Introduction
Endometrial cancer is the sixth most common cancer among women globally and the most frequently diagnosed gynecological malignancy in high-income countries.1 In 2022, an estimated 420,000 new cases were reported worldwide, along with approximately 97,000 deaths. The global incidence of endometrial cancer is steadily rising, largely driven by the increasing prevalence of obesity and the aging population.2,3 While Type I endometrioid carcinomas that are estrogen- and adiposity-associated remain the largest contributor to overall disease incidence, multiple population-based registries have reported steep relative increases in Type II high-risk, relatively hormone-independent non-endometrioid histologies in the United States and in parts of Europe.4–6 Endometrial cancer typically affects postmenopausal women, with a median age at diagnosis of 65 years.7 In most cases, abnormal vaginal bleeding facilitates early detection, enabling diagnosis before the disease extends beyond the uterus in approximately 75% of patients.8,9 The prognosis is generally favorable, with an overall 5-year survival rate of 86%, which increases to 97% when the disease is confined to the uterus. In Switzerland, the 5-year relative survival rate reported between 2000 and 2009 was 75.2%.10 The standard treatment for early-stage endometrial cancer is total hysterectomy with bilateral salpingo-oophorectomy (BSO), typically performed via a minimally invasive laparoscopic approach, resulting in surgical menopause in premenopausal women who represent roughly 25% of cases.2,9 In addition to hysterectomy and BSO, current guidelines from the European Society of Gynaecological Oncology (ESGO)/European Society for Radiotherapy and Oncology (ESTRO)/European Society of Pathology (ESP),2 as well as the National Comprehensive Cancer Network (NCCN),11 recommend sentinel lymph node mapping as part of standard surgical staging in early-stage endometrial cancer.
Menopausal symptoms, such as hot flashes, night sweats, sleep disturbances, mood changes, vaginal atrophy and sexual dysfunction, can significantly impact quality of life (QoL). In women who have undergone treatment for endometrial cancer, these symptoms may be more severe than those experienced during natural menopause.12 Hormone replacement therapy (HRT), using either estrogen alone or in combination with progestin, remains the most effective treatment for alleviating menopausal symptoms. However, concerns regarding the potential risk of cancer recurrence have limited its use among endometrial cancer survivors. This review article summarizes the current evidence on the oncologic safety of HRT in this population and provides recommendations regarding its appropriate use in patients with endometrial cancer.
Endometrial cancer: Background and classification
Traditionally, endometrial cancer has been classified into two broad types based on histopathological features and hormonal responsiveness.9,13 Type I cancers are predominantly endometrioid adenocarcinomas, which are estrogen-dependent, generally low-grade and most often diagnosed at an early stage. These tumors typically arise in the setting of unopposed estrogen exposure, often related to obesity, metabolic syndrome or chronic anovulation, and are associated with a favorable prognosis. In contrast, Type II cancers, which include serous carcinoma, clear cell carcinoma and carcinosarcoma, are not clearly hormone-driven, exhibit high-grade histologic features and tend to behave more aggressively with a higher risk of recurrence and metastasis. They are also more likely to be diagnosed at an advanced stage and are associated with significantly worse outcomes. While stage IA endometrioid tumors are associated with 5-year survival rates of >90%, patients with high-risk histologic subtypes often have survival rates below 50%.2,7 Reflecting the advances in understanding tumor biology, the International Federation of Gynecology and Obstetrics (FIGO) recently updated its staging criteria to incorporate both histologic and molecular features.13 The updated ESGO/ESTRO/ESP clinical guidelines2 incorporate the new approach through an integrated classification model that combines histotype, tumor grade, invasion pattern, lymphovascular space invasion and key molecular alterations, enabling individualized treatment planning and improved prognostication.
