



_https___biorender.com_jk9alwd.jpg)
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common type of non-Hodgkin lymphoma (NHL), accounting for approximately one-third of all NHL cases, with an estimated 150,000 new cases annually.1–4 While most patients are cured with upfront chemoimmunotherapy, 30–40% experience disease relapse.4,5 Despite extensive efforts to improve the first-line standard-of-care regimen rituximab plus CHOP (cyclophosphamide, doxorubicin, vincristine and prednisone) by the substitution of rituximab by obinutuzumab (GOYA) or the addition of bortezomib (REMoDL-B), ibrutinib (PHOENIX) or lenalidomide (ROBUST), the POLARIX trial was the only study to show a significant improvement in progression-free survival (PFS) by adding the CD79b-directed antibody-drug conjugate (ADC) polatuzumab vedotin (Pola) to rituximab plus cyclophosphamide, doxorubicin and prednisone (R-Pola-CHP) (HR: 0.73 [95% CI: 0.57–0.95]; p=0.02).5,6 However, no significant overall survival (OS) advantage was observed (HR: 0.87 [95% CI: 0.641–1.175]).7 Based on these data, R-CHOP and R-Pola-CHP are considered the current standard-of-care regimen for the primary treatment of DLBCL. For older patients (>80 years) who often do not tolerate the full-dose R-CHOP regimen, dose-attenuated R-mini-CHOP remains the most frequently used treatment option.4,8,9
Here, we present the case of an 85-year-old woman with DLBCL who was successfully treated with tafasitamab plus lenalidomide after progressing on the R-mini-CHOP regimen.
Case presentation
The 85-year-old female patient was admitted with an indolent swelling of the left eyebrow. An excisional biopsy performed by her general practitioner revealed the diagnosis of a DLBCL. Immunohistochemical analysis showed positive staining for CD10, CD20, BCL2, BCL6 and partially for MUM1, while CD21, CD23 and CD30, along with a large panel of carcinoma and melanoma markers, were negative. The Ki-67 proliferation index was 90%. C-myc immunohistochemistry exhibited negative nuclear staining and Epstein-Barr virus-encoded region (EBER) in situ hybridization was also negative. Further fluorescence in situ hybridization (FISH) analysis demonstrated a BCL2 and MYC rearrangement, confirming a prognostically poor double-hit DLBCL.
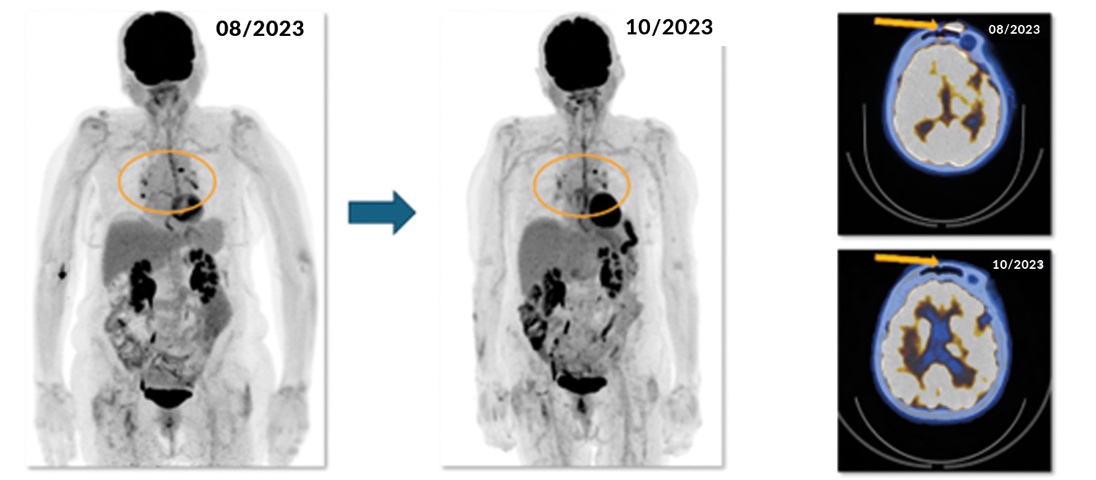
Following the establishment of the diagnosis, staging was completed using 18F-fluoro-deoxyglucose positron emission tomography/computed tomography (18F-FDG-PET/CT). The imaging revealed 18F-fluoro-deoxyglucose (18F-FDG) uptake in the left forehead and mediastinal lymph nodes, corresponding to an Ann Arbor stage IAE to IIAE because the mediastinal lymph node uptake was considered potentially benign (reactive) (Figure 1). Despite the double-expressor/double-hit status,1,4,10 which represents an uncommon DLBCL subset accounting for 5–7% of cases and is associated with inferior outcomes, the patient’s Revised International Prognostic Index (R-IPI) score11 was 2/5. This score, assigned based on age >60 years (one point) and Eastern Cooperative Oncology Group (ECOG) performance status (one point), indicated a good prognosis with an estimated 4-year PFS and OS of approximately 80%.
