Introduction
Antibody-drug conjugates (ADCs) have transformed the treatment landscape of metastatic breast cancer by combining the specificity of targeted monoclonal antibodies with the potency of cytotoxic payloads.1–4 The regulatory approvals of sacituzumab govitecan (SG) for metastatic hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative breast cancer or metastatic triple-negative breast cancer (TNBC), trastuzumab deruxtecan (T-DXd) for HER2-positive, as well as HR-positive, HER2-low and HER2-ultralow disease and datopotamab deruxtecan (Dato-DXd) for HR-positive, HER2-negative subtypes have expanded therapeutic options across molecular profiles.5–7 As a result, an increasing number of patients are now eligible to receive multiple ADCs during the course of their disease.
Each ADC is defined by three key structural elements: a highly selective monoclonal antibody, a linker and a cytotoxic payload.8 They collectively determine its pharmacologic properties, therapeutic index and mechanisms of resistance. While both T-DXd and SG carry a topoisomerase I inhibitor payload, they differ in target specificity, as well as linker and payload chemistry. T-DXd consists of an anti-HER2 monoclonal antibody linked to a deruxtecan-based topoisomerase I inhibitor, whereas SG couples an anti-trophoblast cell surface antigen 2 (TROP2) antibody to the irinotecan metabolite SN-38.9,10 These molecular distinctions raise the possibility that sequential administration may retain efficacy, depending on the dominant resistance mechanisms, which can be target-related, payload-specific or pharmacokinetic.
Despite the profound clinical benefit of ADCs, there is a concern for resistance or compromised efficacy when sequencing therapies that may utilize cytotoxic payloads with similar mechanisms of action. Thus, optimal sequencing strategies remain to be defined. To date, no prospective trials have been designed to evaluate ADC sequencing in either HER2-negative or HER2-low metastatic breast cancer. Most available data come from retrospective real-world analyses and institutional cohorts, which consistently suggest that ADCs can retain some clinical activity when used sequentially, but the magnitude and duration of benefit appear modest.11–15 The median progression-free survival (PFS) on the second ADC typically ranges from two to four months, which is considerably shorter than that achieved with the first ADC.
Interpretation of these findings requires caution. Existing data are limited by small sample sizes, heterogeneous patient populations and the absence of standardized sequencing criteria or control arms. Most real-world datasets also lack detailed molecular characterization (e.g., HER2 “ultra-low” subtyping, Trop-2 expression levels or DNA damage repair biomarkers) that could refine treatment selection.
Despite these limitations, current evidence supports the feasibility of ADC sequencing in heavily pretreated HER2-low and TNBC populations, although with diminished efficacy after prior ADC exposure. Ongoing translational studies, including molecular profiling of resistance mechanisms, liquid biopsy monitoring and analysis of cross-resistance patterns, may eventually guide biomarker-driven sequencing algorithms.
This review summarizes data from published real-world studies evaluating sequential ADC use in metastatic breast cancer, highlighting efficacy and safety, resistance mechanisms and emerging biomarker insights to inform the development of rational, biomarker-driven sequencing strategies in clinical practice.
ESMO and NCCN recommendations on the use of ADCs in metastatic breast cancer
Both the ESMO Living Guidelines and the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) recognize ADCs as integral components of therapy for patients with metastatic TNBC following progression after first-line treatment, as well as those with HR-positive, HER2-negative metastatic breast cancer.
