT was also associated with numerical improvements in symptomatic skeletal event-free survival and time to PSA progression.
As expected for an AKT inhibitor regimen, toxicity was higher in the capivasertib arm compared with the placebo arm, with grade ≥3 AEs in 67% versus 40.4% of patients.17,18 The most common grade ≥3 events with capivasertib included rash (12.3%), hyperglycemia (10.3%) and hypokalemia (8.7%). AEs leading to capivasertib or placebo discontinuation occurred in 18.3% versus 4.8% of patients, respectively.
Patient-reported outcomes presented at the 2026 ASCO Genitourinary Cancers Symposium showed no clinically meaningful differences between treatment arms in least-squares mean change from baseline for the FACT-P total score or in the physical well-being and functional well-being subscores.19 Time to deterioration in physical well-being was shorter with capivasertib plus abiraterone (HR: 1.43), while no differences were observed in time to deterioration for functional well-being (HR: 1.06) or the FACT-P total score (HR: 1.10). Patients receiving capivasertib plus abiraterone experienced more symptomatic AEs (diarrhea, rash), which was consistent with the earlier decline in self-reported physical well-being, but this did not adversely affect functional domains such as daily activities and sleep or overall HRQoL.
PSMAddition: [177Lu]Lu-PSMA-617 delays radiographic progression in patients with mHSPC
Radioligand therapy is also moving earlier in prostate cancer, extending the concept of triplet intensification and targeted agents.20 Lutetium (177Lu) vipivotide tetraxetan ([177Lu]Lu-PSMA-617) is currently indicated for the treatment of adult patients with progressive PSMA-positive mCRPC who have been treated with an ARPI and taxane-based chemotherapy,21 as well as those patients with mCRPC who have been treated with ARPI for whom delaying taxane-based chemotherapy is considered appropriate. Based on its demonstrated efficacy in mCRPC, the first phase III study has been initiated to evaluate this PSMA-targeted radioligand therapy in patients with mHSPC.22
In the phase III PSMAddition trial, patients with untreated or minimally treated PSMA-positive mHSPC were randomized 1:1 to receive either [177Lu]Lu-PSMA-617 at 7.4 GBq ±10% every six weeks for six cycles plus ARPI and ADT, or ARPI and ADT alone, with crossover permitted after confirmed radiographic progression.22 Presented at the 2025 ESMO Congress, the second interim analysis showed a significant rPFS benefit with [177Lu]Lu-PSMA-617 (HR: 0.72 [95% CI: 0.58–0.90]; p=0.002), with median rPFS not reached in both groups.22 In the first interim OS analysis, the median OS was also not reached in both arms (HR: 0.84 [95% CI: 0.83–1.13]; p=0.125). The ORR was 85.3% in the [177Lu]Lu-PSMA-617 group versus 80.8% in the control arm and the complete response rates were 57.1% and 42.3%. The experimental regimen improved multiple disease control measures, including PSA progression and PSA nadir <0.2 ng/mL at 48 weeks.
Safety findings showed higher treatment-related toxicity with [177Lu]Lu-PSMA-617, with grade ≥3 TRAEs in 22.7% versus 12.2% with ARPI plus ADT alone.22 [177Lu]Lu-PSMA-617 was associated with more frequent xerostomia (48.5% vs 3.9%) and cytopenias (44.0% vs 20.4%; grade ≥3, 14.4% vs 5.0%). Despite this, recently presented data showed that patient-reported outcomes were generally comparable between groups.23 HRQoL and pain were largely maintained with the addition of [177Lu]Lu-PSMA-617, with no meaningful or statistically significant differences in time to worsening across standard metrics. A modest early decline in HRQoL was observed during active triplet therapy, but this was transient, with recovery over time and convergence between treatment arms. Pain control remained comparable throughout, with no evidence of increased symptom burden. Similarly, the risk of symptomatic skeletal events was not increased in the experimental arm. Time to first symptomatic skeletal event, with or without death, was comparable between groups (HR: 0.89) and median time to event was not reached in either arm.
