Introduction
Diffuse large B-cell lymphoma (DLBCL) accounts for approximately 30% of all lymphoma cases and is characterized by substantial pathologic, molecular and clinical heterogeneity.1 In newly diagnosed disease, standard first-line therapies include rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone (R-CHOP) or polatuzumab vedotin combined with rituximab, cyclophosphamide, doxorubicin and prednisone (Pola-R-CHP), with dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide and doxorubicin plus rituximab (DA-EPOCH-R) recommended for double- and triple-hit lymphomas.2 Despite these approaches, approximately 30–40% of patients do not respond to first-line therapy or relapse after initial remission. For those with primary refractory disease or early relapse (<12 months), chimeric antigen receptor (CAR) T-cell therapy is the recommended second-line option, whereas patients with late relapse typically receive salvage therapy followed by autologous stem cell transplantation (ASCT) if a response is achieved. For patients ineligible for CAR T-cell therapy, available regimens include rituximab, gemcitabine and oxaliplatin (R-GemOx) or polatuzumab vedotin, bendamustine and rituximab (Pola-BR) and glofitamab plus GemOx3 has emerged as a promising option for patients unable to undergo ASCT.
Axicabtagene ciloleucel (axi-cel) and lisocabtagene maraleucel (liso-cel) are approved for second-line DLBCL based on the registrational phase III ZUMA-7 and TRANSFORM trials, each of which met its primary endpoint of event-free survival (EFS).4,5 At a median follow-up of 47.2 months, axi-cel demonstrated superior overall survival (OS) compared with standard of care (SoC) platinum-based chemotherapy (4-year OS rates, 54.6% vs 46.0%; HR: 0.73 [95% CI: 0.54–0.98]; p=0.03), with the median OS not reached with axi-cel versus 31.1 months with SoC.6 At the 3-year follow-up of TRANSFORM, OS numerically favored liso-cel over SoC (63% vs 52%; HR: 0.757 [95% CI: 0.481–1.191]).7 Retrospective analyses have attempted to compare the two products in terms of efficacy and safety, but their interpretations remained limited by methodological biases.8
Operational considerations often guide treatment selection. Axi-cel has a consistently short manufacturing time (approximately 17 days) and real-world data show significantly shorter vein-to-vein time compared with liso-cel (57 days vs 81 days; p<0.001).8,9 As a result, axi-cel has been the preferred option for patients with rapidly progressive disease. In contrast, liso-cel is associated with a lower incidence of grade ≥3 immune effector cell-associated neurotoxicity syndrome (ICANS) and is therefore favored in older or frail patients with comorbidities. Nevertheless, these observations should be interpreted with caution, as no head-to-head comparison is available and the management of side effects, including cytokine release syndrome (CRS) and ICANS, as well as manufacturing timelines, has evolved and continues to change.
Despite the growing body of evidence supporting CAR T-cell therapy in DLBCL, major knowledge gaps persist. Patients with Richter’s syndrome and those with active central nervous system (CNS) involvement, including CNS post-transplant lymphoproliferative disorder (PTLD), have been excluded from pivotal CAR T-cell trials due to their aggressive disease course, poor performance status, increased neurological risk and historically inferior outcomes.10–13 As a result, prospective data in these high-risk settings are lacking, leaving clinicians with limited guidance on the safety, efficacy and real-world applicability of CAR T-cell therapy for these populations.
In this report, we present two cases illustrating the clinical benefit of CAR T-cell therapy in patients with high-risk DLBCL. The first describes an elderly patient with Richter’s transformation and rapidly progressive DLBCL who achieved a rapid and sustained complete response following axi-cel infusion. The second case highlights a heavily pretreated patient with CNS PTLD who achieved complete remission with liso-cel.
Case 1: Sustained complete remission with axi-cel in a patient with rapidly progressive DLBCL
A 64-year-old male patient was diagnosed with chronic lymphocytic leukemia (CLL) in March 2017. In August 2023, he presented with spontaneous splenic rupture and was diagnosed with stage IV DLBCL, consistent with Richter’s transformation.
The patient received one cycle of R-CHOP followed by two cycles of Pola-R-CHP but developed progressive disease, predominantly involving an enlarging abdominal mass. After discussion at a multidisciplinary tumor board, he was deemed a candidate for CAR T-cell therapy.
