

Introduction
Myelodysplastic syndromes (MDS), also known as myelodysplastic neoplasms per the WHO 2022 classification,1 are clonal hematopoietic stem cell disorders characterized by ineffective blood cell production, dysplasia of blood and bone marrow cells and an increased risk of progressing to acute myeloid leukemia (AML).2 In low-risk MDS, supportive therapies such as red blood cell transfusions and erythropoiesis-stimulating agents are used to achieve transfusion independence, although only 30–60% of patients respond and relapses frequently occur within two years.3 Higher-risk MDS has a poorer prognosis, with up to 40% of patients experiencing deterioration or progression to AML within two years of diagnosis.4 Allogeneic stem cell transplantation (allo-SCT) is the only potentially curative treatment for high-risk MDS, but its use is limited by factors such as age, comorbidities, cytogenetics, performance status, patient preference and donor availability.5 This article provides an overview of the current and emerging treatment strategies for patients with higher-risk MDS.
Current treatment guidelines
In patients with low-risk MDS, the primary treatment goal is to improve cytopenias, reduce transfusion dependency and improve quality of life, which is typically achieved through a “watch & wait” approach, supportive care with red blood count (RBC) or platelet transfusions, iron chelation and antibiotics.5 In contrast, higher-risk MDS is associated with a significant risk of progression to AML and shorter survival, and treatment aims to modify the disease course, with options including hypomethylating agents (HMAs) such as azacitidine or decitabine, allo-SCT and, less frequently, chemotherapy.5,6 In recent years, the combination of anti-apoptotic B-cell lymphoma-2 (BCL-2) protein inhibitor venetoclax with azacitidine has emerged as one of the most commonly used regimens, especially in patients ineligible for transplantation, showing promising response rates in clinical trial.7–9
Hypomethylating agents: azacitidine and decitabine
For patients with higher-risk MDS who do not have major comorbidities but are not immediately eligible for allo-SCT, azacitidine is recommended by both the European Society for Medical Oncology (ESMO) and Onkopedia, the clinical guideline platform of the German, Austrian and Swiss societies for hematology and medical oncology (DGHO, OeGHO and SGH, respectively) (Figure 1).5,6 Phase III clinical trials have demonstrated that azacitidine significantly improves overall survival (OS) compared with supportive care, with median OS ranging from 18 to 24.5 months versus 11 to 15 months, respectively, and markedly higher overall response rates (ORR) at 60% versus 5% (p<0.001).10,11 However, in the real-world study from the Spanish MDS Registry including 821 high-risk MDS patients, azacitidine did not significantly improve OS compared with conventional care (median OS, 13.4 months vs 12.2 months; p=0.41).12 Multivariate analysis confirmed that azacitidine was not an independent predictor of survival (adjusted OR: 1.08 [95% CI: 0.86–1.35]; p=0.49). Nevertheless, a trend toward better survival with azacitidine was observed in patients with chromosome 7 abnormalities (median OS,13.3 months vs 8.6 months; p=0.08).
Decitabine is another HMA that can be used in patients with higher-risk MDS; however, no significant OS benefit with decitabine over conventional treatment was reported in phase III trials. In a phase III study conducted by the European Organization for Research and Treatment of Cancer Leukemia Group and the German MDS Study Group, the median OS was 10.1 months with decitabine versus 8.5 months with conventional treatment (HR: 0.88 [95% CI: 0.66–1.17]; p=0.38).13 Notably, significant improvements were reported in terms of progression-free survival (PFS) (median, 6.6 months vs 3.0 months; HR: 0.68 [95% CI: 0.52–0.88]; p=0.004) and the cumulative incidence of AML (22% vs 33% at one year; 30% vs 43% at two years; p=0.036).