Muscle-invasive bladder cancer
Muscle-invasive bladder cancer (MIBC) emerged as one of the most active areas within genitourinary oncology, driven by two landmark phase III trials initially presented at the ESMO Congress 2025: KEYNOTE-905/EV-303 and IMvigor011. For the first time, perioperative strategies demonstrated substantial survival benefits in patients who are ineligible for cisplatin, while circulating tumor (ct)DNA-guided postoperative treatment provided compelling evidence that molecular residual disease can help guide escalation and de-escalation decisions.24,25 These findings support more personalized perioperative care and challenge traditional “one-size-fits-all” postoperative management.
KEYNOTE-905/EV-303: Perioperative enfortumab vedotin plus pembrolizumab significantly improves clinical outcomes in patients with cisplatin-ineligible MIBC
For decades, the mainstay of curative-intent treatment in MIBC has been neoadjuvant cisplatin-based chemotherapy followed by radical cystectomy with pelvic lymph node dissection (RC + PLND).26 However, nearly half of patients are ineligible for cisplatin and outcomes with surgery alone have historically been poor, leaving this group as the “forgotten half” of MIBC.27–29 The KEYNOTE-905/EV-303 study is the first phase III trial to show a meaningful benefit in cisplatin-unfit or cisplatin-declining patients, and it may redefine the treatment landscape for this underserved population.24