Given the rapid clinical progression and after lymphapheresis, bridging therapy was initiated with three cycles of GemOx, followed by lenalidomide (25 mg), added as a salvage option for proven chemoimmunorefractory disease, starting in November 2023. The patient also received radiotherapy (2 Gy twice) for symptomatic abdominal pain.
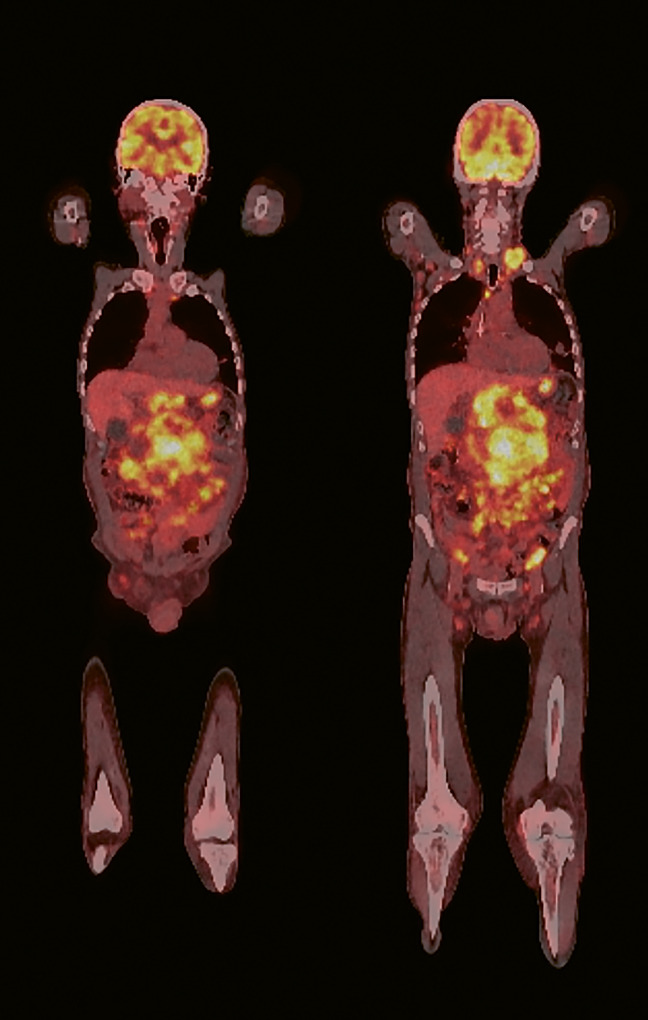
In December 2023, a positron emission tomography-computed tomography (PET-CT) scan revealed a highly metabolically active abdominal bulk (Figure 1). At that time, his Eastern Cooperative Oncology Group (ECOG) performance status was 3. He subsequently underwent lymphodepleting chemotherapy with fludarabine (30 mg/m2) and cyclophosphamide (500 mg/m2), followed by infusion of axi-cel.
_scan_seven_days_prior_to_the_ini.png)
Within 24 hours of axi-cel infusion, the patient experienced grade 2 CRS and grade 3 ICANS according to the American Society for Transplantation and Cellular Therapy (ASTCT) criteria.14 He received prophylactic anakinra (100 mg) every 12 hours from the day of infusion and every six hours upon the diagnosis of ICANS, along with a single dose of tocilizumab (550 mg). Anakinra, an interleukin-1 receptor antagonist, was used based on the study by Park et al. (2023),15 in which it was associated with a low incidence of ICANS in patients receiving anti-CD19 CAR T-cell therapy, and because of the high tumor volume. The patient also developed immune effector cell-associated hematotoxicity (ICAHTl; CAR-HEMATOTOX score16 ≥2) and hypogammaglobulinemia.
