First-line therapy in metastatic breast cancer: Standard of care
Breast cancer is a heterogeneous disease with distinct subtypes defined by molecular and histopathological characteristics, including human epidermal growth factor receptor 2 (HER2) expression, hormone receptor (HR) status and specific genomic alterations such as PIK3CA, AKT1, PTEN, ESR1, germline BRCA1/2 and PALB2 mutations.1,2 First-line systemic therapy for breast cancer has historically been guided by these molecular features. The regimens summarized below reflect the internationally accepted standard of care until the beginning of 2025. However, as discussed in the following sections, emerging data from first-line trials of antibody-drug conjugates (ADCs) and novel targeted combinations are beginning to challenge and potentially reshape these long-standing treatment paradigms.
At the diagnosis of metastatic disease, comprehensive genomic testing is essential to inform therapy selection.1,3 In routine practice, this includes assessment of HER2, HR and progesterone receptor (PgR) status, together with germline BRCA1/2 and PALB2 testing. In patients with HR-positive, HER2-negative disease, evaluation of HER2-ultralow status, as well as somatic profiling for PIK3CA, AKT1/PTEN and ESR1 (after treatment with aromatase inhibitor [AI]) mutations should be performed. For patients with triple-negative breast cancer (TNBC), programmed cell death ligand 1 (PD-L1) status is required to guide immunotherapy. In patients with HER2-negative disease, HER2-low status should be determined. When corresponding therapies are available, additional biomarker testing, such as high microsatellite instability (MSI-H) and mismatch repair deficiency (dMMR), high tumor mutation burden (TMB-H), NTRK fusions, BRAF mutations and RET fusions, should be performed.
Circulating tumor DNA (ctDNA) analysis is increasingly used as a complementary tool for detecting certain mutations, monitoring molecular evolution during therapy and identifying resistance mechanisms. According to the European Society for Medical Oncology (ESMO) clinical practice guidelines, genomic profiling and further diagnostic tests (e.g. on tumor tissue or ctDNA) should only be carried out as part of routine clinical practice if the result will change the treatment approach, as guided by the ESCAT scale or if the patient has access to appropriate clinical trials.1,2
This molecular information plays an important role in guiding treatment.1,2 In HER2-positive breast cancer, taxane-based chemotherapy combined with the HER2-directed antibodies trastuzumab and pertuzumab (THP) has remained the standard first-line treatment for over 13 years, supported by results from the phase III CLEOPATRA trial.1,4 For patients with HR-positive, HER2-negative breast cancer, the combination of a cyclin-dependent kinase 4/6 inhibitor with endocrine therapy (ET) is well-established in those with de novo metastatic disease or relapse more than 12 months after completing adjuvant ET.1,2 In patients with endocrine resistance and a confirmed PIK3CA mutation, which is present in approximately 40% of cases, treatment with inavolisib, fulvestrant and palbociclib is recommended, based on results from the phase III INAVO120 trial.1,2,5–7 This triplet regimen has recently received approval in Switzerland.8 If no PIK3CA mutation is detected in the endocrine-resistant situation, fulvestrant in combination with a cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitor remains the preferred option.
For TNBC, treatment selection is based on PD-L1 expression status, positive in approximately 40% of cases when tested by the SP142 antibody clone (immune-cell [IC] PD-L1 expression ≥1% of tumor area) and the presence of a germline BRCA mutation.1,2,9,10 Until recently, for patients with a combined positive score (CPS) of ≥10 as determined by the 22C3 antibody clone, pembrolizumab plus chemotherapy is the recommended first-line regimen, supported by the phase III KEYNOTE-355 trial, which demonstrated significantly improved both progression-free survival (PFS) and overall survival (OS) compared with chemotherapy alone.9,11 Atezolizumab combined with nab-paclitaxel is another option based on the findings from the IMpassion130 trial.1,2,10 Patients with PD-L1 IC ≥1% and disease-free interval >12 months are eligible for this regimen. For patients with PD-L1-negative tumors and a germline BRCA mutation, poly (ADP-ribose) polymerase (PARP) inhibitors such as olaparib and talazoparib are preferred (in Switzerland, however, they are approved only for patients who have previously received an anthracycline and/or a taxane unless contraindicated in the neoadjuvant, adjuvant or locally advanced/metastatic setting)12,13; otherwise, chemotherapy remains the standard approach. Despite these advances, TNBC remains associated with poor prognosis. Notably, real-world data indicate that only approximately half of the patients proceed to second-line therapy, with a median OS in the first-line setting limited to 11.3 months.14
The ADCs, including trastuzumab deruxtecan (T-DXd),15–17 sacituzumab govitecan (SG)18,19 and datopotamab deruxtecan (Dato-DXd),20–22 has significantly shifted the treatment paradigm for metastatic breast cancer, particularly in later lines of therapy.1,2,23 Research efforts are ongoing to explore the use of these ADCs in earlier treatment settings. Several important studies in the first-line setting have been recently published and presented at international meetings. This review highlights the most practice-relevant studies and emerging concepts likely to influence future clinical approaches, with a particular focus on their implications for Swiss oncology practice.