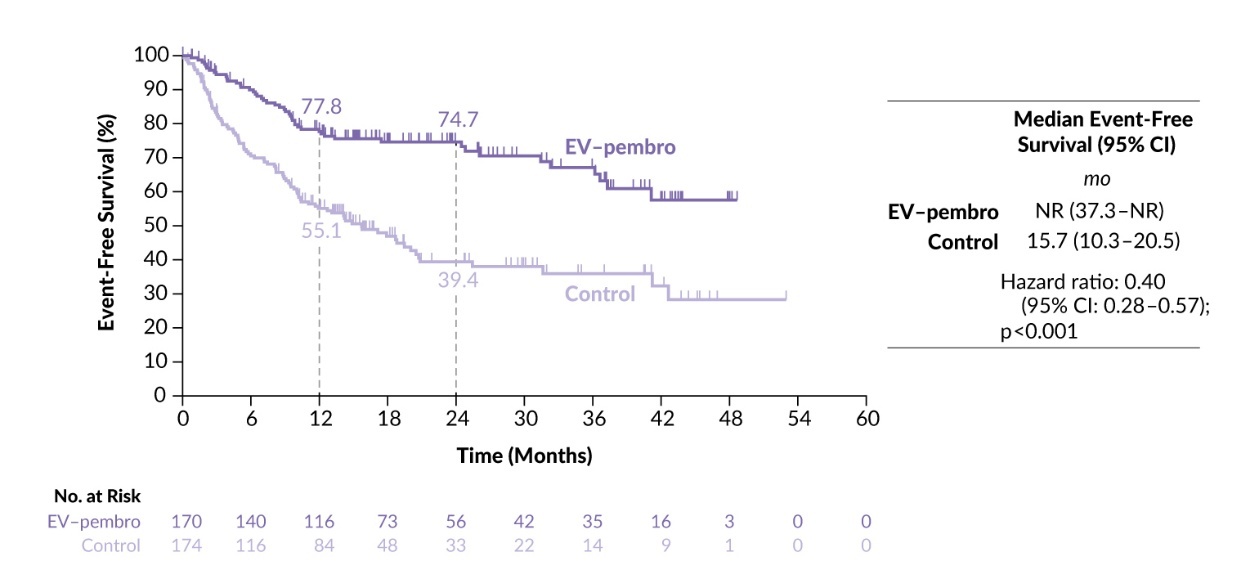
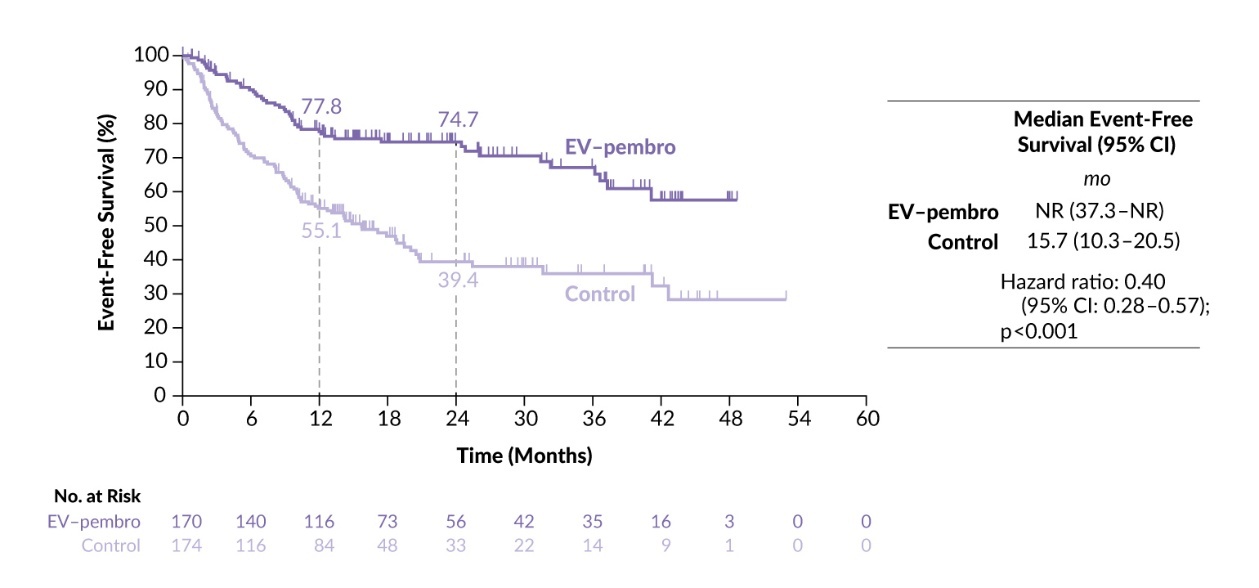
This trial evaluated perioperative enfortumab vedotin (EV), a nectin-4-directed antibody-drug conjugate, combined with pembrolizumab and RC + PLND compared with RC + PLND alone in patients with clinical stage T2–T4aN0M0 or T1–T4aN1M0 MIBC who were ineligible for or declined cisplatin.24,30 At a median follow-up of 25.6 months, the trial met its primary endpoint, demonstrating a significant improvement in EFS. The median EFS was not reached with perioperative EV plus pembrolizumab versus 15.7 months with surgery alone (HR: 0.40 [95% CI: 0.28–0.57]; one-sided p<0.0001), with 12- and 24-month EFS rates of 77.8% and 74.7% for the combination compared with 55.1% and 39.4% for surgery alone (Figure 4). The benefit was consistent across subgroups including age, ECOG performance status, region, cisplatin eligibility, PD-L1 combined positive score and tumor stage.
Importantly, the EFS gain translated into an OS advantage in this analysis.24,30 Median OS was not reached with EV plus pembrolizumab versus 41.7 months with surgery alone (HR: 0.50 [95% CI: 0.33–0.74]; one-sided p=0.0002), with 12-month OS rates of 86.3% versus 75.7% and 24-month rates of 79.7% versus 63.1%.