Allogeneic stem cell transplantation
Allo-SCT remains the most promising curative option for higher-risk MDS, with prolonged disease-free survival achieved in 35–50% of patients.14 However, due to high therapy-related morbidity and mortality, careful patient selection is necessary. Outcomes after allo-SCT depend heavily on cytogenetic and molecular genetic features, with adverse characteristics such as complex or monosomal karyotypes associated with a higher risk of relapse and mortality.15 Furthermore, the timing of allo-SCT is important, as studies show that immediate transplantation maximizes life expectancy for those with higher-risk disease.16,17
After disease progression following treatment with HMAs, even patients with low-risk MDS have a dismal prognosis18 and should be considered for allo-SCT, including those with severe cytopenias, progressive disease or additional unfavorable factors such as bone marrow fibrosis or adverse molecular profiles.19 Although poorer outcomes are generally observed in patients with TP53 mutations, recent analyses indicate that allo-SCT can improve survival even in these cases, including for both single-hit and multi-hit TP53 mutations, as well as for IPSS-M high-risk patients without TP53 mutations.20
Intensive and low-dose chemotherapy
AML-like intensive chemotherapy is not an established standard for patients with higher-risk MDS and is only considered in selected cases.5 Particularly, patients with higher-risk MDS generally achieve lower complete remission (CR) rates and shorter CR durations compared with those with normal karyotypes.21 The role of intensive chemotherapy is primarily limited to remission induction before planned allo-SCT and its use should be assessed individually. In a randomized phase III trial, intensive chemotherapy did not show a significant benefit over azacitidine.10 Recently, CPX-351, a liposomal formulation of daunorubicin and cytarabine, demonstrated superior outcomes over conventional daunorubicin and cytarabine in patients with AML with MDS-related features and post-MDS AML,22 which led to its approval for these AML subsets, including therapy-related AML.23 CPX-351 is currently being investigated in patients with higher-risk MDS.24
Low-dose chemotherapy has also shown inferior outcomes compared with azacitidine in a randomized phase III study, both in terms of response and survival.10 While non-intensive chemotherapy, such as low-dose cytarabine or low-dose melphalan, was historically used when no better alternatives were available for patients with advanced MDS, it may still be considered in selected cases after other treatment options, such as HMAs.6
_as_recommended_by_the.jpg)
Emerging therapies
The life expectancy of patients with higher-risk MDS is significantly shorter compared with the age-matched population and there is a high need for life-prolonging therapy. Survival of patients with relapsed/refractory (R/R) disease is poor with a median OS of 4–6 months and no standardized treatment recommendations currently exist for this population.14
Managing patients with higher-risk MDS is challenging due to the lack of effective treatment options following disease progression after HMA therapy. This highlights the need to improve the efficacy of frontline azacitidine while maintaining tolerability. Several emerging therapies are under investigation, including targeted agents such as IDH1/2 inhibitors (e.g., ivosidenib, enasidenib) and retinoic acid receptor alpha (RARA) agonists (e.g., tamibarotene). In addition, CPX-351 has shown promising efficacy in this patient population, providing higher transplantation rates. Other novel agents in development include eltanexor and BCL-2 inhibitors.
Targeting IDH1/IDH2: enasidenib and ivosidenib
Mutations in the genes encoding isocitrate dehydrogenase (IDH) enzymes 1 and 2 (IDH1 and IDH2) occur in approximately 5% of patients with MDS.25,26 Ivosidenib and enasidenib are oral, selective, mutant IDH1 and IDH2 inhibitors, respectively, indicated in combination with azacitidine for the treatment of patients with IDH1- and IDH2-mutated R/R AML.27,28
The efficacy and safety of ivosidenib in patients with IDH1-mutated higher-risk MDS were assessed in the phase II IDIOME study.29 Among those previously treated with azacitidine, the ORR was 63.6%, including 21% of patients with CR, with a median duration of response (DoR) of 4.8 months and a median OS of 8.9 months. In untreated patients, ivosidenib was associated with significant responses, with an ORR of 78.3% and a CR rate of 61%. With a median follow-up of 25.2 months, the median OS and DoR were not reached and the 12-month OS rate was 91.3%.