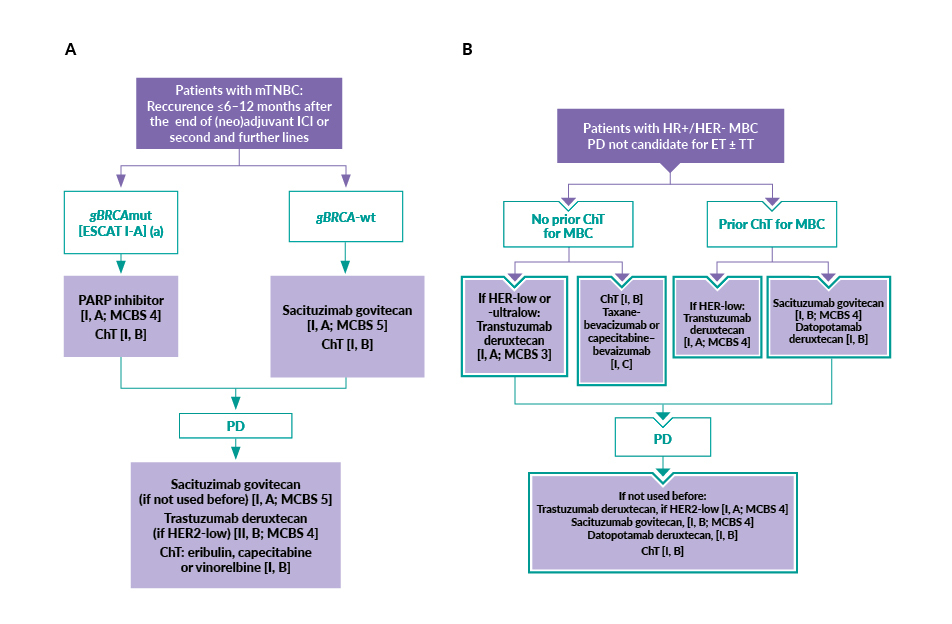
According to the ESMO Living Guidelines, SG is the preferred therapy for patients with metastatic TNBC defined by the absence of estrogen and progesterone receptor expression and HER2 expression of 0, 1+, or 2+ with ISH negativity, including HER2-low and ultralow disease, who relapse within six to twelve months after completing (neo)adjuvant immune checkpoint inhibitor therapy or as a second- or later-line option (Figure 1A).16 This recommendation is supported by a Magnitude of Clinical Benefit Scale (MCBS) score of 5, reflecting the significant survival benefit demonstrated in the ASCENT trial.1,2 In the third-line setting, ESMO recommends SG (if not used previously) (MCBS 5), T-DXd for patients with HER2-low disease (MCBS 4) or chemotherapy, depending on prior treatments and tumor biology.16
Similarly, the NCCN Guidelines recommend SG as a Category 1, preferred second-line regimen for patients with recurrent unresectable or metastatic TNBC.17 For patients in the second-line setting without a germline BRCA1/2 mutation and with HER2 immunohistochemistry (IHC) 1+ or 2+/ISH-negative tumors, T-DXd is listed as an “other recommended” second-line option.
For patients with HR-positive, HER2-negative metastatic breast cancer, the ESMO Living Guidelines recommend ADCs for those whose disease has progressed following chemotherapy and who are no longer candidates for endocrine therapy (with or without targeted therapy).18,19 In this setting, T-DXd is preferred for patients with HER2-low or ultralow disease, irrespective of prior lines of chemotherapy, while SG is recommended after at least two prior lines of chemotherapy (Figure 1B). Dato-DXd may also be considered for patients with HR-positive, HER2-negative MBC previously treated with chemotherapy in the advanced setting. Notably, however, Dato-DXd did not meet the overall survival (OS) endpoint in the TROPION-Breast01 trial,20 while both SG and T-DXd demonstrated OS benefits in phase III studies.1,4 Following progression on one ADC, another ADC not previously used may be administered, based on prior treatment history and molecular subtype.
_metastatic_triple-negative_breast_cancer_(mtnbc)_with_recurrenc.jpg)
According to the NCCN Guidelines, SG is also a Category 1, preferred second-line therapy for patients with HR-positive, HER2-negative metastatic cancer who present with visceral crisis or endocrine-refractory disease, and who are not candidates for T-DXd.17 SG is recommended for adult patients previously treated with endocrine therapy, a CDK4/6 inhibitor and at least two lines of chemotherapy, including a taxane, with at least one chemotherapy administered in the metastatic setting. SG may be considered in later treatment lines if not used as second-line therapy. By contrast, T-DXd is a Category 1, preferred treatment option for patients with HER2 IHC 1+ or 2+/ISH-negative disease who have experienced disease progression following endocrine therapy and chemotherapy.
Importantly, the 2023 ESMO Expert Consensus Statement (ECS) on the definition, diagnosis and management of HER2-low breast cancer specifically addresses sequential ADC use.21 It states that there is no biological rationale suggesting that prior treatment with T-DXd would render subsequent therapy with SG ineffective or unsafe. Therefore, prior exposure to T-DXd should not be considered a contraindication for treatment with SG and vice versa.
Real-world evidence on ADC sequencing in metastatic breast cancer
The optimal order of ADC administration in HR-positive, HER2-negative breast cancer and TNBC remains undefined, as pivotal phase III trials have largely excluded patients with prior ADC exposure and prospective data are lacking. The key outcomes of these studies are summarized in Table 1 and briefly described below.