Risks of HRT in endometrial cancer: The Women’s Health Initiative trial
The use of HRT in endometrial cancer survivors has long been a subject of debate due to concerns regarding the potential for hormone-driven tumor recurrence. Traditionally, HRT was avoided following endometrial cancer treatment, largely due to evidence from the general population showing that both tamoxifen and unopposed estrogen are associated with an increased risk of endometrial hyperplasia and carcinoma14–17 due to stimulation of the mitotic activity of the endometrium, which potentially increases its susceptibility to malignant transformation.18,19 These findings led to the assumption that any estrogen exposure in women previously treated for endometrial cancer could stimulate residual malignant cells and increase the risk of recurrence, even though adding progestin can mitigate this effect. The Women’s Health Initiative (WHI) trial evaluated the safety of HRT in postmenopausal women with an intact uterus.20 A total of 16,608 patients received conjugated equine estrogens (0.625 mg/day) plus medroxyprogesterone acetate (2.5 mg/day) (n=8,506) or placebo (n=8,102). The primary endpoint was coronary heart disease (CHD), including nonfatal myocardial infarction and CHD death, with invasive breast cancer as the primary adverse outcome. The study demonstrated an increased incidence of CHD (HR: 1.29 [95% CI: 1.02–1.63]) and breast cancer (HR: 1.26 [95% CI: 1.00–1.59]) versus placebo at an average follow-up of 5.2 years. The estrogen plus progestin arm of the WHI study was prematurely closed because the overall risks exceeded the benefits. Notably, these risks were not observed in the latter-reported estrogen-alone component of the study in postmenopausal women with prior hysterectomy (n=10,739) (CHD, HR: 0.91 [95% CI: 0.75–1.12]; breast cancer, HR: 0.77 [95% CI: 0.59–1.01]), albeit a higher risk of stroke (HR: 1.39 [95% CI: 1.10–1.77]) was noted.21 The results also suggested that estrogen alone had advantages over estrogen plus progestin. Importantly, there were fewer endometrial cancers in the combined HRT arm compared with the placebo arm (yearly incidence, 0.06% vs 0.10%; HR: 0.65 [95% CI: 0.48–0.89]; p=0.007) and statistically nonsignificant reduction in deaths from endometrial cancer in the HRT arm (5 vs 11 deaths, HR: 0.42 [95% CI: 0.15–1.22]) after a median cumulative follow-up of 13 years.22
Long-term follow-up data of the trial (mean, 10.7 years) in women receiving unopposed estrogen (median use, 5.9 years) indicated no differences in the postintervention risk of stroke (0.36% vs 0.41% with placebo, HR: 0.89 [95% CI: 0.64–1.24]), while the breast cancer reduction persisted overall (HR: 0.77 [95% CI: 0.62–0.95]) and total cancer incidence post-intervention did not differ significantly (HR: 0.93 [95% CI: 0.77–1.13]).23 Nevertheless, HRT in endometrial cancer survivors was historically restricted to patients with severe vasomotor symptoms or urogenital atrophy due to concerns of occult disease.
Recent evidence of HRT safety in endometrial cancer survivors
More recent evidence challenged the concept of avoiding HRT following endometrial cancer treatment, indicating no increased risk of cancer recurrence, particularly in women with low-risk disease who have undergone complete surgical treatment. The data from key studies investigating the safety of HRT in women with endometrial cancer are summarized below.
The randomized, double-blind GOG 137 trial performed by the Gynecologic Oncology Group evaluated the effect of estrogen replacement therapy versus placebo on recurrence rate and survival in women who have undergone hysterectomy for stage I–IIB endometrial carcinoma.24 Enrollment dropped sharply following the publication of the initial WHI results, although patients were receiving estrogen alone and not estrogen plus progesterone. Ultimately, the trial was stopped prematurely with 1,236 eligible patients enrolled, as it became evident that reaching the planned accrual target of 2,108 patients was no longer feasible.
At a median follow-up of 35.7 months, recurrence rates in the overall population were low and 3-year progression-free survival (PFS) rate was 94.3% in the HRT group and 95.6% in the placebo group.24 The trial showed no significant difference in recurrence risk between the HRT and placebo arms (relative risk [RR]: 1.27 [80% CI: 0.916–1.77]). Although the study did not enroll a sufficient number of high-risk patients and could not conclusively confirm or refute the safety of HRT in terms of recurrence risk, it did demonstrate a low incidence of recurrence and new malignancies, thereby contributing to the evidence base for evaluating the overall risk–benefit profile of HRT in patients with low-risk endometrial cancer. Of note, a retrospective analysis of the trial data showed a racial disparity in the HRT arm, with increased risk of recurrence among Black versus White patients who continued to receive HRT following primary treatment (RR: 11.2 [95% CI: 2.86–43.59]; p=0.0005).25
A prospective case-control study by Ayhan et al. evaluating the safety of immediate postoperative HRT in endometrial cancer survivors included 50 women with stage I or II endometrioid-type endometrial cancer who received HRT initiated 4–8 weeks after surgery and 52 matched controls who did not receive HRT.26 The average duration of HRT was 49.1 months and most patients continued therapy for ≥24 months. The study demonstrated no recurrences in the HRT group during follow-up. In the control group, one pelvic recurrence occurred at 12 months, resulting in death despite chemotherapy, and one death due to intercurrent disease at 21 months post surgery. Adverse effects of HRT were minimal, with seven patients discontinued the treatment, among them only two within the first 24 months. While the study was non-randomized and had a limited sample size, the data demonstrated that immediate postoperative use of continuous HRT did not increase the risk of recurrence or death in women with early-stage, low-risk endometrial cancer.