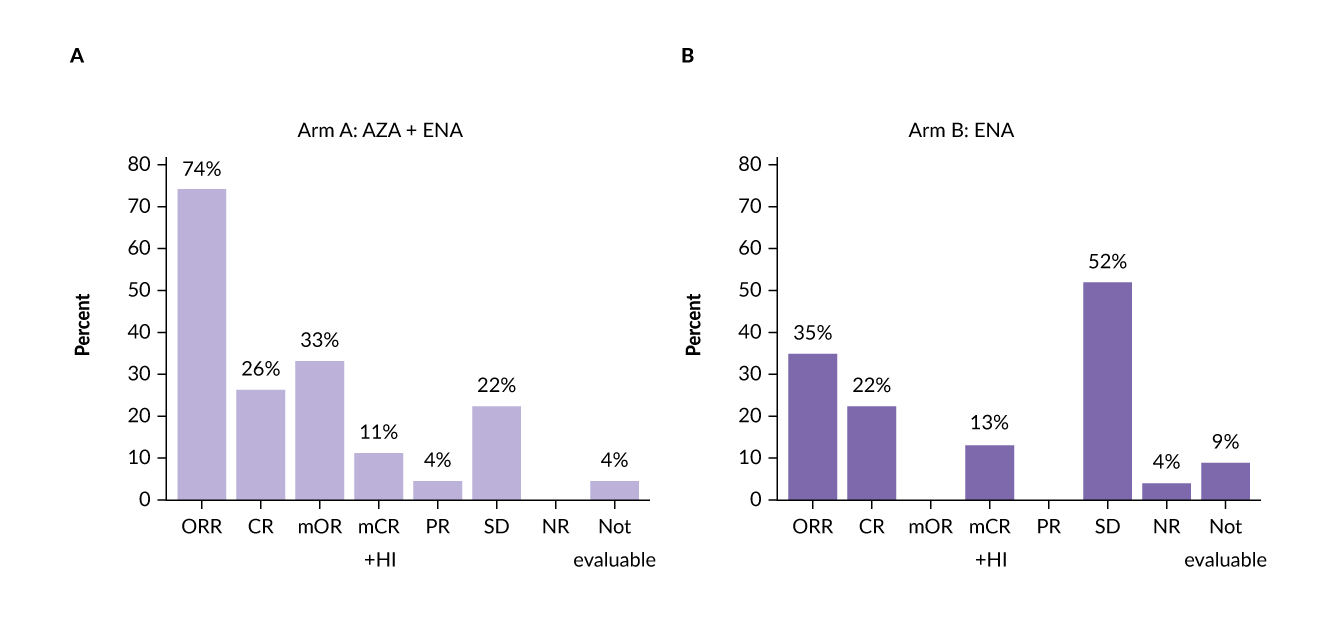
Enasidenib also showed clinical activity in patients with higher-risk MDS, both in combination with azacitidine in newly diagnosed patients and as monotherapy in HMA-pretreated patients.30 In a phase II study, frontline enasidenib plus azacitidine yielded an ORR of 74%, with a composite CR (CRc) rate of 70% and CR rate of 26% (Figure 2A). Among responding patients, the median DoR was 32 months and the median OS was 28 months. In the enasidenib monotherapy cohort, the ORR was 35%, with a CRc rate of 35% and a CR rate of 22% (Figure 2B). Three of 11 transfusion-dependent patients achieved transfusion independence by 4.6 months. The median OS was 20 months and the median event-free survival (EFS) was 6.5 months. With a median follow-up of 23 months, the estimated 24-month OS was 100% in patients who transitioned to allo-SCT.