_initial_staging_with__18_f-fluoro-deoxyglucose_positron_emission_tomography_computed_to.jpeg)
For 20–25% of the DLBCL population, R-CHOP is not a feasible treatment option,4 and in this case, it was deemed unsuitable due to the patient’s age, frailty and reduced performance status, which was not attributable to lymphoma. Based on this, the patient received six cycles of R-mini-CHOP,1–4,8,9 which were successfully completed with the support of granulocyte-colony stimulating factor (G-CSF) without any relevant complications or treatment delays.
Interim staging with an 18F-FDG-PET/CT scan after three cycles exhibited a complete metabolic and morphological response (Figure 2). However, during the second and last cycles of rituximab maintenance treatment, the patient developed a large cervical tumor mass along with an elevated lactate dehydrogenase (LDH) level. This prompted an earlier-than-planned 18F-FDG-PET/CT scan, which confirmed disease recurrence in the right neck but did not reveal any additional lymphoma manifestations (Figure 3).


The patient was diagnosed with primary refractory DLBCL, defined as disease recurrence during or less than six months after the initial therapy. Based on the results of the L-MIND trial,12 she received tafasitamab and lenalidomide. The key consideration for selecting this treatment regimen was its application in an outpatient setting, as the patient had experienced episodes of delirium during previous hospitalizations. Following the recommended schedule, tafasitamab was administered at the standard dose of 12 mg/kg (700 mg absolute) on days 1, 4, 8, 15 and 22 during the first 28-day cycle and on days 1, 8, 15 and 22 during the second and third cycles. Starting from the fourth cycle, tafasitamab was administered on days 1 and 15. Despite concerns regarding the tolerability of the standard 25 mg starting dose of lenalidomide, the patient received this dosage, given that she had not developed any higher-grade cytopenias during the previous therapy. However, due to a history of unsteady gait and cranial polyneuritis following Borrelia burgdorferi infection one year before the DLBCL diagnosis, close monitoring for polyneuropathy was obligatory.
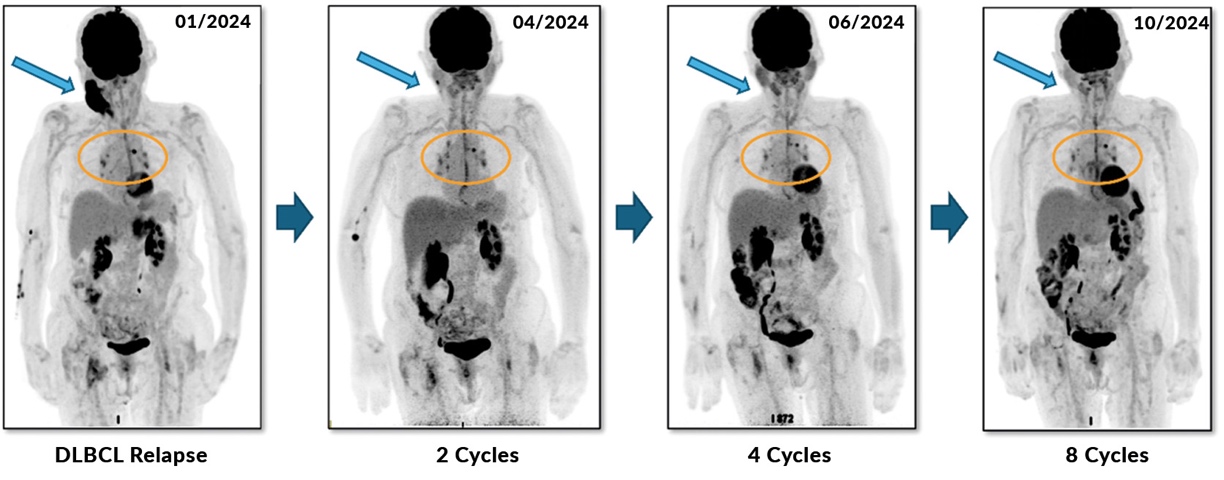
The patient showed a rapid clinical response after only two weeks of treatment. By the end of the second cycle, an FDG PET/CT scan demonstrated a subtotal metabolic and morphological response, which further deepened throughout the course of treatment (Figure 4). After completing the fourth cycle, the patient achieved a CR for the first time, which is currently ongoing.