Pathological complete response (pCR) rates were also unprecedented in this setting, at 57.1% with EV plus pembrolizumab versus 8.6% with surgery alone, for an estimated difference of 48.3% (p<0.000001).24,31 Exploratory analyses suggested that pCR correlated with longer EFS, with median EFS not reached versus 41.2 months among those achieving pCR (HR: 0.43 [95% CI: 0.16–1.16]); among patients without pCR, median EFS was 26.1 months versus 14.2 months (HR: 0.76 [95% CI: 0.51–1.14]).24
Results also showed that pathological downstaging below pT2N0 was markedly more common among patients receiving EV plus pembrolizumab, with rates of 65.9% compared with 12.6% in the control arm.31 Furthermore, the median disease-free survival (DFS) was not reached with EV plus pembrolizumab versus 23.6 months with surgery alone and 24-month rates were 83.2% versus 49.6%, respectively.
Toxicity was consistent with prior experience from advanced urothelial carcinoma and requires proactive management in an older, frailer population.24 Grade ≥3 TEAEs occurred in 71.3% of patients receiving EV plus pembrolizumab versus 45.9% with surgery alone, and serious AEs occurred in 58.1% versus 40.9%, respectively. EV-related events of special interest included skin reactions (57.5%), peripheral neuropathy (36.5%) and ocular disorders (17.4%), while pembrolizumab-related events included hypothyroidism (14.4%), severe skin reactions (13.8%) and hyperthyroidism (4.8%).
Overall, the KEYNOTE-905/EV-303 trial demonstrated unprecedented improvements in clinical outcomes, which positions perioperative EV plus pembrolizumab as a potential new standard of care for this underserved, high-risk population.32 Key open questions include the optimal duration of adjuvant therapy and whether treatment de-escalation is feasible in selected responders, while established alternatives such as adjuvant nivolumab and perioperative durvalumab plus chemotherapy remain relevant in selected patients.33–35
KEYNOTE-B15/EV-304: Perioperative enfortumab vedotin plus pembrolizumab improves outcomes versus chemotherapy in cisplatin-eligible MIBC
Perioperative EV plus pembrolizumab was further investigated in the phase III EV-304/KEYNOTE-B15 trial in patients with MIBC eligible for cisplatin. In this study, 808 patients were randomly assigned 1:1 to receive either EV plus pembrolizumab or cisplatin plus gemcitabine.36 Both groups received four cycles of neoadjuvant therapy, followed by RC + PLND; postoperatively, patients received either EV (five cycles) plus pembrolizumab (13 cycles) or observation, respectively.
At the ASCO Genitourinary Cancers Symposium 2026, Prof. Matthew D. Galsky reported a significant improvement in EFS with EV plus pembrolizumab versus chemotherapy, with median EFS not reached versus 48.5 months and 24-month EFS rates of 79.4% versus 66.2% (HR: 0.53 [95% CI: 0.41–0.70]; p<0.001).36 The pCR rate was 55.8% with EV plus pembrolizumab compared with 32.5% with chemotherapy, translating into an estimated difference of 23.4% (p<0.0001). OS data were immature, with medians not reached in either arm.
The safety profile of EV plus pembrolizumab was consistent with prior reports.36 Nearly all patients experienced any-grade TEAEs, with grade ≥3 events occurring in 75.7% of patients in the EV plus pembrolizumab arm versus 67.2% in the cisplatin plus gemcitabine arm. The most common TEAE was pruritus (46.2%) with the combination and anemia (56.3%) with chemotherapy. Among grade ≥3 AEs of special interest, skin reactions were most frequent with EV (14.1%), while severe skin reactions were the most common with pembrolizumab (13.9%).
These findings support perioperative EV plus pembrolizumab as a potential alternative to cisplatin-based chemotherapy and suggest a shift toward a platinum-free perioperative therapy.
IMvigor011: ctDNA positivity is strongly predictive of adjuvant immunotherapy benefit in MIBC
Approximately half of the patients with MIBC will eventually recur after cystectomy and the recurrence is associated with poor outcomes. Although adjuvant immunotherapy is recommended in some settings, treating unselected patients after surgery has not consistently improved survival.37 The phase III IMvigor011 study was designed based on strong evidence that ctDNA detection of molecular residual disease is prognostic after surgery and may predict benefit from adjuvant immunotherapy.25,38,39 In this first randomized ctDNA-guided study to demonstrate a survival benefit in bladder cancer, patients with high-risk MIBC were tested for ctDNA following cystectomy. Those who were ctDNA-positive were randomized to receive atezolizumab or placebo, while persistently ctDNA-negative patients entered active surveillance.