Emerging therapeutic approaches in first-line treatment
Targeted treatment
HR-positive, HER2-negative breast cancer with ESR1 mutation: The SERENA-6 trial demonstrates an improved PFS with camizestrant plus CDK4/6 inhibitor
Approximately 70% of breast cancers are estrogen receptor (ER)-positive and HER2-negative.24 The ER is encoded by the ESR1 gene and hotspot ESR1 mutations lead to ligand-independent, constitutive activation of the receptor. While ESR1 mutations are rare (<5%) at the time of diagnosis of advanced breast cancer, they frequently emerge during first-line treatment with an aromatase inhibitor (AI) plus CDK4/6 inhibitor, detected in approximately 40% of patients at the time of disease progression.25,26
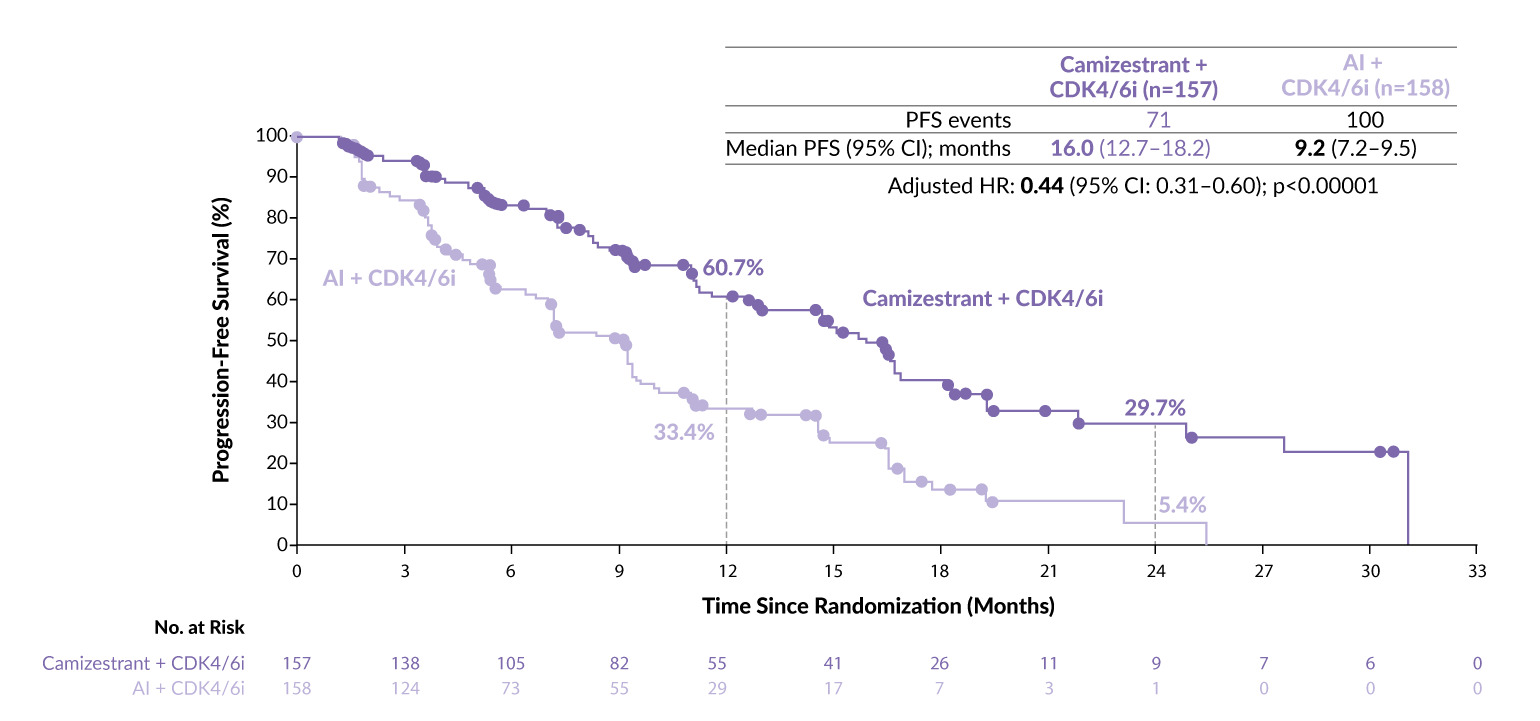
The SERENA-6 study tested the hypothesis that introducing camizestrant, a next-generation, oral selective estrogen receptor degrader (SERD) and complete ER antagonist, at the time of ESR1 mutation emergence (before clinical progression) could extend the duration of benefit from first-line therapy.27 In this phase III study, patients with ER-positive, HER2-negative advanced breast cancer were screened regularly for the emergence of ESR1 mutations. Among the 3,256 tested patients, 315 developed detectable ESR1 mutations during first-line AI plus CDK4/6 inhibitor and were randomized 1:1 to either continue the AI (n=158) or switch to camizestrant (n=157), while maintaining the CDK4/6 inhibitor. The most commonly used CDK4/6 inhibitor across both arms was palbociclib (76% of patients).
The primary endpoint of PFS was met with statistical significance. Patients who switched to camizestrant had a median PFS of 16.0 months, compared with 9.2 months for those continuing AI (HR: 0.44 [95% CI: 0.31–0.60]; p<0.00001) (Figure 1).27 Kaplan-Meier curves showed early separation, with substantial PFS differences at one year (60.7% vs 33.4%) and two years (29.7% vs 5.4%). While PFS2, which is considered a more robust surrogate for OS, was not mature in the interim analysis, it showed a trend in favor of camizestrant (HR: 0.52 [95% CI: 0.33–0.81]; p=0.0038), with 1-year PFS2 rates of 85.4% with camizestrant versus 74.4% with AI.
