Introduction
AML is a fast-progressing myeloid neoplasm caused by the clonal expansion of abnormal, immature white blood cells in the bone marrow.1 Its clinical and genetic profiles are highly diverse, which greatly influences prognosis and treatment strategies.2–4 FMS-like tyrosine kinase 3 (FLT3) is one of the most commonly mutated genes in AML, appearing in about 30% of cases.5 The mutation patterns are classified into two primary subtypes: internal tandem duplications (FLT3-ITD; about 25% of all AML cases) and tyrosine kinase domain (FLT3-TKD2; 7–10% of all AML cases) mutations. Additional mutations have been described in other kinase domains, but due to the rarity of these mutations the clinical impact remains elusive.6–9 FLT3-ITDs are best evaluated and associated with a particularly poor prognosis due to higher relapse rates and reduced overall survival (OS) compared to other AML subtypes.10 As gain-of-function FLT3 mutations drive oncogenesis and play a central role in leukemia biology, mutant-FLT3 marks an ideal target for therapeutic intervention.
Over the past three decades, major advances in comprehending and targeting mutant-FLT3 have significantly transformed the treatment of FLT3-mutated AML.5 Efforts to harness FLT3 inhibitors have led to substantial breakthroughs in improving remission rates and extending patient survival. However, despite this progress, challenges remain, and ongoing research continues to explore the limitations of current therapies and opportunities for new approaches.
Historical overview of the development of FLT3 inhibitors
Internal tandem duplications within the juxtamembrane and TK1 domain of FLT3 were first identified in 1998.11 Further studies revealed that FLT3-ITD gain-of-function mutations lead to aberrant activation of FLT3 signaling, which was linked to enhanced myeloproliferation12,13 validating it as a compelling target for therapeutic intervention. Preclinical studies demonstrated that inhibiting mutant-FLT3 could effectively suppress leukemic cell growth, prompting efforts to develop FLT3-targeted inhibitors.14–17 By 2005, clinical evaluation of the first-generation FLT3 inhibitors such as sunitinib, sorafenib, midostaurin, tandutinib and lestaurtinib in mutant AML showed promise.18–25 These single-agent trials demonstrated reductions in leukemic burden, but complete remissions (defined as <5% blasts in the marrow together with adequate hematopoietic recovery) have rarely been achieved in these trials.19,21,26 This indicated that monotherapy alone was insufficient for durable remission, underscoring the need to incorporate FLT3 inhibitors into broader therapeutic strategies.27
The feasibility of combining FLT3 inhibitors with standard chemotherapy (ChT) was established by 2004.28–31 This strategy aimed to enhance remission rates and leverage the cytotoxic synergy between FLT3 inhibitors and cytotoxic agents. PKC412 (midostaurin) was the most advanced FLT3 inhibitor in clinical development32,33 and by 2008, the phase III RATIFY (CALGB 10603) trial (NCT00651261) was launched to confirm the clinical benefits of combining midostaurin with ChT in newly diagnosed FLT3-mutated AML patients.23 The publication of the RATIFY trial results in 2017 marked a pivotal moment. This double-blind, randomized study demonstrated a 22% reduction in the risk of death in patients treated with midostaurin plus ChT compared to those treated with ChT alone. Subgroup analyses revealed durable benefits regardless of FLT3 subtype, whether ITD or TKD, and across varying allelic ratios. Based on these results, midostaurin became the first FLT3-targeting therapy approved for use in newly diagnosed FLT3-mutated AML in the US and EU in 2017.23,34,35
The development of second-generation FLT3 inhibitors offered enhanced selectivity and potency over first-generation multikinase agents, such as midostaurin. Gilteritinib, which targets both FLT3-ITD and FLT3-TKD mutant isoforms, proved potent activity as a monoagent to induce hematologic remission rates with a superior efficacy rate when compared to conventional care regimens in the relapsed/refractory (R/R) situation and consequently was approved in 2018 for R/R FLT3-mutated AML,36,37 with regulatory approvals later extended to Japan,38 Europe39 and Switzerland.40,41 In the meantime, a third inhibitor, quizartinib, made its way to approval in Japan in 2019 for treating R/R FLT3-ITD-mutated AML,42,43 as well as to approval in 2023 in the US44 and EU45 for use in frontline settings, which represents another milestone.46
In addition to the three approved FLT3 tyrosine kinase inhibitors with options spanning from first-line therapy to maintenance to salvage therapy, a fourth (multikinase) FLT3 inhibitor, sorafenib, is at hand and widely recommended for post-allogeneic hematopoietic stem cell transplantation (HSCT) maintenance therapy47,48 (whereas formal approval is lacking).