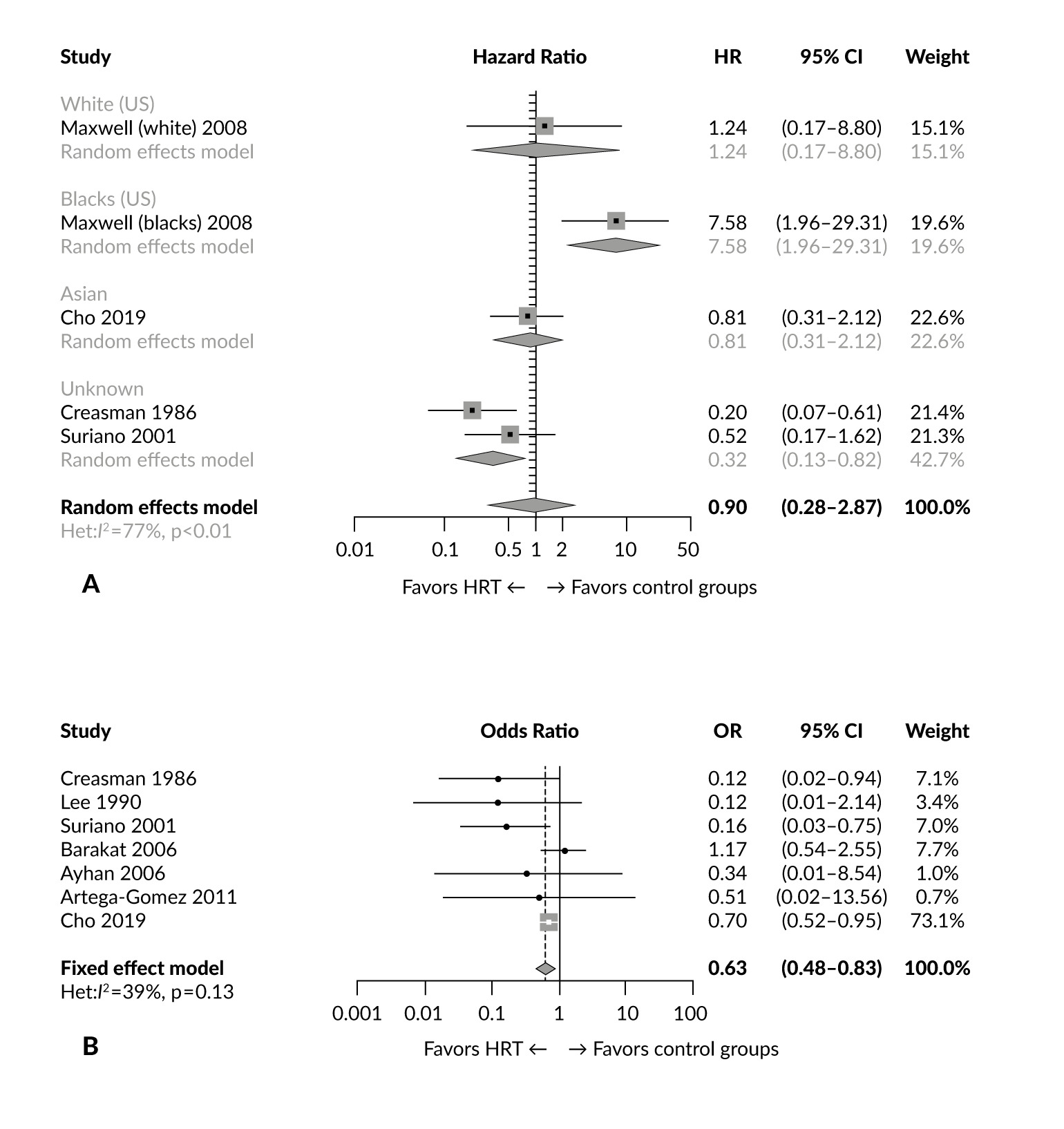
Several systematic reviews aimed to evaluate the safety and effectiveness of HRT in women treated for endometrial cancer. Edey et al.27 identified GOG 13724 as the only randomized controlled trial that met the inclusion criteria for assessing HRT in this patient population, based on searches of the Cochrane Register of Controlled Trials, MEDLINE and Embase. Di Donato et al. screened 1,332 abstracts and included seven eligible studies in the analysis, among them four retrospective series, one prospective study, one randomized controlled trial and one population-based study.28 Overall, across predominantly stage I–II cohorts, HRT use was not associated with a statistically significant increase in recurrence compared with controls. An important limitation was selection bias, as HRT was preferentially prescribed to younger women with low-risk, early-stage disease. A more recent meta-analysis included both randomized and observational studies, comprising 10 papers published between 1986 and 2021.29 Of these, two reported data from randomized clinical trials, five were non-randomized cohort studies and three were case-control studies.24–26,30–34 The total sample included 7,944 patients, including 1,801 treated with HRT and 6,015 controls. Based on four studies that allowed time-dependent analysis, the study indicated no significant difference in disease-free survival between women treated with HRT and those not treated (pooled HR: 0.90 (95% CI: 0.28–2.87). However, significantly increased risk of recurrence was reported among Black American women treated with continuous estrogen (HR: 7.58 (95% CI: 1.96–29.31),29 confirming the findings of the GOG 137 trial.25 A pooled odds ratio (OR) of 0.63 (95% CI: 0.48–0.83) across all included studies indicated a significantly reduced risk of recurrence among endometrial cancer survivors treated with HRT. Combined estrogen and progestin therapy, particularly when administered in cyclic regimens, appeared to be the most favorable for reducing the recurrence risk. The results of this study are summarized in Figure 1.
_meta-analysis_(a)_and_odds_ratio_(or)_(b)_meta-analysis_f.png)