Clinical outcomes with sequential ADC use
One of the first RWE analyses, by Huppert et al. (2025), evaluated patients with HER2-low metastatic breast cancer treated sequentially with SG and T-DXd.11 Results showed that the median time to treatment failure (TTF) was longer for the first ADC than for the second, regardless of HR status, age, visceral involvement or intervening therapy. The sequence of administration appeared to influence survival outcomes, with patients treated with SG followed by T-DXd experiencing numerically longer survival than those receiving the reverse order. Multivariable analysis identified younger age, a longer interval from diagnosis to the first ADC and receiving SG first as predictors of improved real-world OS. Interstitial lung disease (ILD)/pneumonitis occurred exclusively during T-DXd therapy (16.7%), consistent with the higher ILD rates reported in DESTINY-Breast04 compared with ASCENT or TROPiCS-02.1,3,4 A complementary retrospective study by Premji et al. (2024), which specifically evaluated the incidence of ILD in patients with HER2-low metastatic breast cancer treated with both SG and T-DXd in either sequence, showed that ILD events (16.6%) occurred only during T-DXd treatment, regardless of sequencing direction.22
Across several retrospective analyses, the second ADC consistently yielded shorter PFS than the first one, typically by around two months. In one large cohort study by Mai et al. (2024), sequencing SG and T-DXd in either order produced no statistically significant difference in PFS for the second ADC, although prior duration of benefit on the first ADC and earlier line of therapy correlated with improved outcomes.12 PFS was shorter when SG was administered as the second ADC, while T-DXd retained similar efficacy irrespective of sequence. However, the study did not stratify results by breast cancer subtype, which may limit interpretation for specific molecular subgroups.
A real-world analysis from the Moffitt Cancer Center (Joshi et al., 2025) reported consistent findings, demonstrating that while both T-DXd and SG maintain activity in patients with HER2-low metastatic breast cancer treated sequentially, PFS declines with the second ADC.13 Patients treated with T-DXd as the second ADC appeared to derive a longer benefit compared with the reverse sequence. Patients who received back-to-back ADCs achieved longer PFS than those with intervening chemotherapy.31
Similarly, Alaklabi et al. (2025) reported that SG retains clinical activity in patients with heavily pretreated metastatic TNBC and that T-DXd achieved efficacy following SG, supporting the feasibility and therapeutic potential of sequential ADC use in this population.14 However, it is important to note that none of the patients had received T-DXd before SG in this study. In the HER2-low subgroup, the median PFS with T-DXd after SG was 7 months, which is comparable to the 8.5 months reported in the DESTINY-Breast04 study for HR-negative disease.4 Approximately one-third of patients who benefited from SG also responded to subsequent T-DXd, whereas none who were refractory to SG derived benefit.
A study by Raghavendra et al. (2024) reported comparable survival outcomes with the two ADCs, regardless of sequence, although the median OS was numerically longer when SG was administered first.23 Another large multicenter study confirmed that sequential ADC use in HER2-low metastatic breast cancer yields modest efficacy, with a median PFS2 of approximately 2–3 months and OS under eight months, with similar results across HR subgroups.24,32 T-DXd as the second ADC showed a numerical trend toward improved PFS2, but cross-resistance between ADCs sharing topoisomerase I inhibitor payloads remained a major challenge. Primary resistance was observed in approximately 40% of patients treated with the first ADC and 60% of patients treated with the second ADC, including half of those with secondary resistance to the first ADC. Data also showed that intervening therapies between two ADCs shorten PFS2 (with, 2.6 months; without, 3.1 months).
Real-world experience from Nezirevic et al. (2025) also confirmed the clinical activity of SG and T-DXd in patients with heavily pretreated HER2-negative metastatic breast cancer, including those with brain metastases.15 However, efficacy declined when ADCs were administered sequentially, with the median PFS reduced to approximately 3–4 months for the second ADC. The median PFS was slightly longer when SG was received as first ADC compared with second ADC.
Recently, a retrospective observational study utilizing the Flatiron Health electronic health record database demonstrated poorer outcomes to T-DXd in patients previously treated with SG.26 While providing valuable large-scale RWE on the sequential use of ADCs in metastatic breast cancer, this study had notable limitations, including restricted sequencing direction (only SG to T-DXd), incomplete covariate adjustment, small subgroups and ignored confounders (e.g., age, ECOG, brain metastases). Interestingly, high rwPFS with chemotherapy after T-DXd, especially in patients HR-positive, HER2-negative disease, raises concerns about selection bias or modeling inconsistencies.