Regarding safety, the rates of treatment discontinuation were 1.3% with camizestrant and 1.9% with AI.27,28 As expected, neutropenia was common due to the ongoing CDK4/6 inhibition and the incidence was higher in the camizestrant group, likely reflecting longer treatment duration (45% vs 34%). Photopsia was reported more frequently in the camizestrant group (20% vs 8%); however, the symptoms were mild and transient and did not impact daily functioning or visual acuity. Anemia and leukopenia were also observed but overall, patients maintained good quality of life (QoL), with switching to camizestrant consistently delaying time to clinically meaningful deterioration (TTD) in global health status.27–29 TTD favored camizestrant compared with AI across both cancer symptoms and functioning domains, including pain, fatigue, shortness of breath/dyspnea, physical functioning, role and emotional functioning, as well as breast and arm symptoms.29
Together, the data from the SERENA-6 trial mark a pivotal advance in precision oncology, demonstrating that early ctDNA-guided intervention can improve first-line outcomes and enable preemptive optimization of therapy in advanced breast cancer before clinical progression. However, certain limitations of the study including the absence of proven OS benefit from early endocrine-backbone switching, the higher use of chemotherapy or ADCs as subsequent therapy in the camizestrant arm and the logistical burden of large-scale molecular screening indicate that further evidence is needed before this strategy can be widely adopted.
_in_the_serena-6_trial.png)
HR-positive breast cancer with PIK3CA-mutation: The INAVO120 trial shows longer survival and delayed chemotherapy with inavolisib
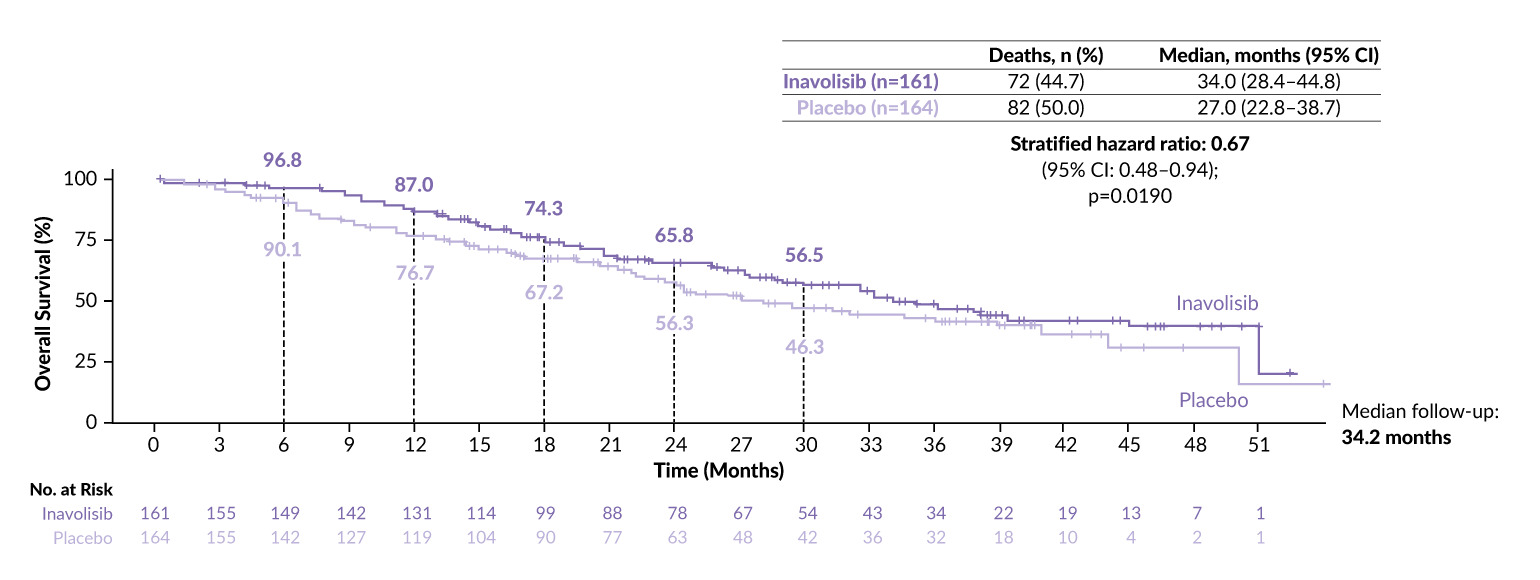
Inavolisib is an oral, highly potent and selective PI3Kα inhibitor that binds to the mutated PI3Kα enzyme, particularly in cancers with activating PIK3CA mutations, and can be co-administered at full doses along with palbociclib and fulvestrant.7,30 The phase III INAVO120 study enrolled patients with PIK3CA-mutated, HR-positive, HER2-negative advanced breast cancer who had progressed during or within 12 months after completing adjuvant ET and had not received prior systemic therapy for advanced disease. This population is known to respond less favorably to CDK4/6 inhibition alone, which makes this study particularly relevant.