Taken together, the existing evidence suggests that HRT appears safe in women with low-grade, early-stage endometrial cancer after hysterectomy. However, since most available data are derived from surgically treated stage I cohorts with limited use of adjuvant radiotherapy or systemic therapy, the oncologic safety of HRT in women receiving adjuvant treatment remains insufficiently studied, warranting a cautious approach. Therapy initiation should be tailored to the patient’s needs and undertaken following careful discussion with the patient regarding its risks and benefits. As molecular classification is increasingly incorporated into prognostic risk stratification and treatment planning, it may further refine individualized counselling regarding the use of HRT after endometrial cancer. While clinical evidence remains limited, this approach may become relevant for polymerase epsilon (POLE)-mutated, mismatch repair (MMR)-deficient, no specific molecular profile (NSMP) and p53-abnormal tumors. Specifically, the excellent prognosis of POLE-mutated tumors could support a more permissive approach, whereas p53-abnormal or serous-like disease may justify greater caution with systemic HRT.
Beyond HRT safety, the potential protective role of progestins after hysterectomy remains a relevant clinical question. In healthy postmenopausal women, continuous combined estrogen–progestin therapy has been associated with a reduced risk of developing endometrial cancer, supporting a biologically plausible antiproliferative effect of progestins on residual endometrial tissue.35 Consistent with this rationale, a systematic review by Shim et al. reported an inverse association between recurrence risk and the use of combined estrogen–progestin therapy compared with estrogen monotherapy in endometrial cancer survivors, suggesting a possible protective effect.36 Moreover, in selected young women with atypical hyperplasia or well-differentiated endometrioid endometrial cancer who desire fertility preservation, high-dose oral progestins or levonorgestrel-releasing intrauterine devices are established therapeutic options until endometrial normalization is achieved, further underscoring the antitumor activity of progestins in hormonally driven disease.2
However, these potential benefits must be balanced against important safety considerations. Progestin-containing regimens are associated with an increased risk of breast cancer compared with estrogen-only therapy, and may exert unfavorable metabolic and cardiovascular effects.37,38 This is particularly relevant in women with hypertension, diabetes mellitus, metabolic syndrome, polycystic ovary syndrome or obesity, which are highly prevalent among patients with endometrial cancer, thereby limiting the routine use of progestins after hysterectomy and reinforcing the need for individualized risk–benefit assessment.