_azacitidine_plus_enasidenib_(aza___ena)_and_b)_.jpg)
Targeting RARA overexpression: tamibarotene
The superenhancer at the retinoic acid receptor alpha (RARA) gene is associated with RARA mRNA overexpression in approximately 50% of patients with MDS, with 30% of higher-risk patients being RARA-positive.31,32 This overexpression is a target for tamibarotene, an oral potent and selective RARα agonist with improved pharmacological properties over first-generation pan-retinoids such as all-trans retinoic acid (ATRA). Initial clinical data for RARA-positive patients with R/R higher-risk MDS showed that treatment with tamibarotene resulted in myeloid differentiation, improved blood counts and reduced bone marrow blasts.33 However, the subsequent phase III SELECT-MDS-1 study assessing tamibarotene plus azacitidine in newly diagnosed RARA-positive patients with higher-risk MDS did not meet the primary endpoint of CR rate, with 23.8% of patients achieving a CR compared with 18.8% of those treated with placebo plus azacitidine (p=0.2084).34,35
CPX-351: liposomal cytarabine and daunorubicin
The encapsulated formulation of cytarabine and daunorubicin CPX-351 has demonstrated superior efficacy over the traditional 3+7 regimen in patients with secondary AML.36 CPX-351 has also been investigated in patients with higher-risk MDS and chronic myelomonocytic leukemia (CMML) in an investigator-initiated two-cohort phase II trial by the Groupe Francophone des Myélodysplasies.24 Among 31 patients (median age, 62 years), 87% achieved a response, 52% received at least one consolidation cycle and 94% proceeded to transplantation. These findings indicate that CPX-351 is a valuable treatment option, especially when subsequent allo-SCT is considered.
Further evaluation of CPX-351 in comparison to FLAG-Ida was conducted in the UK NCRI AML19 trial, which included younger patients with adverse karyotype AML and higher-risk MDS.37 Results showed no significant difference in the ORR (64% vs 76%), median OS (13.3 months vs 11.4 months) or median EFS, while relapse-free survival was significantly longer with CPX-351 (median, 22.1 months vs 8.35 months). Notably, patients with MDS-related gene mutations experienced significantly prolonged OS with CPX-351, with a median of 38.4 months versus 16.3 months.
An ongoing phase II trial is currently recruiting to investigate CPX-351 versus conventional care regimens as first-line treatment before allo-SCT in patients with higher-risk MDS and oligoblastic AML (NCT04061239).38
In in vitro animal studies, CPX-351 has been shown to prevent mucosal damage, dysbiosis and morbidity in preclinical models of intestinal inflammation by upregulating aryl hydrocarbon receptor (AhR), which plays a protective role against cellular damage, inflammation and dysbiosis.39 AhR is known to negatively regulate the NLRP3 inflammasome, a multiprotein complex involved in inflammation.40 Dysbiosis may contribute to increased susceptibility to infections and impaired barrier function, potentially playing a significant role in non-relapse morbidity (and possibly mortality) among patients experiencing microbiome disruption due to chemotherapy protocols such as 7+3 for AML or antibiotic treatments. However, further studies are needed to better understand the impact of dysbiosis on treatment outcomes in higher-risk MDS.
Eltanexor: second-generation SINE
Eltanexor is an oral, second-generation selective inhibitor of nuclear export (SINE) with low brain penetrance that demonstrated clinical activity and safety in patients with higher-risk, primary HMA-refractory MDS in a phase I/II study.41 In the efficacy cohort (n=15), the ORR was 53.3%, with 46.7% of patients achieving marrow CR and one additional patient achieving hematologic improvement. The median OS was 9.86 months in the overall cohort, with patients who attained marrow CR experiencing a longer median OS of 11.86 months compared with 8.67 months in those who did not achieve marrow CR. The most frequently reported treatment-related adverse events included nausea (45%), diarrhea (35%) and decreased appetite (35%). Eltanexor is currently being investigated in combination with venetoclax in patients with R/R MDS and AML (NCT06399640), as well as in combination with decitabine and cedazuridine in patients with MDS (NCT05918055).
