ADC Therapy for Breast Cancer: Current Progress and Future Directions
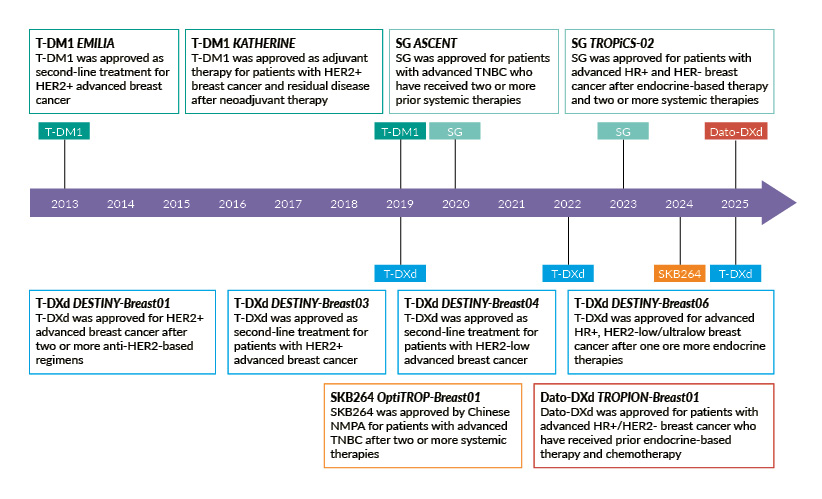
Antibody-drug conjugates (ADCs), which combine the high specificity of monoclonal antibodies (mAbs) and the potent activity of cytotoxic drugs, have become major players in targeted cancer therapy owing to their significant clinical activity in various cancers. The success of the first human epidermal growth factor receptor 2 (HER2)-targeting ADC trastuzumab emtansine (T-DM1) in second-line HER2-positive metastatic breast cancer marked a significant milestone that paved the way for a new wave of next-generation ADCs in breast cancer (Figure 1).1,2

Trastuzumab deruxtecan (T-DXd), an ADC carrying a DNA topoisomerase I inhibitor payload (deruxtecan), demonstrates greater cytotoxicity compared with T-DM1, which carries a tubulin inhibitor (DM1), due to a higher drug-to-antibody ratio (DAR) (8 vs 3.5).3,4 It also has an enzyme-cleavable linker that ensures targeted drug release, systemic stability and bystander killing of neighboring tumor cells. Findings from the head-to-head phase III DESTINY-Breast03 trial established T-DXd as the standard of care (SoC) in patients with metastatic HER2-positive breast cancer upon progression.5,6 In the long-term analysis of this study, T-DXd improved both progression-free survival (PFS) (HR: 0.30 [95% CI: 0.24–0.38]; p<0.001) and overall survival (OS) (HR: 0.73 [95% CI: 0.56–0.94]) compared with T-DM1, with a median PFS of 29.0 months versus 7.2 months and a median OS of 52.6 months versus 42.7 months, respectively.7
Beyond advanced disease, these ADCs are also being investigated in early breast cancer settings. T-DM1 is approved as an adjuvant treatment for patients with HER2-positive early breast cancer with residual invasive disease in the breast or axilla after neoadjuvant taxane-based chemotherapy and trastuzumab, as supported by the phase III KATHERINE trial.8,9 At a median follow-up of 8.4 years, T-DM1 significantly improved OS compared with trastuzumab (7-year rate, 89.1% vs 84.4%; HR: 0.66 [95% CI: 0.51–0.87]; p=0.003), along with a sustained invasive disease-free survival (DFS) (7-year rate, 80.8% vs 67.1%; HR: 0.54 [95% CI: 0.44–0.66]).10
T-DXd is currently being directly compared with T-DM1 in the phase III DESTINY-Breast05 trial.11 It is also under investigation in the neoadjuvant setting as monotherapy or administered for four cycles followed by trastuzumab, pertuzumab and paclitaxel in comparison with standard treatment in the DESTINY-Breast11 trial.12 Both studies are expected to be completed and presented at upcoming congresses later this year.