At a median follow-up of 16.1 months, ctDNA-positive patients receiving atezolizumab experienced statistically significant improvements in DFS (HR: 0.64 [95% CI: 0.47–0.87]; p=0.0047) and OS (HR: 0.59 [95% CI: 0.39–0.90]; p=0.0131) versus placebo.25,39 Across patient subgroups, adjuvant atezolizumab was generally associated with improved outcomes. Furthermore, the prognosis of persistently ctDNA-negative patients was notably favorable, with DFS rates of 95.4% at the end of the one-year monitoring period and 88.4% at two years, and OS rates of 100% at one year and 97.1% at two years.
An exploratory analysis presented at the ASCO Genitourinary Cancers Symposium 2026 further showed that adjuvant atezolizumab promoted reductions in ctDNA levels and increased ctDNA clearance compared with placebo, which was associated with improved clinical outcomes.40 In contrast, patients with early ctDNA positivity or higher ctDNA levels had worse outcomes. For example, patients who were ctDNA-negative had 24-month DFS rates of 88.4% and OS of 97.1%, whereas those with ctDNA detected at the initial test had poorer outcomes, with rates of 8.2% and 48.5%, respectively. Atezolizumab improved DFS and OS versus placebo across ctDNA-defined subgroups, with a greater relative benefit observed in patients with higher ctDNA levels. Beyond simple positive/negative status, both the timing of ctDNA detection and its concentration provided additional prognostic value, as early positivity and higher levels were consistently associated with shorter survival. However, the efficacy of atezolizumab appeared consistent regardless of ctDNA timing or concentration.
Although atezolizumab is not yet approved for adjuvant use in MIBC, IMvigor011 represents a critical step toward biomarker-driven perioperative care. Ongoing trials are now exploring ctDNA-guided escalation and de-escalation strategies, bladder-preserving approaches and refined biomarker algorithms.41,42
Metastatic clear cell renal cell carcinoma
In metastatic clear cell renal cell carcinoma (ccRCC), first-line therapy is currently established as a PD-1-based immune checkpoint inhibitor combined either with a CTLA-4 inhibitor or with an angiogenesis-targeted therapy.43 The optimal choice of second-line treatment after progression on PD-1-based regimens remains uncertain. Prospective second-line data after first-line PD-1-targeted therapy are available for several agents, including axitinib, pazopanib, cabozantinib, lenvatinib plus everolimus and sunitinib, but interpretation is complicated by trial heterogeneity and the lack of head-to-head comparisons among commonly used options.
LITESPARK-011: Clinical benefits with belzutifan plus lenvatinib versus cabozantinib in advanced ccRCC
Combining belzutifan, the first HIF-2α inhibitor indicated for advanced RCC after prior anti-PD-1/PD-L1 and antiangiogenic therapy, with lenvatinib, a potent VEGFR tyrosine kinase inhibitor, may improve outcomes through complementary inhibition of angiogenesis pathways.44 This combination was assessed in the phase III LITESPARK-011 trial in patients with unresectable, locally advanced or metastatic ccRCC who had received up to two prior systemic therapies and experienced disease progression after immune checkpoint inhibitor treatment in the first- or second-line setting.45 A total of 747 patients were randomly assigned to receive belzutifan 120 mg plus lenvatinib 20 mg (n=371) or cabozantinib 60 mg (n=376).
In the second interim analysis at a median follow-up of 29.0 months, belzutifan plus lenvatinib significantly improved PFS compared with cabozantinib, with median PFS of 14.8 months versus 10.7 months and 24-month PFS rates of 35.6% versus 19.1% (HR: 0.70 [95% CI: 0.59–0.84]; p=0.00007).45 OS also favored the combination, although the difference did not reach statistical significance. Median OS was 34.9 months with belzutifan plus lenvatinib versus 27.6 months with cabozantinib (HR: 0.85 [95% CI: 0.68–1.05]; p=0.06075), with 24-month OS rates of 62.8% and 55.4%, respectively.