A total of 325 patients were randomly assigned in a 1:1 ratio to receive either inavolisib or placebo in combination with the standard of care (SoC) therapy consisting of palbociclib and fulvestrant. The study previously demonstrated a significant PFS benefit with the inavolisib-containing regimen7 and updated results presented this year showed a significant OS advantage.30 The median OS was 34.0 months in the inavolisib arms versus 27.0 months in the placebo arm (HR: 0.67 [95% CI: 0.48–0.94]; p=0.0190) (Figure 2).6,30 The PFS benefit was maintained with the longer follow-up, showing a median of 17.2 months with inavolisib versus 7.3 months with placebo (HR: 0.42 [95% CI: 0.32–0.55]). The triplet therapy also delayed the need for the first subsequent chemotherapy by 23 months, with a median of 35.6 months versus 12.6 months (HR: 0.43 [95% CI: 0.30–0.60]).
Although higher toxicity was observed in the inavolisib group, adverse events (AEs) were generally manageable.30 Patients in the inavolisib arm experienced more frequently severe AEs (grade 3–4, 90.7% vs 84.7%; grade 5, 3.7% vs 1.2%) and serious AEs (27.3% vs 13.5%) compared with those in the placebo arm, but only 6.8% of AEs led to inavolisib discontinuation. The most common grade 3–4 AEs in the inavolisib arm included neutropenia (82.6% vs 80.4% with placebo), thrombocytopenia (12.7% vs 4.9%), anemia (6.8% vs 1.8%) and hyperglycemia (6.8% vs 0%).
_in_the_inavo120_trial.png)
Antibody-drug conjugates
HER2-positive breast cancer: The DESTINY-Breast09 trial demonstrates superior progression-free survival with trastuzumab deruxtecan plus pertuzumab
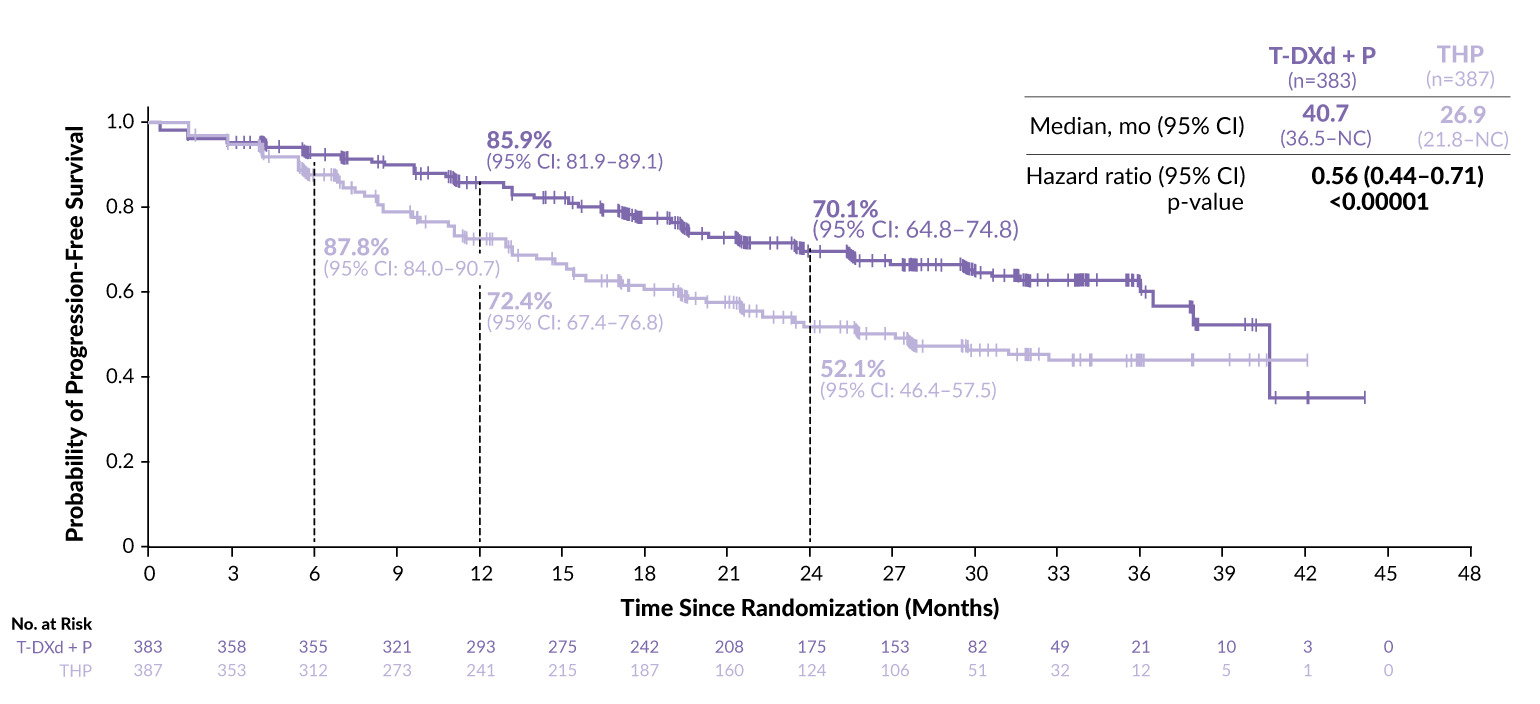
The phase III DESTINY-Breast09 trial evaluated first-line treatment strategies for HER2-positive metastatic breast cancer.31 While T-DXd has been the SoC in the second-line setting based on the DESTINY-Breast03 study, showing a median PFS of 28.8 months versus 6.8 months with T-DM1,15,16 this new study assessed its role earlier in the treatment sequence. Patients with previously untreated HER2-positive advanced or metastatic breast cancer were randomized 1:1:1 to receive T-DXd plus placebo (n=387), T-DXd plus pertuzumab (n=383) or THP (n=387).31 A statistically significant and clinically meaningful improvement in PFS was reported with T-DXd plus pertuzumab versus THP at a median follow-up of 29.2 months (median, 40.7 months versus 26.9 months; HR: 0.56 [95% CI: 0.44–0.71]; p<00001) (Figure 3).31
Secondary endpoints also favored T-DXd plus pertuzumab versus THP.31 The overall response rate (ORR) was 85.1% versus 78.6%, with 15.1% of patients in the T-DXd arm achieving a complete response (CR) compared with 8.5% in the THP arm. The median duration of response (DoR) was 39.2 months and 26.4 months, respectively, with 2-year rates of 73.3% and 54.9%. Although still immature, data for PFS2 also suggested a benefit with T-DXd plus pertuzumab, with the median PFS2 