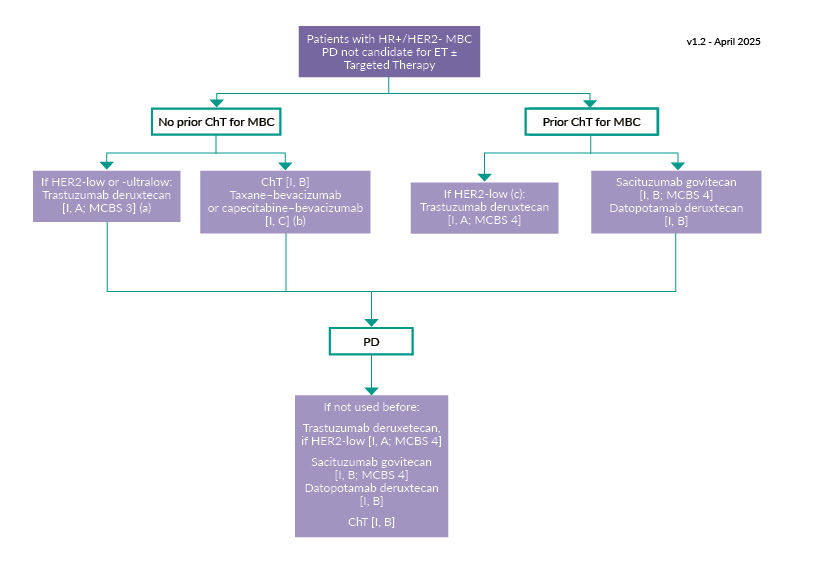
In hormone receptor (HR)-positive, HER2-negative metastatic breast cancer, defined as immunohistochemical (IHC) 0, 1+ or IHC2+ with negative in situ hybridization (ISH), the first-line treatment includes a combination of cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitor and endocrine therapy (ET).8,9 Subsequent strategies are guided by various clinical factors, including disease aggressiveness, organ function, progression on prior ET and somatic/germline mutational status, as well as the toxicity profile of therapy and patient preferences. For patients with endocrine-resistant disease, treatment options include chemotherapy and newer ADCs, such as T-DXd and Trop-2-directed sacituzumab govitecan (SG) and datopotamab deruxtecan (Dato-DXd) (Figure 2). However, these ADCs are not always approved or reimbursed in all settings in accordance with this guideline.
-positive__human_epidermal_grow.jpg)
Traditionally, HER2-low breast cancer, defined as IHC1+ or IHC2+ with negative ISH, has been classified as HER2-negative breast cancer due to the lack of clinical benefit from earlier HER2-directed therapies.13 However, T-DXd has shown remarkable efficacy in this subtype, which represents approximately 60% of HER2-negative metastatic breast cancers, highlighting the need for more precise pathological evaluation and tailored treatment approaches.14 In the phase III DESTINY-Breast04 study, T-DXd significantly improved PFS (HR: 0.51 [95% CI: 0.40–0.64]; p<0.001) and OS (HR: 0.64 [95% CI: 0.48–0.86]; p=0.003) compared with chemotherapy in patients with HR-positive, HER2-low metastatic breast cancer after 1–2 prior treatment lines.8,9,14 As a result, T-DXd is now the preferred option after first-line chemotherapy, according to the ESMO guidelines.
The Trop2-directed SG is also recommended after ET and ≥2 prior lines of chemotherapy in HER2-negative disease, supported by data from the phase III TROPiCS-02 trial, which showed an OS benefit over chemotherapy (HR: 0.79 [95% CI: 0.65–0.96]; p=0.02).15 Dato-DXd is another approved treatment option in this setting, based on results from the phase III TROPION-Breast01 trial.16–19 Although it did not significantly improved OS versus chemotherapy (HR: 1.01), Dato-DXd showed meaningful PFS benefit (HR: 0.63; p<0.0001) and a more favorable safety profile, with fewer grade ≥3 treatment-related adverse events (TRAEs; 22% vs 46% with chemotherapy), supporting its continued use and investigation.