Response outcomes were also improved with the combination. The ORR was 52.6% with belzutifan plus lenvatinib compared with 40.2% with cabozantinib, including complete response rates of 5.4% versus 1.1%, respectively.45 Median duration of response was 23.0 months versus 12.3 months, with 24-month rates of 49.5% versus 25.5%, respectively.
The safety profiles were broadly comparable between the treatment arms. Grade 3 TEAEs occurred in 84.1% of patients receiving belzutifan plus lenvatinib and 82.7% of those receiving cabozantinib and serious AEs were reported in 51.6% versus 43.9% of patients, respectively.45 The most common AEs with the combination were anemia (69.2%), hypertension (58.9%) and diarrhea (52.7%). Hypoxia occurred more frequently with belzutifan plus lenvatinib (15.4% overall; grade ≥3, 11.9%) and was not observed with cabozantinib. Cardiac dysfunction was also more common with the combination (7.0% vs 1.1%), including grade ≥3 events in 4.6% versus 0.5% of patients.
LITESPARK-022: Adding belzutifan to adjuvant pembrolizumab reduced the risk of recurrence in high-risk ccRCC
Adjuvant pembrolizumab is the standard of care for patients with high-risk RCC based on the phase III KEYNOTE-564 trial, which demonstrated improved DFS and OS versus placebo.46 The phase III LITESPARK-022 trial evaluated whether adding belzutifan to adjuvant pembrolizumab could further improve outcomes in patients with resected ccRCC at increased risk of recurrence and no prior systemic therapy.47 In total, 1,841 patients were randomly assigned 1:1 to receive pembrolizumab 400 mg every six weeks for up to nine cycles plus either belzutifan 120 mg daily (n=921) or placebo (n=920).
After a median follow-up of 28.4 months, pembrolizumab plus belzutifan significantly improved DFS compared with pembrolizumab alone, showing median DFS of not reached in either arm, with a 28%-reduced risk of recurrence or death with pembrolizumab plus belzutifan (HR: 0.72 [95% CI: 0.59–0.87]; p=0.0003).47 The 12-, 24- and 30-month DFS rates were 91.9%, 85.2% and 80.7% versus 73.7%, 75.8% and 68.6% with combination versus pembrolizumab alone. OS data remained immature at the time of the analysis, with only 29% of expected events reported. Median OS was not reached in either arm and the 30-month OS rates were 95.6% with pembrolizumab plus belzutifan and 93.8% with pembrolizumab alone.
The addition of belzutifan increased toxicity compared with pembrolizumab alone.47 Grade ≥3 TEAEs occurred in 52.1% versus 30.2% of patients, and discontinuation of all study therapy due to AEs occurred in 11.9% versus 9.0%, respectively. The most common AEs with the combination were anemia (84.0%), fatigue (36.4%) and increased alanine aminotransferase levels (28.9%). Grade ≥3 anemia occurred in 12.1% of patients receiving belzutifan, while hypoxia was reported in 7.0% of patients, including grade ≥3 events in 4.6%.