not reached versus 36.5 months (HR: 0.60 [95% CI: 0.45–0.79]; nominal p=0.00038). Fewer patients required second-line therapy after discontinuation in the T-DXd combination than in the THP arm (32.4% vs 46.8%). A recent subgroup analysis of outcomes in the T-DXd plus placebo versus THP arms demonstrated a clinically meaningful PFS advantage and improved responses with T-DXd plus placebo across key subgroups irrespective of hormone receptor or PIK3CA mutation status and prior treatment.32
_in_the_destiny-breast09_trial.png)
Despite the efficacy advantage, the T-DXd combination was associated with increased toxicity. The most common grade ≥3 treatment-emergent adverse events (TEAEs) with T-DXd included nausea (5.0% vs 0.3%), diarrhea (6.8% vs 5.2%) and neutropenia (23.9% vs 33.2%).31 Consistent with previous studies, two treatment-related deaths due to interstitial lung disease (ILD) occurred (0.5%), although no new safety signals related to left ventricular dysfunction were observed. Notably, treatment with both T-DXd and chemotherapy was recommended until disease progression, while in clinical practice in Switzerland, taxane-based chemotherapy is typically limited to six to eight cycles.
Taken together, the DESTINY-Breast09 study shifts the first-line standard of care for HER2-positive advanced or metastatic breast cancer, although toxicity remains a concern. Recently, the phase III PATINA trial showed that adding the CDK4/6 inhibitor palbociclib to standard maintenance endocrine and anti-HER2 therapy after induction chemotherapy significantly prolonged PFS from 29.1 months to 44.3 months (HR: 0.74 [95% CI: 0.58–0.94]; p=0.0074) in patients with HER2-positive, HR-positive metastatic breast cancer with manageable toxicity.33 Together, these findings highlight the benefit of targeting more than just the HER2 pathway in HER2-positive disease and support sequencing strategies that combine HER2 and endocrine blockade, thus offering prolonged disease control while preserving QoL.
Clinical benefit of adding sacituzumab govitecan to pembrolizumab in PD-L1-positive TNBC: ASCENT-04/KEYNOTE-D19
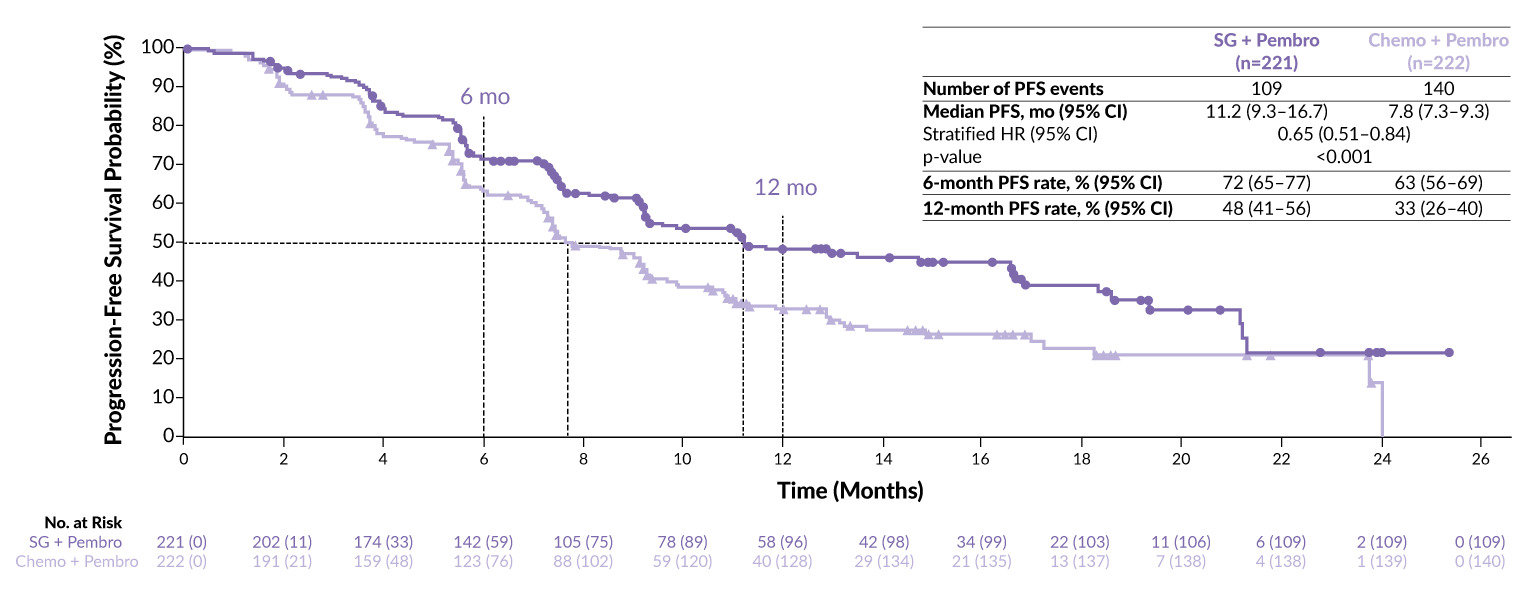
The ASCENT-04/KEYNOTE-D19 study evaluated the combination of a TROP-2-directed ADC SG and pembrolizumab in the first-line setting compared with the current SoC of chemotherapy plus pembrolizumab in patients with TNBC. This study enrolled patients with previously untreated, locally advanced unresectable or metastatic PD-L1-positive TNBC (CPS ≥10) with de novo disease or who had completed curative-intent therapy at least six months prior to recurrence.34 Patients were randomly assigned at a 1:1 ratio to either SG plus pembrolizumab (n=221) or chemotherapy plus pembrolizumab (n=222). At a median follow-up of 14.0 months, SG plus pembrolizumab significantly reduced the risk of progression or death by 35% compared with chemotherapy plus pembrolizumab (HR: 0.65 [95% CI: 0.51–0.84]; p<0.001), with a 1-year PFS rate of 48% versus 33%, respectively (Figure 4).34 The median PFS was 11.2 months with SG plus pembrolizumab and 7.8 months with SoC. Tumor response rate and DoR were also superior with SG, with an ORR of 60% versus 53% and a median DoR of 16.5 months versus 9.2 months.