Recommendations for the use of HRT in women with endometrial cancer
Choice of HRT regimen
The choice of HRT in endometrial cancer survivors depends on surgical history, symptom profile, comorbidities and oncologic risk. Swiss clinical practice is aligned with the ESGO-ESTRO-ESP guidelines for the management of endometrial carcinoma,2 while substance- and route-specific recommendations for menopausal HRT follow the European Menopause and Andropause Society (EMAS) guidelines.39 In addition to treating menopausal symptoms, the decision for or against HRT should include a discussion of other long-term benefits of HRT with the patient. In women under 60 years of age using HRT, the absolute risks for overall mortality, fractures, diabetes mellitus (estrogen-progesterone therapy and estrogen-only therapy) and breast cancer (estrogen therapy) are reduced. This is especially important in women with endometrial cancer who often have a higher risk of these diseases due to obesity and already existing unfavorable metabolic profile.
In patients who have undergone total hysterectomy for low-grade early-stage endometrial cancer and whose menopausal symptoms significantly compromise their QoL, estrogen-only replacement therapy at the lowest effective dose could be considered.11,12,40,41 Common formulations based on early studies include oral 17β-estradiol (E2) starting at a dose of 1 mg/day or conjugated equine estrogen (CEE) at 0.625 mg/day (not available/used in Switzerland).42–44 Alternatively, transdermal estradiol patches delivering 25 (low dose) to 100 µg/day (high dose), estradiol gel or spray are also widely used. Transdermal administration is often favored in women with cardiovascular risk factors because it is associated with a lower risk of venous thromboembolism, stroke and cardiovascular events due to avoiding first-pass hepatic metabolism, which results in fewer adverse effects on coagulation and inflammatory markers.40,43,45
For patients experiencing isolated genitourinary syndrome of menopause (GSM) with persistent symptoms, low-dose local estrogen therapy delivered via cream, pessary or intravaginal ring may be considered due to its minimal systemic absorption and endometrial safety profile.46–49 This approach is supported by both the EMAS and Swiss expert recommendations and is appropriate when vasomotor symptoms are absent and GSM remains the predominant clinical concern.
Timing of HRT administration
The initiation of systemic HRT is generally delayed until 6–12 months after the completion of cancer treatment, allowing for confirmation of disease remission.11 This cautious approach aligns with clinical consensus to reduce the risk of stimulating residual or occult disease. Therapy should be initiated at the lowest effective dose and reassessed annually. Monitoring includes regular clinical evaluation and adjustment of therapy based on symptom control and emerging health risks.
Who should avoid HRT?
HRT is contraindicated in patients with active or recurrent disease and in those with high-risk histologic subtypes such as serous, clear cell or carcinosarcoma or with advanced-stage disease (FIGO stage III or IV).11,12,40 While data are lacking for these populations, there is a theoretical concern regarding the potential for hormone-driven recurrence. In addition, contraindications unrelated to cancer, including a personal history of thromboembolism, active liver disease or estrogen-sensitive comorbidities, should be carefully considered in line with general menopause management guidelines.
Alternative non-hormonal options
For women who are ineligible for or who decline HRT, non-hormonal therapies should be considered.12,40 Vasomotor symptoms can be managed with selective serotonin or norepinephrine reuptake inhibitors, such as escitalopram or venlafaxine, or with alternatives, such as gabapentin and oxybutynin. Genitourinary symptoms may respond to non-hormonal vaginal moisturizers and lubricants or newer interventions, such as vaginal laser therapy, although the latter requires further validation.
In addition to established non-hormonal therapies, novel agents targeting neurokinin-3 (NK3) and neurokonin-1 (NK1) receptors have recently emerged as effective options for vasomotor symptom control. NK3 receptor antagonists, such as fezolinetant, and NK1/NK3 receptor antagonists, such as elinzanetant, reduce hot flashes by modulating hypothalamic thermoregulatory pathways without direct estrogenic or progestogenic activity.50 Fezolinetant has demonstrated significant efficacy in reducing the frequency and severity of vasomotor symptoms and is approved in several European countries, including Switzerland.51–53 These agents represent a particularly attractive option for endometrial cancer survivors in whom systemic HRT is contraindicated or declined, although long-term safety data in oncology populations remain limited.
Special considerations
In women with Lynch syndrome (hereditary non-polyposis colorectal cancer) undergoing risk-reducing hysterectomy with BSO at a young age (35–45 years), the management of premature menopause is a common indication for HRT. In this setting, systemic estrogen-only therapy can be offered after premenopausal BSO.2,54
Patient counseling and long-term follow-up
Effective counseling is essential given the limited data from large randomized controlled trials in this population. Clinicians should provide a balanced discussion of the known benefits and theoretical risks of HRT,9 tailoring recommendations based on cancer characteristics, symptom severity, patient preference and overall comorbidity profile. Long-term follow-up with a gynecologic oncologist is recommended and should include regular physical examinations, imaging as clinically indicated and ongoing evaluation of symptom control and treatment tolerability.