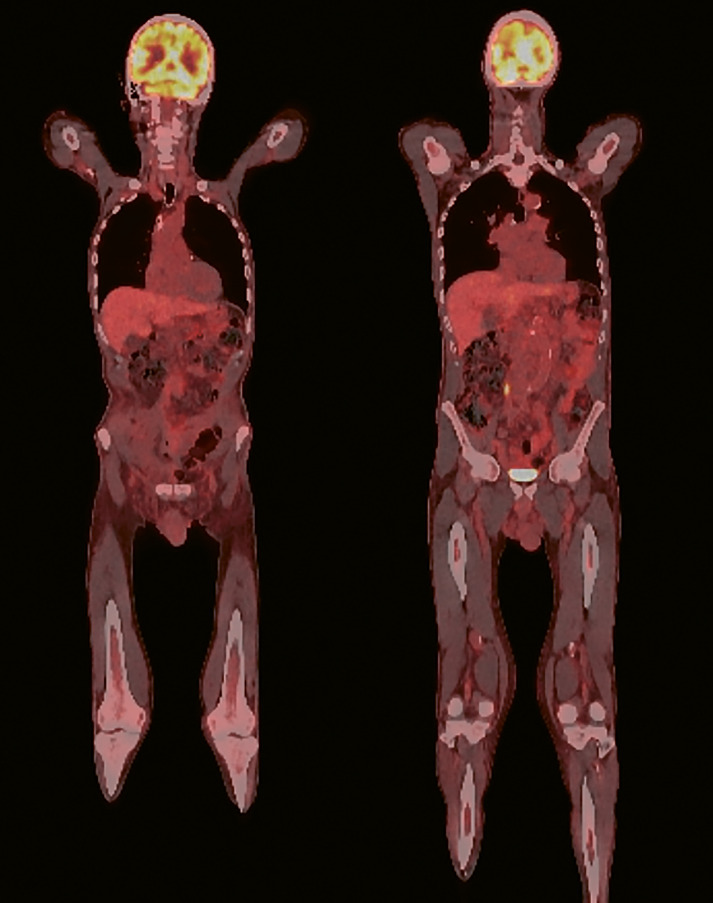
Despite these complications, the patient achieved a complete metabolic remission (CR) one month after CAR T-cell therapy (Figure 2), which has been sustained at 18 months.
_scan_30_days_after_car_t-cell_in.png)
Case 2: Successful treatment of PTLD with liso-cel
A 24-year-old male patient initially underwent kidney transplantation in 2000 for reflux nephropathy and hydronephrosis and subsequently received immunosuppression with tacrolimus, mycophenolate mofetil and prednisone. In March 2006, he was diagnosed with stage IIa PTLD, which was negative for Epstein-Barr virus (EBV). First-line management included reduction of immunosuppression and rituximab monotherapy in April 2006, followed by R-CHOP between May and July 2006, which resulted in CR.
Following a second kidney transplant due to graft failure and immunosuppression in 2015, the patient developed de novo stage IIa (iliac bulk) EBV-negative PTLD in March 2019 which was clonally unrelated to the prior PTLD episode, as confirmed by B-cell receptor rearrangement. He received six cycles of DA-EPOCH-R (without vincristine) followed by radiotherapy (36 Gy) and he again achieved CR.
In October 2024, the patient presented with a generalized seizure. Magnetic resonance imaging (MRI) revealed multiple supratentorial hyperintense lesions and brain biopsy confirmed EBV-negative PTLD involving the CNS. Immunosuppression was discontinued except for low-dose prednisone (5 mg) and treatment with methotrexate, cytarabine and rituximab was initiated between November and December 2024. The patient achieved CR, confirmed by MRI and PET-CT.
Despite dilated cardiomyopathy (ejection fraction 48%; nadir 30%) and multiple cardiovascular risk factors, multidisciplinary evaluation supported the use of CAR T-cell therapy. In January 2025, the patient received lymphodepletion with dose-reduced fludarabine and cyclophosphamide followed by infusion of liso-cel.
Early post-infusion complications included a port infection with Corynebacterium amycolatum and thrombosis of the left subclavian vein. No CRS or ICANS occurred. The patient developed ICAHT (CAR-HEMATOTOX score ≥2) that required platelet transfusion and granulocyte colony-stimulating factor (G-CSF) administration, as well as hypogammaglobulinemia managed with intravenous immunoglobulin (IVIG). He also experienced viral respiratory tract infection.
The patient achieved CR, which was maintained at follow-up. He remains off immunosuppression, with a creatinine clearance of 48 mL/min.