BCL2 inhibition in MDS
BCL-2 protein is frequently overexpressed in several hematologic malignancies, including higher-risk MDS.8 This has led to the development of BCL-2 inhibitors such as venetoclax, which has shown efficacy in combination with azacitidine in newly diagnosed patients with AML, including those with IDH1/2 mutations.42,43 Recent clinical data have also highlighted the potential of venetoclax in higher-risk MDS. In a phase Ib study evaluating venetoclax plus azacitidine in treatment-naïve patients with higher-risk MDS, promising clinical activity was observed.7 At a median follow-up of 31.9 months, 29.9% of patients achieved CR and 50.5% achieved marrow CR, with an ORR of 80.4% (Figure 3). Among the 54 patients with the best response of marrow CR, 37.0% experienced hematologic improvement. The overall median OS was 26.0 months and OS rates at 12 and 24 months were 71.2% and 51.3%, respectively. Transfusion independence was achieved in 24 of 59 patients who were transfusion-dependent at baseline. Several later-phase clinical trials are further investigating venetoclax-based therapies in previously untreated patients with higher-risk MDS, including the phase III VERONA study to confirm the survival benefit of this combination.9

Following HMA treatment, an increase in BCL-2 and a decrease in MCL-1 levels have been observed.44 Data suggest that venetoclax may lower the apoptotic threshold in MDS and potentially allow for a response to HMAs even in previous resistant cells. Based on these findings, a phase Ib study was conducted to assess venetoclax in combination with azacitidine in patients with R/R higher-risk MDS who had progressed on prior HMA therapy.8 Marrow responses included CR in 7% of patients and marrow CR in 32%. Additionally, 36% of patients achieved transfusion independence for RBCs and/or platelets, while 43% of those with marrow CR experienced hematological improvement. The median OS was 12.6 months, which extended to 14.8 months in patients with marrow CR. The median PFS and EFS were 8.6 months and 6.9 months, respectively.
Navitoclax is another oral inhibitor of BCL-2 that has been investigated in patients with higher-risk MDS after disease progression on both HMA and venetoclax. The recently presented initial results from a phase Ib/II study suggested clinical activity of navitoclax in this refractory population; however, the study was subsequently closed to further enrollment.45
Lisaftoclax is a novel, promising BCL-2 inhibitor currently under investigation in patients with higher-risk MDS. In a phase Ib/II study evaluating lisaftoclax in combination with azacitidine, follow-up data indicated encouraging efficacy and safety in this patient population.46 Among 49 patients, the ORR was 75.0%. In the subset of 40 efficacy-evaluable, treatment-naïve patients, the ORR was 77.5%, with a CR rate of 25.0%. Notably, in 23 treatment-naïve patients who received lisaftoclax at a dose of 600 mg in combination with azacitidine, the ORR and CR rates were 73.9% and 30.4%, respectively. The cCR rate was 69.6%, with a median time to CR of 2.84 months. At the time of analysis, neither the median PFS nor OS had been reached. This combination therapy was well tolerated, with no reported 60-day mortality, minimal dose modifications and low infection rates.
Second-generation HMAs: cedazuridine and guadecitabine
Second-generation HMAs have been developed to improve the bioavailability and efficacy of traditional therapies. Decitabine, a DNA methyltransferase 1 inhibitor, is rapidly degraded by cytidine deaminase in the gut and liver, which limits its oral use.47 Cedazuridine is a cytidine deaminase inhibitor that increases the bioavailability of oral decitabine. The combination of decitabine and cedazuridine was approved by the FDA48 for the treatment of patients with intermediate- and high-risk MDS based on the ASTX727-01 and ASTX727-02 (ASCERTAIN) trials, which demonstrated CR rates of 18% and 21%, respectively, with median CR durations of 8.7 and 7.5 months.47,49
Azacitidine is another DNA methyltransferase 1 inhibitor that is currently being investigated in combination with cedazuridine. The phase I–III ASTX030-01 trial was designed to assess oral azacitidine combined with cedazuridine (ASTX030) versus subcutaneous azacitidine in patients with MDS and MDS/myeloproliferative neoplasms including CMML.50 Preliminary results from 33 patients with a median follow-up of 36.2 months showed a median OS of 29.5 months, with 24% achieving CR, 24% marrow CR and 33% stable disease.
Guadecitabine, a dinucleotide form of decitabine, has demonstrated high response rates in patients with high-risk MDS. The updated data from a phase II trial enrolling 82 patients with higher-risk MDS and eight patients with CMML showed an ORR of 52%, including a CR rate of 29%.51 The median OS was 16.8 months, with a median OS of 32 months in patients with CR and 23.3 months in patients achieving marrow CR. Notably, patients with marrow CR who underwent allo-SCT (n=9) had a median OS of 46 months, compared with 14.4 months in those who did not (p<0.005).