_in_the_ascent-04_keynote-d19_trial.png)
Although there had been some concerns about potentially increased toxicity when combining an immune checkpoint inhibitor with an ADC, this was not observed. TEAEs occurred at comparable rates between the treatment arms and were consistent with previously reported data for SG and pembrolizumab, with no evidence of additive toxicity.34 The most frequent grade ≥3 TEAEs with SG plus pembrolizumab versus SoC were neutropenia (43% vs 45%), fatigue (8% vs 3%) and diarrhea (10% vs 2%). TTD in physical functioning was comparable between SG plus pembrolizumab versus chemotherapy plus pembrolizumab; however, sensitivity analysis demonstrated possible delay in physical decline with SG plus pembrolizumab (9.3 months vs 6.9 months; HR: 0.82 [95% CI: 0.60–1.11]), as well as improved outcomes across several EORTC QLQ-C30 domains but clinically meaningful worsening of diarrhea (for 10.41 points).35
Taken together, this study is practice-changing, given that only half of patients with TNBC proceed to second-line therapy and optimizing first-line treatment is critical. Although the combination is not yet reimbursed or included in the treatment guidelines in Switzerland, label changes are expected soon. Once approved, this regimen is likely to become a new SoC in the first-line treatment of TNBC.
TNBC ineligible for PD-1/PDL1-inhibitors: Reduced progression with sacituzumab govitecan (ASCENT-03 trial) or datopotamab deruxtecan (TROPION-Breast02)
The results of ASCENT-04/KEYNOTE-D19 were complemented by the recently published outcomes of the phase III ASCENT-03 trial, which also investigated first-line SG in advanced TNBC. Many patients with previously untreated metastatic TNBC are not candidates for immunotherapy targeting programmed cell death protein 1 (PD-1)/PD-L1,9 which further limits treatment options in this aggressive disease. To address this unmet need, ASCENT-03 enrolled patients with previously untreated, locally advanced, inoperable or metastatic TNBC whose tumors were either PD-L1-negative, were PD-L1–positive and had previously received a PD-1 or PD-L1 inhibitor in the curative setting, or were ineligible for PD-1/PD-L1 inhibitors due to the presence of comorbidities.36 A total of 558 patients were randomized 1:1 to receive SG or treatment of physician’s choice (paclitaxel, nab-paclitaxel or gemcitabine plus carboplatin). Patients in the chemotherapy arm were allowed to cross over to second-line SG following disease progression. The primary endpoint was PFS and the secondary endpoints included OS, ORR, DoR, time to onset of response (TTR), safety and QoL.