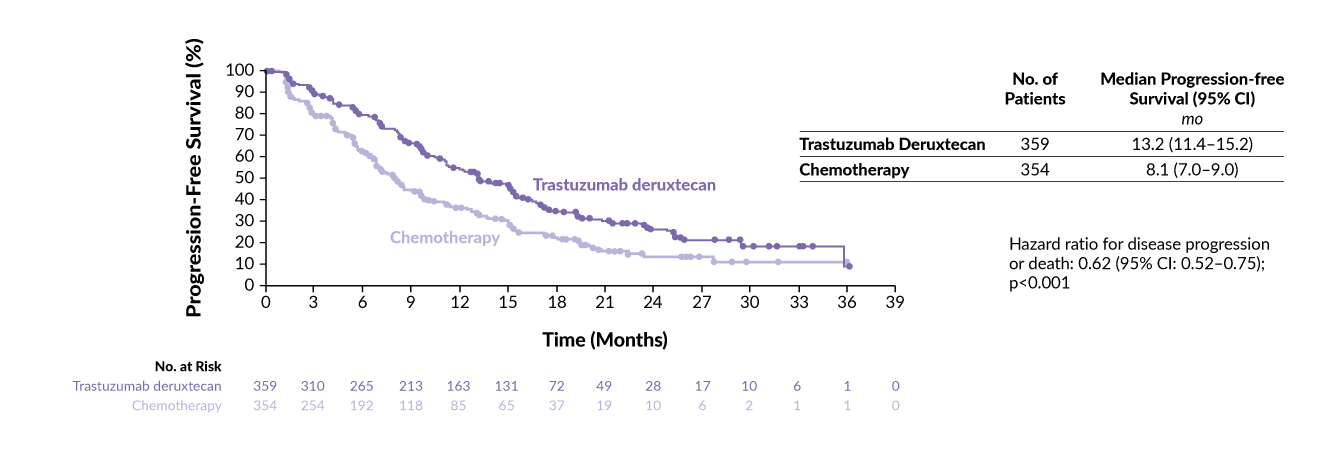
Given the poor prognosis upon progression on CDK4/6 inhibitors, the phase III DESTINY-Breast06 trial investigated the efficacy of T-DXd versus chemotherapy after ET in patients with low or ultralow HER2 expression (IHC 0 with detectable membrane staining) who had not received prior chemotherapy.20 In the HER2-low population, T-DXd significantly prolonged PFS compared with chemotherapy (HR: 0.62 [95% CI: 0.52–0.75]; p<0.001), with a median of 13.2 months versus 8.1 months, respectively (Figure 3). Consistent results were reported for the exploratory HER2-ultralow cohort (13.2 months vs 8.3 months; HR: 0.78 [95% CI: 0.50–1.21]); notably, however, the trial was not powered to show statistical significance in the HER2-ultralow population. The confirmed objective response rate (ORR) with T-DXd was 57% versus 32% with chemotherapy in the HER2-low population and it was doubled in the HER2-ultralow subgroup (62% vs 26%).
These findings led to the inclusion of T-DXd in the treatment guidelines by both the European Society for Medical Oncology (ESMO) and the German Gynecological Oncology Group (AGO) as a recommended post-ET option for patients with HER2-low metastatic breast cancer.8,9,21 Notably, central versus local HER2 scoring in DESTINY-Breast06 revealed a 78% overall concordance for HER2-low classification, although 64% of centrally confirmed HER2-low/ultralow tumors had received a HER2 IHC score of 0 locally. These findings further reinforce the need for increased awareness and standardization in HER2 assessment for informed treatment decision-making.22
-positive__human_epidermal.jpg)
In metastatic relapsed or refractory triple-negative breast cancer (TNBC), SG is the preferred treatment option after previous chemotherapy, while T-DXd may be considered for patients with HER2-low disease after at least one line of chemotherapy.8,9 In the phase III ASCENT study, SG significantly prolonged both PFS (HR: 0.41 [95% CI: 0.32–0.52]; p<0.001) and OS (HR: 0.48 [95% CI: 0.38–0.59]; p<0.001) compared with single-agent chemotherapy in patients without brain metastases (BMs), with a median OS of 12.1 months versus 6.7 months, respectively.23 In the HR-negative, HER2-low subset of the phase III DESTINY-Breast04 trial (representing approximately 10% of the study population), T-DXd also demonstrated a meaningful benefit over chemotherapy, with a median PFS of 8.5 months versus 2.9 months (HR: 0.46 [95% CI: 0.24–0.89]) and a median OS of 18.2 months vs 8.3 months (HR: 0.48 [95% CI: 0.24–0.95]), respectively.14 However, this finding is based on a small exploratory subgroup analysis and should therefore be interpreted with caution compared with the dedicated phase III evidence supporting SG in TNBC.
