
Dear Colleagues,
Among all genitourinary malignancies, muscle-invasive bladder cancer (MIBC) is arguably the “winner” in 2025 when it comes to therapeutic progress. Two landmark phase III trials, KEYNOTE-905/EV-303 and IMvigor011, were presented at the European Society for Medical Oncology (ESMO) 2025 Congress and highlighted at the Swiss Oncology and Hematology Congress (SOHC). In particular, for the patient population addressed in KEYNOTE-905 — cisplatin-ineligible — this trial has delivered long-awaited advances to those historically underserved.
A breakthrough for cisplatin-ineligible patients
Cisplatin-ineligible patients represent roughly 50% of the MIBC population and, as neoadjuvant cisplatin-based chemotherapy was the gold standard for decades, this group was long considered the “forgotten half of MIBC patients.” The 2022 ESMO guidelines essentially recommend upfront radical cystectomy with pelvic lymphadenectomy or trimodal treatment, with perioperative therapy largely restricted to clinical trials.1 This changed with the KEYNOTE-905/EV-303 trial, which evaluated perioperative enfortumab vedotin (EV) plus pembrolizumab versus cystectomy alone in cisplatin-unfit or cisplatin-declining patients.2,3
The trial demonstrated unprecedented improvements in both event-free and overall survival (OS), reducing the risk of recurrence, progression or death by approximately 60% and the risk of death by about 50% compared with surgery alone. Importantly, the addition of EV plus pembrolizumab did not compromise the execution of the planned radical cystectomy and benefits were consistent across subgroups. These results position perioperative EV plus pembrolizumab as a potential new standard of care for this so far systemic treatment-wise unserved high-risk population, although the regimen remains off-label pending regulatory decisions. Toxicity, thus well-known from first-line metastatic urothelial carcinoma treatment, warrants careful management, as many cisplatin-ineligible patients are older and frail, which underscores the need for multidisciplinary care.
Several questions remain. With a pathologic complete response rate of approximately 57%, the possibility of bladder preservation for selected responders is appealing but requires reliable biomarkers or imaging-based assessments. It is also unclear whether all patients need the full course of adjuvant EV and pembrolizumab. Treatment de-escalation for responders is an important focus for future research. Clinical trials are ongoing addressing the rate of of bladder preservation as an endpoint; thus, the term “clinical complete response” (cCR) after neoadjuvant treatment needs validation. A proposal from a consensus definition was recently published by Necchi et al.4 Meanwhile, established alternatives, including adjuvant nivolumab from CheckMate 274 and perioperative durvalumab plus chemotherapy from NIAGARA, remain relevant options in selected patients.5–7
The role of post-cystectomy ctDNA in guiding adjuvant therapy for MIBC
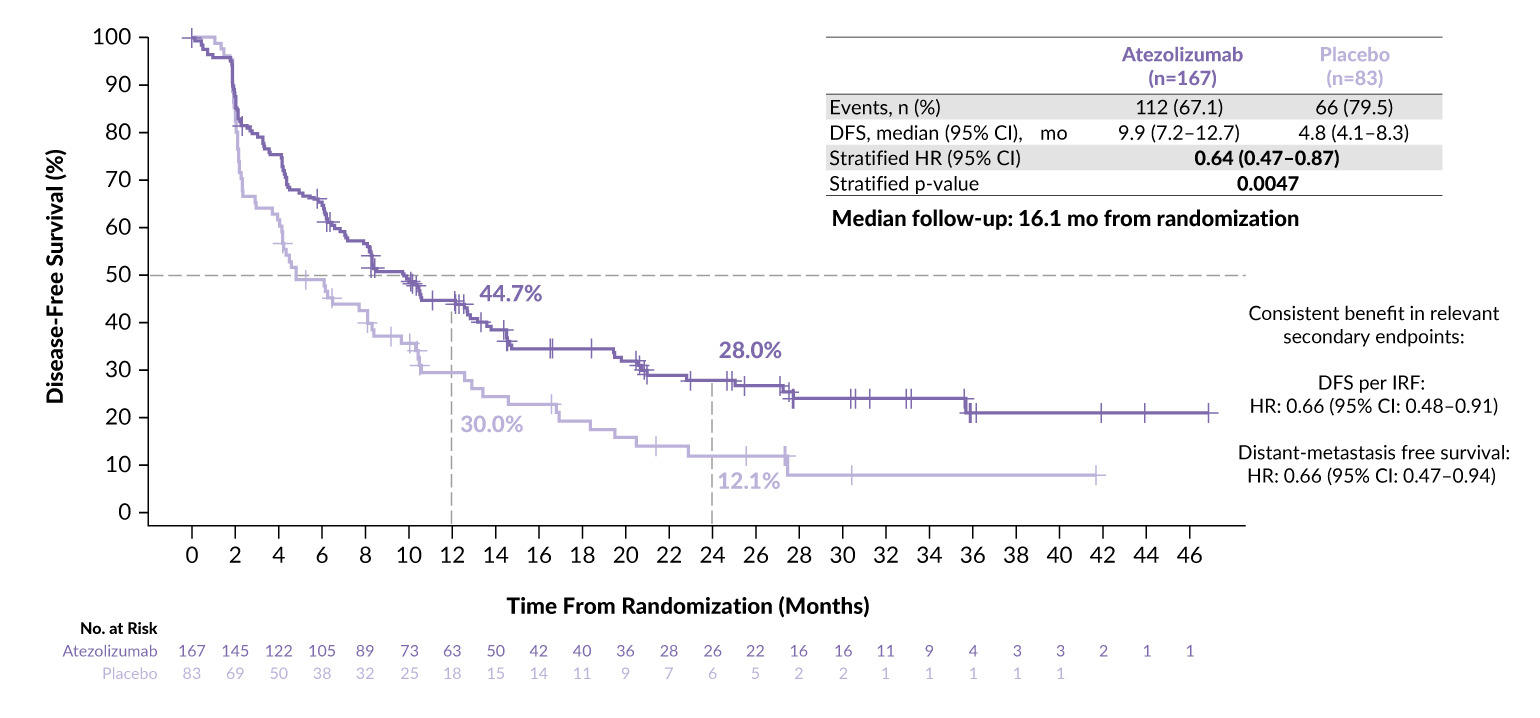