In May 2024, the patient developed recurrent swelling at the right neck but fine-needle aspiration ruled out a possible second DLBCL relapse. The specimen showed necrobiotic changes with negative immunohistochemistry for CD20 and CD79a, providing no evidence of second lymphoma relapse. The swelling spontaneously regressed following the diagnostic intervention.
By the time this case report was submitted, the patient had completed 12 cycles of lenalidomide. During the 12 cycles, the patient experienced no toxicities requiring a dose reduction of either lenalidomide or tafasitamab. Treatment was delayed only once due to moderate anemia, which was managed with darbepoetin alfa when the hemoglobin levels dropped below 10 g/dL. Overall, treatment tolerability was excellent, with polyneuropathy never exceeding grade 1, as classified by the Common Terminology Criteria for Adverse Events version 6.0 (CTCAE v6.0).
Discussion
To our knowledge, this report represents the first documented case of primary refractory double-hit DLBCL successfully treated with tafasitamab and lenalidomide. This is of particular interest, since these cases have been excluded in the L-MIND trial.4,5
While recurrent DLBCL occurring more than 12 months after first-line therapy is still managed with high-dose salvage chemotherapy and autologous hematopoietic stem-cell transplantation (ASCT) according to current recommendations, chimeric antigen receptor (CAR) T-cell therapy has become the new standard of care for primary refractory DLBCL and cases relapsing within 12 months, which is supported by the positive results of the ZUMA-7 and TRANSFORM trials.5,13,14 However, a significant proportion of patients are ineligible for these treatment approaches, highlighting an urgent need for alternative, more tolerable treatment options.
Tafasitamab in combination with lenalidomide was the first regimen approved for this patient population, receiving U.S. FDA approval in July 2020, EMA approval in June 2021 and Swissmedic approval in June 2022. According to its label, patients must have received at least one previous line of treatment, including a CD20-directed monoclonal antibody and must be ineligible for ASCT. The registrational L-MIND trial demonstrated an overall response rate (ORR) of 57.5%, with 42% of patients achieving a CR.12,15 These responses were durable with a median duration of response (DoR) of not reached (NR) after the final analysis at five years (95% CI: 9.1–NR). The median PFS and OS were 11.6 months (95% CI: 9.1–NR) and 33.5 months (95% CI: 18.3–NR), respectively.
An alternative approved for R/R DLBCL is the three-drug regimen consisting of polatuzumab vedotin, rituximab and bendamustine (Pola-BR). It was approved based on the randomized phase Ib/II trial GO29365, which included an expanded Pola-BR cohort of 106 patients.16,17 The study reported a median PFS of 9.2 months with Pola-BR compared with 3.7 months with BR alone (HR: 0.39 [95% CI: 0.23–0.66]; p<0.0003) and a median OS of 12.4 months compared with 4.7 months, respectively (HR: 0.42 [95% CI: 0.24–0.72]; p=0.001). The ORR in the Pola-BR arm was 62.5% with a CR rate of 52.5% and a median DoR of 10.9 months, compared with an ORR of 25.0% in the BR arm, with a CR rate of 22.5% and a median DoR of 10.6 months (HR for DoR: 0.60 [95% CI: 0.25–1.43]; p=0.25). The extension cohort confirmed the findings for Pola-BR, showing a slightly shorter PFS (median, 6.6 months [95% CI: 5.1–9.2]), but overall similar results, including a median OS of 12.5 months (95% CI: 8.2–23.1), an ORR of 56.6%, a CR rate of 52.8% and a median DoR of 9.5 months (95% CI: 7.9–12.1).
Glofitamab, a CD20xCD3 bispecific antibody, was investigated in a phase I/II trial that enrolled DLBCL patients with at least two prior lines of therapy and an ECOG PS of 0–1.18 The trial reported an ORR of 52% (95% CI: 32–48) and a CR rate of 39% (95% CI: 32–48), with a median DoR of 18 months (95% CI: 13.7–NR). In a supporting cohort exploring long-term outcomes in patients achieving a CR, the median CR duration was 34.2 months (95% CI: 17.9–NR). The median PFS and OS were 4.9 months (95% CI: 3.4–8.1) and 11.5 months (95% CI: 7.9–15.7), respectively. In the context of this case, it is worth highlighting that for patients with double-hit or double-expressor lymphoma (accounting for 10% of the study population), the CR rate was lower at 25% (95% CI: 9–49) and 20% (95% CI: 4–48), respectively.
Another treatment option for patients with refractory DLBCL is the CD19-directed ADC loncastuximab tesirine, which carries a payload acting as an alkylating agent. In the phase II LOTIS-2 trial, loncastuximab tesirine demonstrated an ORR of 48% (95% CI: 39.9–56.7) and a CR rate of 24.1% (95% CI: 17.4–31.9).6,19 The median DoR, PFS and OS were estimated at 13.4 months (95% CI: 6.9–not estimable), 4.9 months (95% CI: 2.9–8.3) and 9.5 months (95% CI: 17.4–31.9). These results led to its approval by the U.S. FDA and EMA; however, the Swissmedic has withdrawn the approval.