In the early disease setting, several trials are investigating ADCs in patients who did not achieve a pathological complete response (pCR) post-neoadjuvant therapy. SG is being evaluated as monotherapy in HER2-negative breast cancer (TNBC or HR-positive) in the phase III SASCIA trial and in combination with pembrolizumab in the phase III ASCENT-05 trial.24,25 Additionally, the combination of sacituzumab tirumotecan and pembrolizumab is under investigation in the phase III MK-2870-012 study (TNBC).26 Furthermore, the ongoing phase III TROPION-Breast04 trial is investigating neoadjuvant Dato-DXd combined with durvalumab, followed by adjuvant durvalumab with or without chemotherapy, compared with the SoC chemotherapy plus pembrolizumab in patients with previously untreated stage II–III TNBC or HR-low (1% to <10%)/HER2-negative breast cancer.27,28
An important consideration in breast cancer management is the development of BMs, which occur in approximately 30–50% of patients, most commonly those with HER2-positive breast cancer or TNBC.29 Emerging data indicate that ADCs demonstrate meaningful intracranial (IC) activity. Pooled analysis of DESTINY-Breast01, -02 and -03 trials in HER2-positive breast cancer showed notable BM response with T-DXd, including patients with treated or stable BMs (IC ORR: 45% vs 28% with comparator therapy) and those with untreated or active lesions (46% vs 12%).30 These data are further supported by findings from the phase IIIb/IV DESTINY-Breast12 study, which evaluated T-DXd in patients with previously treated HER2-positive breast cancer, regardless of BM status.31 Treatment with T-DXd resulted in a central nervous system (CNS) overall response in 79% of patients with stable BMs at baseline and 62% of those with active BMs. Notably, among patients with active BMs, the CNS ORR was 83% in those with untreated lesions and 50% in those with previously treated lesions, thus favoring the use of T-DXd in these challenging populations.
In summary, ADCs have consistently demonstrated superiority over chemotherapy in metastatic breast cancer and are being increasingly investigated in earlier disease settings.
Resistance to ADCs and emerging therapies
Most patients develop acquired, rather than primary, resistance to ADCs. Their complex design may activate multiple potential mechanisms of resistance, which may include alterations in target antigen expression, changes in payload sensitivity and disruptions in intracellular antibody trafficking.32,33 For example, one study reported parallel genomic alterations in both the antigen and payload targets, conferring resistance to SG in TNBC.34
The dynamic nature of tumor biology is also evident in the instability of HER2-low expression, with most fluctuations shown between HER2-low and -negative status, observed in 14−15% of cases in either direction.35 These data, along with inter-metastatic heterogeneity in HER2 expression in HER2-low disease, suggest that earlier use of T-DXd before disease evolution may be advantageous.36 With respect to optimal sequencing within the evolving treatment landscape, PFS2, defined as the time to progression on first subsequent therapy or death, may be an increasingly relevant endpoint in industry-sponsored trials.
Ultimately, prospective studies are needed to guide treatment algorithms.37,38 One real-world study that evaluated post-T-DXd regimens found that clinical outcomes significantly varied by disease subtype and subsequent therapy.39 In HR-positive, HER2-negative breast cancer, chemotherapy (capecitabine or eribulin) yielded better PFS outcomes than SG (median, approximately 6 months vs 2.5 months). In contrast, all regimens following T-DXd in TNBC were associated with shorter median PFS (≤3 months). However, these findings should be interpreted with caution, as they are based on a case series rather than a randomized controlled trial.