Cross-resistance and mechanistic insights
Abelman et al. (2024) provided mechanistic evidence of ADC cross-resistance.27 In their study, resistance to a second ADC occurred in approximately half of the patients and depended on both antibody target and payload. Specifically, cross-resistance was 49% when both target and payload changed, 57% when only the payload changed, 30% when only the target changed and 67% when neither changed. Changing both the antibody and payload was therefore associated with improved outcomes on subsequent ADCs. This study also showed differences in subtype-specific outcomes, with sequencing SG before T-DXd resulting in longer PFS in both HR-positive, HER2-negative and TNBC populations, while T-DXd followed by SG was less effective, particularly in HR-positive, HER2-negative disease. Whole-exome sequencing revealed candidate resistance mutations in TOP1, TOP2A, TOP3A and TOP3B, suggesting that alterations in topoisomerase-related genes may mediate resistance to ADCs with topoisomerase I inhibitor payloads. These findings support a mechanistic rationale for cross-resistance between ADCs such as SG and T-DXd, which share this payload class.
Molecular and biomarker-based correlates
Data on biomarkers predictive of response to ADC in metastatic breast cancer remain limited, but emerging data suggest prognostic potential. Morganti et al. (2025) analyzed a ctDNA-based classifier (DNADX) that stratifies tumors into five molecular subtypes (X0–X4).28 Results from study demonstrated that sequencing direction (anti-Trop-2 to anti-HER2 or vice versa) did not affect time to next treatment (TTNT), including across HR subtypes. DNADX clusters correlated with OS, highlighting the potential of ctDNA-based molecular signatures for prognostic refinement in patients with HER2-negative metastatic breast cancer receiving sequential ADC therapy. In this cohort, most patients received anti-Trop2 ADC therapy first, followed by an anti-HER2 ADC.
A multicenter real-world next-generation sequencing (NGS)-based analysis further characterized the genomic landscape of HER2-low metastatic breast cancer treated sequentially with T-DXd and SG.29 Distinct mutational profiles were observed: PIK3CA, TP53 and ESR1 mutations dominated in HR-positive disease, while TP53 mutations were highly prevalent in HR-negative tumors. This study demonstrated that time from diagnosis and prior treatment burden, rather than ADC sequence, were the main clinical factors influencing OS outcomes. No association was observed between TP53 or PIK3CA status and real-world OS from ADC initiation. These findings highlight the genomic heterogeneity of HER2-low metastatic breast cancer and underscore the need for biomarker-driven strategies to optimize sequencing and resistance management for ADC therapies.
HER2 expression and HR subtype-specific sequencing effects
A large real-world analysis of patients with HER2-negative metastatic breast cancer stratified by HER2 expression (HER2-low, HER2-ultra-low and HER2-null) identified subtle subtype-specific differences in clinical outcomes with sequential ADCs.30,33 Among HR-negative, HER2-null patients, the SG to T-DXd sequence yielded significantly longer time-on-treatment 2 and improved OS, while T-DXd to SG offered a modest benefit in HER2-low disease. In HR-positive (HER2-null and HER2-low) patients, outcomes were similar regardless of sequence. HER2-low tumors were more common among those receiving T-DXd first (45%), while HER2-null predominated among those starting with SG (42%). These findings suggest that HER2 expression level and HR status may influence sequencing efficacy and warrant biomarker-integrated confirmation.
Ongoing studies on ADC sequencing
Several ongoing and recruiting studies are actively investigating the sequencing of ADCs in patients with metastatic breast cancer. These studies aim to optimize treatment strategies following prior ADC exposure, elucidate mechanisms of resistance and identify biomarkers predictive of response. The SATEEN study,34 SERIES study,35,36 study on genomic and transcriptomic predictors of sequential SG sensitivity after T-DXd in ER+/HER2-low metastatic breast cancer (NCT06665178)37 and the ENCORE registry study38 are evaluating the clinical activity, molecular determinants and real-world outcomes associated with the sequential use of SG. Table 2 provides an overview of these ongoing and recruiting studies. Furthermore, an ongoing phase II TRADE-DXd trial evaluates sequencing of T-DXd versus Dato-DXd, the ADCs that share the same payload.39
Conclusion
To date, no prospective study has evaluated the clinical outcomes of ADC sequencing in HR-positive, HER2-negative metastatic breast cancer or TNBC. Current knowledge is largely derived from retrospective, real-world analyses involving heterogeneous patient populations, diverse tumor subtypes and varying treatment lines.11–15,22,28,29 These studies consistently suggest that ADCs can retain antitumor activity when used sequentially, although efficacy is diminished and cross-resistance frequently emerges, particularly between agents sharing topoisomerase I inhibitor payloads.