The role of circulating tumor DNA (ctDNA) in guiding adjuvant therapy has gained attention with the phase III IMvigor011 trial, which is the first randomized ctDNA-guided study to demonstrate a survival benefit in bladder cancer.8–10 In this study, patients with high-risk MIBC were tested for ctDNA following cystectomy; those who were ctDNA-positive at baseline were randomized to receive atezolizumab or placebo, while repeatedly ctDNA-negative patients entered active surveillance.
With a median follow-up of 21.8 months, ctDNA-negative patients showed remarkably low recurrence and mortality rates, suggesting that many can be safely spared adjuvant therapy.8 In contrast, ctDNA-positive patients experienced clear improvements in disease-free survival (Figure 1) and OS with one year of adjuvant atezolizumab, providing the first level 1 evidence that minimal residual disease should guide postoperative treatment decisions in MIBC. These findings confirm earlier observation from the IMvigor010 study11,12 and are consistent with results from CheckMate-274 and NIAGARA, all showing ctDNA negativity as a strong marker of favorable prognosis.5,13
Although atezolizumab is not currently approved for adjuvant therapy in MIBC, IMvigor011 marks an important step toward biomarker-driven perioperative management. The trial also opens the door for further advances, including minimal residual disease (MRD)-guided escalation and de-escalation strategies now being explored in clinical studies.14,15
_in_patients_who_tested_posit.png)
Looking ahead
In summary, 2025 marks a turning point for MIBC, with perioperative EV plus pembrolizumab offering the first truly effective systemic option for cisplatin-ineligible patients and IMvigor011 establishing ctDNA as a clinically meaningful tool to guide postoperative therapy. The upcoming phase III EV-304 trial investigating EV plus pembrolizumab perioperatively in cisplatin-eligible patients — if positive — will render the perioperative setting potentially platinum-free. Together, these advances move MIBC toward a more personalized, biology-driven treatment paradigm, where intensified therapy is directed to those who need it most and unnecessary drug-related and financial toxicity can be avoided in those who do not. The field is rapidly evolving towards a more precise and patient-tailored care, with ongoing trials refining biomarkers, exploring bladder-preserving strategies and testing MRD-guided escalation and de-escalation.

PD (AUT) Dr Ursula Vogl
Editor-in-Chief
Senior physician oncologist
Oncology Institute of Southern Switzerland and
Ente Ospedaliero Cantonale
Bellinzona, Switzerland
Email: ursula.vogl@eoc.ch
Conflict of interest
The author received advisory board and speaker honoraria from the following entities. Private: Astellas, healthbook and Bayer; institutional: Roche, Janssen, Bayer, Merck, MSD, BMS, Pfizer, Novartis AAA, SAMO, ESMO, ESO and healthbook. Grant funding: Fond’Action Contre le cancre.
Funding
The author has declared that no financial support was received from any organization for the submitted work.
Author contributions
The author has created and approved the final manuscript.