Conclusions
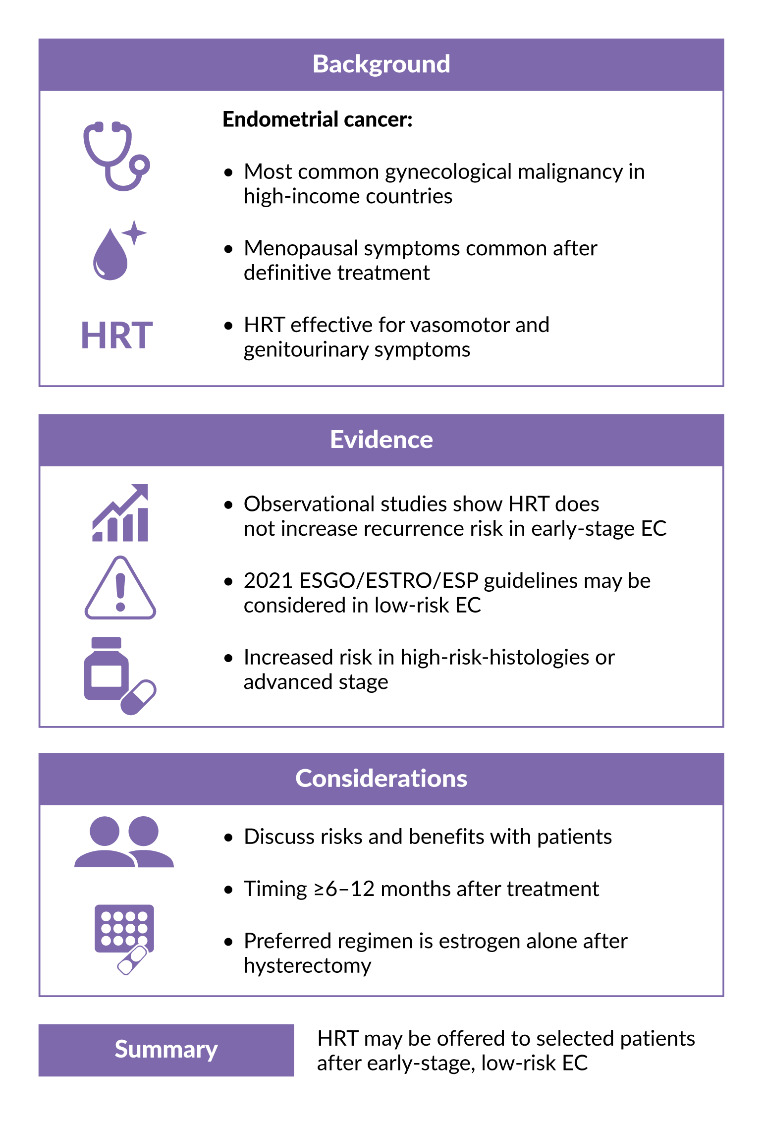
Hormone replacement therapy can be safely offered to carefully selected survivors of early-stage, low-risk endometrial cancer who suffer from significant menopausal symptoms. Current evidence, primarily from observational studies, supports the oncologic safety of estrogen-only regimens in this population. For women with advanced-stage or high-risk histologic subtypes, the absence of robust data continues to warrant a cautious approach. In all cases, treatment decisions should be guided by individualized risk assessment, symptom burden and patient preference, supported by ongoing follow-up within a multidisciplinary framework. Molecular risk stratification is likely to become increasingly relevant for individualized counseling and recommendations regarding HRT after endometrial cancer. Figure 2 summarizes the current state of evidence and outlines a practical approach to HRT use in endometrial cancer survivors.
_in_endometrial_cancer_(ec)_survivors.png)
Conflict of interest
Marcus Vetter received honoraria for consultancy from GSK, Roche, Novartis, ExactSciences, Pfizer, Stemline, AbbVie and ASC Oncology. Ursula Gobrecht-Keller received honoraria for consultancy from Astellas, Bayer and Gedeon Richter. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way.
Funding
The authors declared that no financial support was received from any organization for the submitted work.
Author contributions
Both authors contributed to and approved the final manuscript.