Strategies to delay or prevent resistance after earlier ADC exposure include the development of novel agents with alternative targets or cytotoxic payloads. There are several novel HER2-targeting ADCs in ongoing trials such as trastuzumab duocarmazine, ARX788, disitamab vedotin and zanidatamab zovodotin.40–43 When exploring new targets, it is essential to consider both the tumor and the tumor microenvironment (TME), including stroma, vasculature and immune cells, while accounting for expression patterns and tumor heterogeneity.44 Notable examples include patritumab deruxtecan (targeting HER3), praluzatamab ravtansine (targeting CD166) and the immune-stimulating HER2-targeted BDC-1001, all showing promising results in phase I/II trials.45–47 Another investigational ADC is MORAb-202, which is composed of the folate receptor alpha (FRα)-directed mAb farletuzumab and the microtubule dynamics inhibitor eribulin, conjugated via a cathepsin-B-cleavable linker.48
Combination regimens with immune checkpoint inhibitors (ICIs) are also under active investigation. For example, the phase Ib/II BEGONIA trial investigates durvalumab with novel oncology therapies in first-line metastatic TNBC.49 In the study arm 7, durvalumab in combination with Dato-DXd demonstrated promising activity, including an ORR of 74%, with responses observed regardless of PD-L1 expression.
In summary, ADCs continue to evolve rapidly and are changing the therapeutic landscape for breast cancer, especially by offering new targeted options for patients with limited treatment choices, such as those with TNBC. ADCs have also expanded treatment possibilities in HER2-low disease, which is not a distinct subtype but rather a therapeutic target. Effective sequencing and patient selection remain key to optimizing outcomes.
Optimizing toxicity management of ADCs
ADC therapy is associated with an increased incidence of certain uncommon but potentially life-threatening TRAEs.50 This underscores the need for proactive monitoring, early recognition and optimized treatment strategies to ensure patient safety and treatment continuity.
One of the most significant TRAE of interest is interstitial lung disease (ILD)/pneumonitis, initially reported in patients receiving T-DXd.50 Although most cases are mild or moderate in severity, the associated mortality rate of approximately 1% has led to the development of specific guidelines for the monitoring and management of T-DXd-related ILD/pneumonitis.50–53 In the DESTINY-Breast12 study, patients with baseline BMs had a higher incidence of grade 5 ILD compared with those without BMs (2.3% vs 1.2%).31 Notably, four of six fatal ILD cases involved concurrent opportunistic infections, suggesting an elevated risk in patients on corticosteroids for symptom relief. Therefore, prophylaxis against Pneumocystis jirovecii pneumonia is strongly recommended in patients taking chronic corticosteroids.
ILD is typically suspected in the presence of new or worsening respiratory symptoms and/or radiological findings suggestive of lung inflammation.50 Suspected ILD should be treated with steroids, with rechallenge recommended only for patients with resolving grade 1 disease. In a real-world study, 78% of patients with prior grade 1 ILD were safely re-treated with T-DXd, with a median treatment duration of 100 days.54 Although the exact mechanism is not fully understood, ILD appears to be specific to T-DXd among ADCs. This is possibly due to its higher DAR and the membrane permeability of the DXd payload, which may enhance off-target uptake by alveolar macrophages.51
Neutropenia and diarrhea are other key TRAEs associated with several ADCs, with severe cases frequently reported in patients receiving SG.23,55 In the ASCENT study in patients with heavily pretreated TNBC who received SG, severe neutropenia was reported in 51% (grade 3, 34%; grade 4, 17%) and severe diarrhea in 10% (all grade 3). The payload of SG, SN-38, which is the active metabolite of irinotecan, is metabolized by the UGT1A1 enzyme. Polymorphisms in the UGT1A1 gene are associated with impaired irinotecan metabolism and increased risk of toxicity.56,57 Therefore, screening for these polymorphisms can be performed prior to treatment with SG or other irinotecan-derived ADCs.