Germ cell cancer: Stage II seminoma
For stage IIA seminoma, The European Association of Urology (EAU), ESMO and National Comprehensive Cancer Network (NCCN) guidelines recommend para-aortic and ipsilateral iliac radiotherapy or chemotherapy as standard options.48–50 Across guidelines, standard chemotherapy includes bleomycin, etoposide and cisplatin (BEP) or etoposide and cisplatin (EP) alone if bleomycin is contraindicated. For stage IIB seminoma, there is broad consensus that primary chemotherapy with BEP or EP is preferred due to greater disease volume, although radiotherapy can be considered in select cases. Single-dose carboplatin plus involved-node radiotherapy has been incorporated to the NCCN guidelines as an alternative option.50 This approach is supported by a 3-year PFS rate of 93.7% and a median 75% reduction in irradiated volume, with minimal acute toxicity.51 Long-term follow-up data presented at the ESMO Congress 2025 by Dr Alexandros Papachristofilou further reinforce this regimen as a guideline-endorsed alternative to standard radiotherapy or multi-cycle cisplatin-based chemotherapy in this setting.51,52
SAKK 01/10: Single-dose carboplatin and radiotherapy demonstrate long-term efficacy with minimal toxicity in patients with stage II seminoma
SAKK 01/10 was a prospective, single-arm therapy optimization trial that enrolled 116 patients with stage IIA or stage IIB seminoma across 20 centers in Switzerland and Germany.51,52 All patients received one cycle of carboplatin (AUC 7), followed three weeks later by involved-node radiotherapy delivered at a dose of 30 Gy for stage IIA and 36 Gy for stage IIB disease.
With a median follow-up of 8.1 years, long-term outcomes remained highly favorable.52 The 10-year PFS rate was 92.8% overall, with rates of 95.2% in stage IIA and 91.3% in stage IIB disease. No additional disease-related events were observed beyond the time of the primary analysis, and 85 patients remained in active follow-up. The 10-year OS rate was estimated at 99.1%, with a seminoma-specific survival rate of 100%.
Late toxicity were uncommon.52 One patient experienced treatment-related non-ST elevation myocardial infarction seven years after treatment, four patients developed a contralateral stage I germ cell tumor and four patients were diagnosed with other second primary malignancies. Events reported at the time of the primary analysis included two contralateral germ cell tumors, one renal cancer and one fatal cholangiocarcinoma.51 Extended follow-up identified two additional germ cell tumors, as well as one case of urothelial bladder cancer with incidental prostate cancer and one case of basal cell carcinoma.52 All second primary tumors occurred outside the radiotherapy fields and were not considered related to the study treatment.
Conclusions
Genitourinary cancer treatment is moving toward earlier and more personalized use of systemic therapies. New data from the major oncology meetings will likely influence routine practice across prostate, bladder, kidney and germ cell cancers. In prostate cancer, recent trials confirm a shift toward earlier and biomarker-driven treatment intensification, with survival gains demonstrated for androgen receptor-targeted combinations in high-risk biochemical recurrence and meaningful disease control improvements with targeted triplet strategies in mHSPC. Furthermore, perioperative systemic therapy in MIBC has entered a new period, with EV plus pembrolizumab delivering unprecedented survival benefits in cisplatin-ineligible patients and ctDNA-guided strategies identifying who truly benefits from adjuvant immunotherapy. In metastatic and high-risk ccRCC, LITESPARK-011 and LITESPARK-022 are the first phase III studies to demonstrate improved outcomes with the addition of the HIF-2α inhibitor belzutifan to lenvatinib and adjuvant pembrolizumab, respectively, supporting belzutifan-based combinations as promising new treatment strategies in both advanced and adjuvant ccRCC settings.45,47 Finally, long-term follow-up from SAKK 01/10 confirms that single-dose carboplatin plus involved-node radiotherapy achieves durable disease control with minimal late toxicity.
Conflict of interest
The author received advisory board and speaker honoraria from the following entities. Private: Astellas, healthbook and Bayer; institutional: Roche, Janssen, Bayer, Merck, MSD, BMS, Pfizer, Novartis AAA, SAMO, ESMO, ESO and healthbook. Grant funding: Fond’Action Contre le cancer.
Funding
The author has declared that no financial support was received from any organization for the submitted work.
Author contributions
The author has created and approved the final manuscript.
AI use
The author declared that no generative artificial intelligence (AI) or AI-assisted technologies were used in the preparation or writing of this manuscript. All content was produced entirely by the author who takes full responsibility for the accuracy, integrity and originality of the work.