Targeting aberrant inflammation: emavusertib
Targeting aberrant inflammation is a promising therapeutic strategy in higher-risk MDS.52 Therapies such as IRAK-4 inhibitors, including emavusertib, and NLRP3 inhibitors, such as ibrutinib, are currently under investigation in this patient setting.
Emavusertib is a potent oral inhibitor of IRAK4, FLT3 and CLK that demonstrated potential preclinical efficacy advantages over other IRAK4 or FLT3 inhibitors.53 By inhibiting the NF-kB and MAPK pathways, emavusertib provides a mechanism to counteract known pathways of resistance to BCL2 and FLT3 inhibitors. This small-molecule inhibitor has been investigated in several phase I/II clinical trials, both as monotherapy and in combination with other agents, in R/R B-cell non-Hodgkin lymphomas (NHLs) and myeloid malignancies.
Preliminary efficacy data from the phase I/II TakeAim Leukemia trial showed antitumor activity of emavusertib in patients with higher-risk MDS with splicing factor mutations who had progressed following venetoclax- or HMA-based therapies.54 Among 14 response-evaluable patients, eight demonstrated a significant reduction in bone marrow blast percentage from baseline, with five achieving an objective response of marrow CR.
In addition to IRAK-4 inhibition, NLRP3 inhibition is also being explored as a therapeutic approach in patients with higher-risk MDS. A phase Ib clinical trial (NCT02553941) is currently evaluating the efficacy and safety of the combination of ibrutinib with azacitidine in patients with higher-risk MDS.
Lack of efficacy in recent trials of novel agents for HR-MDS and AML
Recent clinical trials investigating novel agents in HR-MDS and AML have yielded disappointing results, with several combinations failing to demonstrate meaningful clinical benefit. This includes the TIM-3 inhibitor sabatolimab, which was evaluated in combination with azacitidine in treatment-naïve patients with HR-MDS in the phase III STIMULUS-MDS2 trial.55 Although the addition of sabatolimab was associated with numerically higher CR rates (19.6% vs 14.3%,) and improved PFS (median, 13.6 months vs 10.1 months), the study did not meet the primary endpoint of OS, with a median OS of 22.31 months versus 18.83 months with azacitidine alone (HR: 0.85 [95% CI: 0.67–1.07]; p=0.0825).56
Similarly, the phase III ENHANCE trial assessed magrolimab, an anti-CD47 antibody, in combination with azacitidine in patients with untreated HR-MDS. Despite promising early-phase data,57 the trial was discontinued following a planned interim analysis that indicated futility, with no improvement in OS.58
In the BRIGHT AML 1019 trial, the Hedgehog pathway inhibitor glasdegib was evaluated in combination with either intensive or non-intensive chemotherapy in newly diagnosed AML patients. However, no OS benefit was seen with the addition of glasdegib in either treatment setting.59
Summary
-
Patients with high-risk MDS have a poor prognosis, with up to 40% progressing to AML within two years. The main treatment options include HMAs such as azacitidine and decitabine, allo-SCT and chemotherapy. Allo-SCT remains the only potentially curative option but is limited by patient eligibility and donor availability.
-
New targeted treatments are being explored, including IDH1/2 inhibitors such as ivosidenib and enasidenib for patients with IDH1/2 mutations and RARA agonists such as tamibarotene for RARA-positive patients.
-
CPX-351, a liposomal formulation of cytarabine and daunorubicin, demonstrated promising results in patients with higher-risk MDS, particularly in those undergoing transplantation. Other agents such as eltanexor and BCL-2 inhibitors are being investigated to overcome resistance to HMAs.
-
New HMAs including cedazuridine and guadecitabine demonstrated improved bioavailability and response rates. Inflammatory pathway inhibitors such as emavusertib are also being developed to increase treatment options for patients with R/R disease.
Conflict of interest
The author has declared that the study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author has declared that no financial support was received from any organization for the submitted work.
Author contributions
The author has created and approved the final manuscript.