Discussion
Richter’s syndrome, defined as the transformation of CLL or small lymphocytic lymphoma (SLL) into an aggressive lymphoma, most frequently DLBCL, occurs in approximately 2–10% of patients with CLL and is associated with a poor prognosis.17,18 CR rates after chemoimmunotherapy do not exceed 20% and the median OS is only 6–12 months. Given the aggressive disease course and rapid clinical deterioration, patients with Richter’s syndrome are often excluded from DLBCL trials, including key CAR T-cell studies.10–12 Nevertheless, emerging real-world evidence suggests that CAR T-cell therapy, particularly axi-cel, can provide clinically meaningful outcomes in this population. A large CIBMRT registry analysis of 140 patients with Richter’s syndrome, with two-thirds receiving axi-cel, reported a CR rate of 57% and a 2-year OS rate of 46.6%.19
Our first case aligns with these observations. Despite a high tumor burden, rapid disease progression, and poor (lymphoma-related) performance status, the patient achieved early and sustained complete remission following axi-cel infusion. The clinical course shows the ability of axi-cel to induce deep and sustained responses even in patients with chemo-refractory, rapidly progressing disease and underscores the importance of timely referral to CAR T-cell therapy in those with Richter’s syndrome. As expected, toxicity was pronounced in our patient, given his disease course and high tumor burden, which is a known risk factor for CRS and/or ICANS,20 but these complications were anticipated and effectively managed. The sustained remission observed at 18 months further supports axi-cel as a highly active therapeutic option in this otherwise poor-prognosis setting. Our findings contribute to the growing evidence supporting CAR T-cell therapy for Richter’s syndrome.
PTLD is another uncommon but challenging lymphoma subtype that arises due to immunosuppression after solid organ transplantation.21 For patients with relapsed or refractory disease, the optimal treatment strategy remains unclear, with limited data on the use of CAR T-cell therapy. A multicenter retrospective study reported outcomes comparable to those achieved with axi-cel in the ZUMA-1 trial and liso-cel in the TRANSCEND NHL 001 trial, with an ORR of 64%, a CR rate of 55% and a 2-year OS rate of 58%.21 Most patients were kidney transplant recipients and axi-cel was the most frequently used CAR T-cell therapy, reflecting its wide use and established efficacy. The management of immunosuppression before lymphapheresis, during and after CAR T-cell treatment remains a key challenge in PTLD, requiring a careful balance between preventing graft rejection and reducing the risk of relapse.
In our second case, we selected liso-cel because the TRANSCEND study included patients with secondary CNS involvement and demonstrated durable responses in this population.22,23 Registry data also support liso-cell activity in secondary CNS lymphoma, with response rates and survival outcomes comparable to those observed in systemic disease and with a relatively favorable neurotoxicity profile.24 Axi-cel has similarly demonstrated meaningful real-world activity in secondary CNS lymphoma, with response rates exceeding 70% but with a higher incidence of neurotoxicity.25 Notably, a meta-analysis suggests that CAR T-cell therapy is both feasible and effective in both primary and secondary CNS lymphoma and does not appear to confer an increased risk of severe ICANS.22 Our case is consistent with these reports and highlights the feasibility of CAR T-cell therapy in a post-transplant patient with CNS involvement. Despite substantial comorbidities and prior immunosuppression, liso-cel was administered safely, with manageable hematologic and infectious complications and without CRS or ICANS.
Conclusion
These case reports highlight the therapeutic potential of CAR T-cell therapy in rare but highly aggressive lymphoma settings. Despite high tumor burden, poor performance status and CNS involvement, our patients achieved rapid, deep and sustained remissions with axi-cel and liso-cel. The observed responses demonstrate that CAR T-cell therapy is feasible even in these high-risk patients, when supported by multidisciplinary evaluation and proactive toxicity management. These reports further emphasize the importance of timely referral and individualized selection based on disease biology and course, as well as patient-specific risk factors. Together, these findings add to the growing real-world evidence suggesting that CAR T-cell therapy may provide a valuable treatment option for patients with Richter’s transformation and CNS-involved PTLD.
Ethics approval and consent to participate
Written consent for the further use of patient data was obtained.
Consent for publication
Consent for publication was obtained.
Availability of data and materials
All patient data that support this case report are included in the anonymized form in the published article.
Conflict of interest
The authors declared that the study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors declared that no financial support was received from any organization for the submitted work.
Authors contributions
All authors contributed to and approved the final manuscript.