Interpretation of these findings requires caution due to inherent limitations in the available evidence. Real-world cohorts often include mixed tumor types, lack consistent stratification by line of therapy and differ in intervening treatments between the first and second ADC. Moreover, sample sizes are modest, control arms are absent and data maturity varies, which altogether complicates the assessment of comparative benefit. Nevertheless, emerging evidence indicates that SG tends to maintain greater activity when administered before T-DXd in HR-negative, HER2-null disease, while the reverse sequence may yield modest benefit in HER2-positive and HER2-low disease.
It should be emphasized that the current body of evidence does not demonstrate that sequential use of ADCs is superior to conventional chemotherapy for most patients. In addition, ADC therapy may, in some cases, exert a greater negative impact on quality of life than single-agent chemotherapy. Therefore, ADC sequencing should not be regarded as an appropriate strategy for all patients and requires careful, individualized consideration.
In addition to sequencing an anti-Trop2 ADC followed by an anti-HER2 ADC and the reverse strategy, the sequence of trastuzumab emtansine (T-DM1) followed by T-DXd is likely to gain relevance as T-DXd moves into earlier treatment settings. This sequence has demonstrated clinically meaningful activity, with consistent evidence of PFS benefit, likely indicating the therapeutic advantage of administering a second-generation ADC after prior exposure to a first-generation agent.26,40 In contrast, clinical data on the reverse sequence remain limited. However, this question is expected to become important as more patients receive neoadjuvant T-DXd. In such cases, patients who do not achieve a pathological complete response and lack more effective alternatives may subsequently be considered for adjuvant T-DM1.
Beyond resistance to the payload, emerging translational and real-world data indicate that exposure to T-DXd may lead to the downregulation or complete loss of HER2 expression in a substantial proportion of tumors.41,42 This phenomenon has important implications for treatment sequencing, as reduced target availability may compromise the efficacy of subsequent HER2-directed therapies, including T-DM1 and other HER2-based ADCs. In the context of earlier-line or neoadjuvant use of T-DXd, this biological effect becomes particularly relevant: patients who fail to achieve pathological complete response may present with diminished HER2 expression at residual disease, potentially limiting the benefit of adjuvant HER2-targeted strategies. These observations underscore the need for reassessment of HER2 status after T-DXd exposure and raise caution regarding very early deployment of T-DXd outside established indications, especially in curative-intent settings, where preservation of downstream HER2-directed options remains clinically meaningful.
In current clinical practice, sequencing decisions are individualized and guided by clinical judgment and guideline recommendations. Both ESMO and NCCN position SG and T-DXd as complementary agents within the treatment continuum of HER2-negative metastatic breast cancer, which also includes the HER2-low group. Based on the available evidence, SG is the preferred choice as the primary ADC in metastatic TNBC which includes all levels of HER2 negativity (HER2-null, ultralow and low). In endocrine-refractory disease with detectable HER2 expression, evidence clearly points towards the choice of T-DXd as the primary ADC, while permitting sequential use based on prior exposure and disease biology. Clinicians also weigh prior response duration, toxicity considerations (e.g., risk of interstitial lung disease with T-DXd versus hematologic toxicity with SG), antigen expression and local access or reimbursement constraints.
The growing recognition of payload-specific resistance mechanisms and differential antigen expression further highlights the need for biomarker-driven sequencing strategies. Genomic profiling, ctDNA-based molecular signatures and HER2 expression subtypes are emerging as tools to improve patient selection, guide treatment order and mitigate cross-resistance.
Conflict of interest
Marcus Vetter received honoraria for consultancy from GSK, Roche, Novartis, Exact Sciences, Pfizer, Stemline, AbbVie and ASC Oncology. Benjamin Müller received honoraria from AbbVie for advisory activities and congress participation support from Daiichi Sankyo. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way.
Funding
The preparation of the article was supported by Gilead Sciences Switzerland Sàrl. The sponsor did not have any role in the development of the manuscript and did not influ-ence its content in any way.
Author contributions
The authors created and approved the final manuscript.