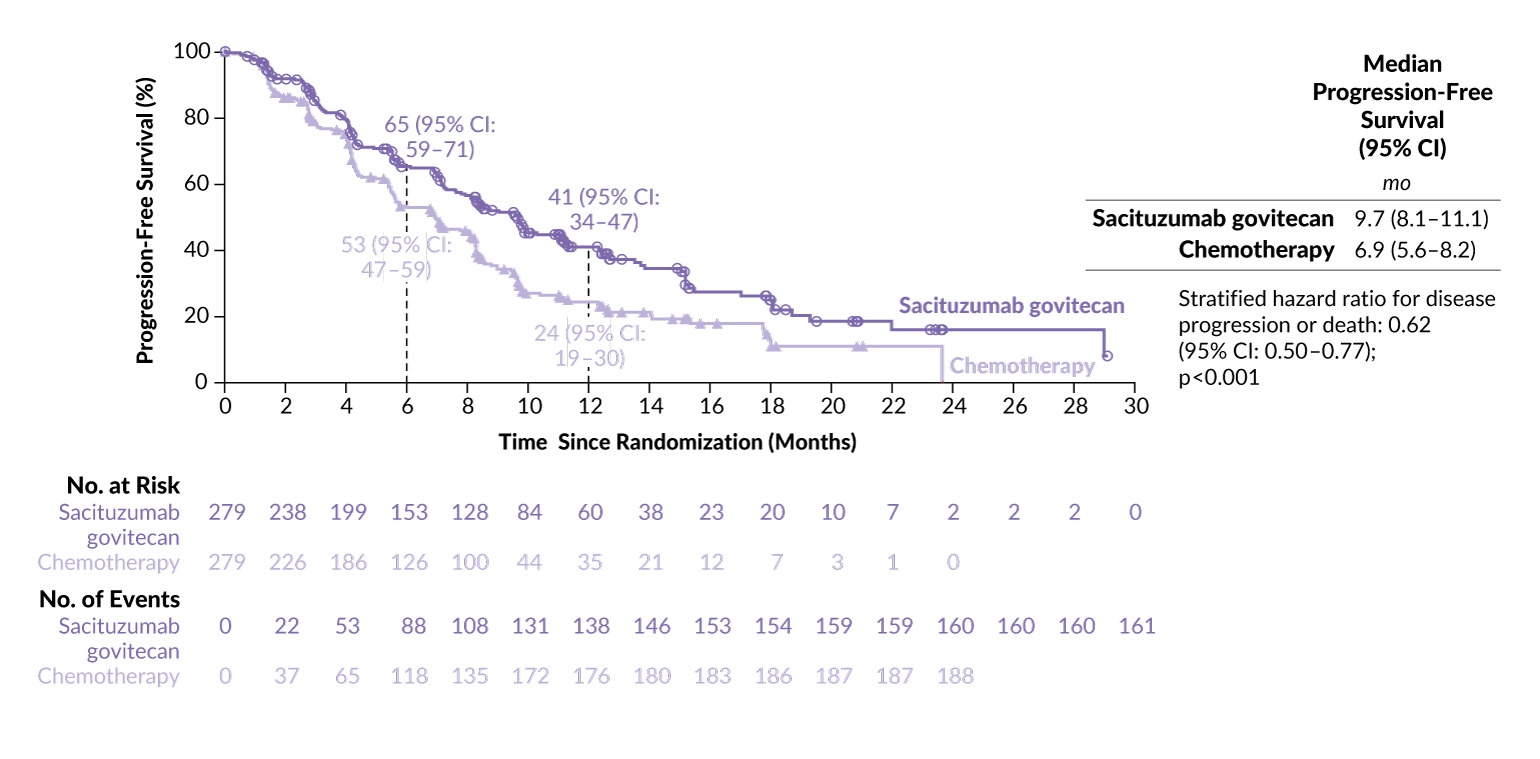
SG demonstrated a statistically significant and clinically meaningful improvement in PFS compared with chemotherapy, reducing the risk of disease progression or death by 38% (HR: 0.62 [95% CI: 0.50–0.77]; p<0.0001) (Figure 5).36 At a median follow-up of 13.2 months, the median PFS was 9.7 months with SG compared with 6.9 months with chemotherapy (12-month PFS rates, 41% vs 24%, respectively). The ORR was comparable between the treatment arms and the median DoR was 12.2 months with SG versus 7.2 months with chemotherapy. The OS data are still immature. It is important to note that since patients were offered the option by the manufacturer to receive second-line SG after disease progression, this ethically commendable measure may, however, influence subsequent OS analyses. The median PFS2 was longer in the SG arm at 18.2 months, as compared with 14.0 months with chemotherapy (HR: 0.70 [95% CI: 0.55–0.90]).
The ability of SG to delay death and progression in this population represents an important milestone in offering new hope for patients with TNBC who are ineligible for PD-1/PD-L1-targeting immunotherapy and, therefore, have limited treatment options and poor prognosis.