In cases of neutropenia, granulocyte-colony stimulating factor (G-CSF) should be administered before considering dose reduction, depending on severity.58 The choice between daily G-CSF and the long-acting pegylated G-CSF should be guided by the timing of neutropenia onset, with the latter administered when neutropenia is observed on day 8 of treatment. For diarrhea, standard therapy with loperamide should be initiated at the first symptoms, given that infectious agents have been ruled out.
Stomatitis is another toxicity associated with ADCs, mainly with Dato-DXd.50 In the TROPION-PanTumor01 and BEGONIA studies, grade ≥3 stomatitis was observed in 10–11% of patients.49,59 Management typically includes steroid-containing mouthwashes (e.g., dexamethasone) to reduce inflammation and alleviate symptoms.
Ocular toxicities, specifically keratitis and dry eye, are distinctive adverse effects associated with certain ADCs.49,50,59 Although mild in most patients, these symptoms should be promptly managed in consultation with an ophthalmologist.
Escalation and treatment optimization in early HER2-positive breast cancer and TNBC
Recent advances in the management of early-stage HER2-positive breast cancer and TNBC raise important questions about the optimal balance between treatment escalation for high-risk patients and de-escalation strategies to minimize toxicity in those likely to achieve favorable outcomes.28 While pCR remains a critical surrogate for long-term outcomes at the individual patient level, its role in guiding treatment decisions continues to be debated.60 Residual cancer burden has also demonstrated independent prognostic value and is being evaluated as a tool to guide response-adapted therapeutic strategies.61
In HER2-positive disease, despite impressive outcomes with adjuvant T-DM1, invasive disease recurrence remains a concern, with a 7-year rate of 19% and no observed improvement in CNS recurrence compared with trastuzumab.10,62 These limitations have triggered interest in de-escalation strategies for patients achieving excellent responses to therapy. Phase II studies such as CompassHER2-pCR are currently investigating de-escalation following pCR, assessing the feasibility of omitting chemotherapy while continuing trastuzumab and pertuzumab.63 Furthermore, the PHERGAIN study employs a PET-guided, pCR-adapted strategy to safely omit chemotherapy in both pre- and postoperative settings, whereas TRAIN-3 evaluates early discontinuation of preoperative chemotherapy after three or six cycles in patients showing a complete response on MRI.64,65
In TNBC, neoadjuvant chemotherapy combined with pembrolizumab, followed by adjuvant pembrolizumab, is recommended for high-risk patients based on the phase III KEYNOTE-522 trial. However, the role of adjuvant pembrolizumab in pCR responders remains uncertain and no predictive biomarkers have yet been validated for precision treatment.28,66,67 Exploratory analyses of KEYNOTE-522 have not yet reliably identified predictors of response, and tumor-infiltrating lymphocytes (TILs), while potentially prognostic, remain inconsistently reported in clinical studies.
Conclusions
ADCs have revolutionized the treatment landscape of breast cancer, demonstrating significant efficacy even in HER2-low and TNBC subtypes. Despite their substantial clinical benefit, they necessitate careful consideration of therapy sequencing and proactive toxicity management. As ADCs move earlier into the treatment paradigm, the focus must shift toward thoughtful patient selection, biomarker development and balancing efficacy with long-term toxicity. Advances in antigen targeting, payload design and linker chemistry will be the key to the next generation of ADCs, with ongoing research likely to yield further breakthroughs in cancer therapy.
Conflict of interest
Marcus Vetter received honoraria for consultancy from GSK, Roche, Novartis, ExactSciences, Pfizer, Stemline, AbbVie and ASC Oncology. Christian Kurzeder reported honoraria from Tesaro, GSK, Astra Zeneca, Novartis, PharmaMar, Genomic Health, Roche, Eli Lilly S.A., Pfizer and Daichi; consulting or advisory role for Tesaro, GSK, Astra Zeneca, Novartis, PharmaMar, Genomic Health, Roche, Eli Lilly S.A., Merck MSD and Pfizer; and travel and accommodation expenses from GSK, Astra Zeneca and Roche. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way.
Funding
The authors have declared that no financial support was received from any organization for the submitted work.
Author contributions
All authors contributed to and approved the final manuscript.