Selinexor, an exportin (XPO1) nuclear export inhibitor, has received U.S. FDA approval for its use in patients with DLBCL, although both EMA and Swissmedic have not approved it yet for this indication. In the phase IIb SADAL trial, selinexor showed a rather moderate ORR of 28% (95% CI: 20.7–37.0) and a CR rate of 12% (95% CI: 6.8–18.7).20 The median DoR was 9.3 months (95% CI: 4.8–23.0), which extended to 23.0 months (95% CI: 10.4–23.0) in patients achieving a CR. The median PFS was 2.6 months (95% CI: 1.9–4.0) and the median OS was 9.1 months (95% CI: 6.6–15.1).
As the only novel therapy evaluated in a randomized phase III trial so far is the combination of glofitamab, gemcitabine and oxaliplatin (GemOx) versus R-GemOx (the STARGLO study),21 the optimal treatment choice for R/R DLBCL remains unclear. Although the CAR T-cell trials TRANSFORM and ZUMA-7 specifically included patients with primary refractory disease,13,14,22,23 the proportion of enrolled patients with double-hit, triple-hit or double-expressor lymphoma did not exceed 15% in any of these studies.
In a real-world setting, tafasitamab in combination with lenalidomide was compared to Pola-BR, lenalidomide and rituximab (R2) and CAR T-cell therapies in the RE-MIND2 study.24 This study was designed to contextualize treatment outcomes and support clinical decision-making. In the non-randomized data set, the inverse probability weights method (IPTW) was used to minimize selection bias. The results suggested a significant OS benefit of tafasitamab plus lenalidomide compared with both Pola-BR (HR: 0.441 [95% CI: 0.203–0.956]; p=0.034) and R2 (HR: 0.435 [95% CI: 0.224–0.847]; p=0.012). When compared with CAR T-cell therapies, OS outcomes were similar (HR: 0.953 [95% CI: 0.475–1.931]; p=0.8929). With a median OS ranging from 20.1 to 24.6 months, the outcomes across the tafasitamab plus lenalidomide arms were highly consistent.
Overall, each of the discussed regimens provides the potential for long-lasting remissions, especially when a CR is achieved. However, there are significant differences in terms of tolerability, accessibility, costs, feasibility for outpatient administration and CR rates, which can impact treatment selection in clinical practice. The results of the clinical trials investigating different regimens in second-line and later settings are summarized in Table 1.
Taken together, tafasitamab in combination with lenalidomide represents a highly effective treatment option with an excellent safety profile, even for very frail patients with R/R DLBCL and prognostically poor double-hit biology.
Conclusion and clinical takeaways
This case illustrates that double-hit DLBCL represents a major treatment challenge especially when it occurs in elderly, frail patients. When CAR T-cell therapies are not feasible in the primary refractory disease setting, the treatment options are limited. Since these patients have been for the most part excluded in the L-MIND trial (primary refractory disease, 18%; double-hit DLBCL, 0%), this case report adds to the currently available evidence and demonstrates that tafasitamab plus lenalidomide is an effective therapeutic option in primary refractory, double-hit DLBCL.

Acknowledgements
We thank Dr Ahmed Haider for his assistance in creating the figures. We would also like to acknowledge the valuable support of our dedicated nursing team.
Ethics approval and consent to participate
Ethics approval was not required for the study. Written consent for further use of patient data was obtained.
Consent for publication
Consent for publication was obtained.
Availability of data and materials
All patient data that support this case report are included in the anonymized form in the published article.
Conflict of interest
AM has provided a consulting, advisory or speaker role for Amgen, Astellas, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Gerresheimer, GSK, Incyte, Janssen, Merck, MSD, Novartis, Roche, Regeneron, Sanofi, Servier, Takeda and Vifor, has received research funding from AstraZeneca (personal), Bayer (personal), Gerresheimer (personal) and Merck & Cie (institutional), has intellectual property interests relating to Merck & Cie (not related to this report), has been paid to provide expert testimony for Sanofi and has reported travel/accommodation expenses paid for by Amgen, Astellas, Boehringer Ingelheim, Daiichi-Sankyo, Janssen, Merck, Roche, Sanofi and Servier. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way. Other authors declared that the manuscript was written in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
Preparation of this article was financially supported by Incyte Inc. The supporting company did not have any decision-making role in the development of the manuscript and did not influence its content in any way.
Author contributions
All authors contributed to and approved the final manuscript.