_in_the_ascent-03_trial.png)
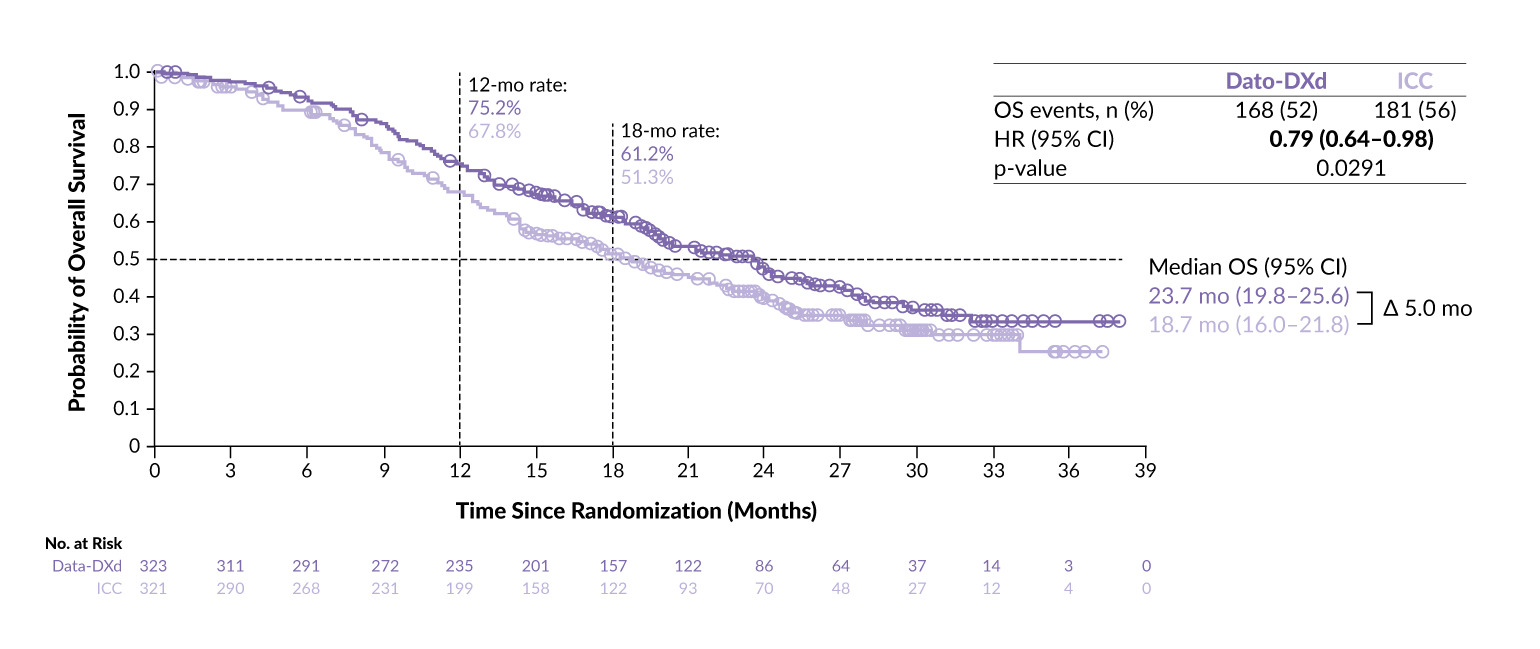
The efficacy and safety of another TROP-2-directed ADC, Dato-DXd, were recently evaluated in the phase III TROPION-Breast02 trial in TNBC patients who were ineligible for immunotherapy.37 Immunotherapy ineligibility was defined as PD-L1-negative disease or PD-L1-positive disease with relapse after prior (neo)adjuvant PD-1/PD-L1 therapy, comorbidities precluding checkpoint inhibition or lack of regulatory access to pembrolizumab in the country of treatment. The trial did not mandate a specific time interval from prior immunotherapy, in contrast to ASCENT-03 which required a minimum interval of ≥6 months between completion of curative-intent anti–PD-1/PD-L1 treatment and recurrence.36 In TROPION-Breast02, patients with previously untreated locally recurrent inoperable or metastatic TNBC who were not candidates for first-line immunotherapy were randomized 1:1 to receive Dato-DXd (n=323) or the investigator’s choice of chemotherapy, including paclitaxel, nab-paclitaxel, capecitabine, eribulin mesylate or carboplatin (n=321).37 The dual primary endpoints were OS and PFS by blinded independent central review. The secondary endpoints included investigator-assessed PFS, ORR, DoR and safety. No crossover was allowed.
At a median follow-up of 27.5 months, Dato-DXd reduced the risk of progression or death by 43% compared with chemotherapy (HR: 0.57 [95% CI: 0.47–0.69]; p<0.0001), with almost double the 18-month PFS rate (32.7% vs 16.8%) and a median PFS of 10.8 months versus 5.6 months, respectively.37 OS was also significantly improved with Dato-DXd (HR: 0.79 [95% CI: 0.64–0.98]; p=0.0291) with a median OS of 23.7 months vs 18.7 months (Figure 6). The ORR more than doubled with Dato-DXd vs chemotherapy (62.5% vs 29.3%), with a higher CR rate (9% vs 2.5%) and a longer median DoR (12.3 months vs 7.1 months). The safety profile of Dato-DXd was manageable and generally consistent with previous reports. This study further expands the existing treatment landscape for patients with locally recurrent inoperable or metastatic TNBC who are ineligible for immunotherapy, supporting Dato-DXd as a new first-line SoC in this setting.
_in_the_tropion-breast02_trial.png)
Conclusions
Recent clinical trials continue to demonstrate a shift toward more personalized and durable first-line treatment strategies across various breast cancer settings. In HR-positive disease, patients with a PIK3CA mutation who experience early ET recurrence now have an approved and recommended option with the PI3K inhibitor inavolisib in combination with palbociclib and fulvestrant. For patients whose tumors developed ESR1 mutations during first-line AI therapy, switching to camizestrant, a SERD and complete ER antagonist, while maintaining the CDK4/6 inhibitor, demonstrated improved PFS compared with continuing the AI. In parallel, ADCs such as T-DXd, SG and Dato-DXd are set to transform routine clinical practice by delivering stronger and more durable clinical outcomes across subtypes.
Together, these developments highlight a clear trajectory toward more individualized, effective and tolerable treatments, reflecting a renewed commitment to patient-centered innovation in oncology. Importantly, changes in patient-reported outcomes remain essential when balancing clinical benefit against potential harms, ensuring that therapeutic progress translates into real improvements in patients’ lives.
Conflict of interest
Marcus Vetter received honoraria for consultancy from GSK, Roche, Novartis, ExactSciences, Pfizer, Stemline, AbbVie and ASC Oncology. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way.
Funding
The author has declared that no financial support was received from any organization for the submitted work.
Author contributions
The author created and approved the final manuscript.