The focus is now shifting to the development and integration of more kinase-specific FLT3 inhibitors49 and refining therapeutic combinations, e.g. in combination with hypomethylating agents.50
Advances and insights from key studies
Setting the standard with midostaurin monotherapy
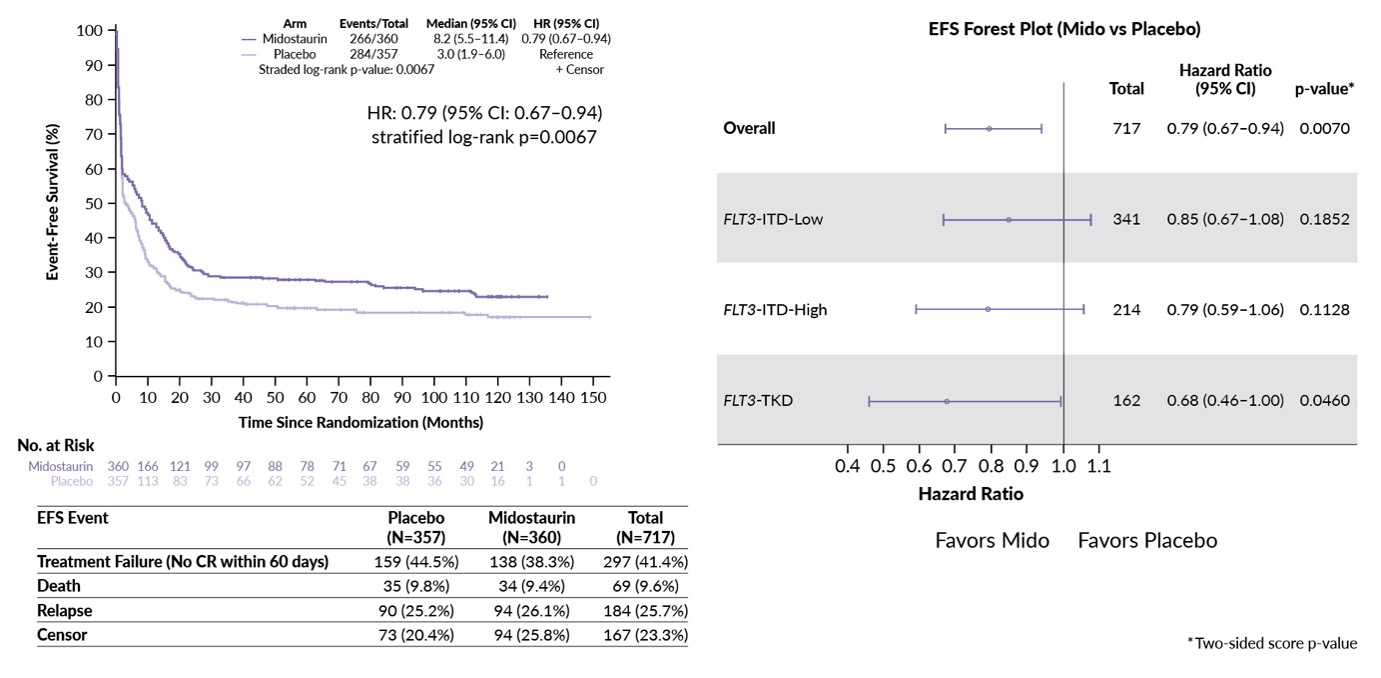
The phase III RATIFY trial provided robust evidence for incorporating midostaurin into induction and consolidation ChT, with initial findings published in 2017. At a median follow-up of 59 months, a clear benefit of adding midostaurin to intensive ChT was demonstrated.23 Event-free survival (EFS) was significantly enhanced, with a median of 8.2 months for midostaurin versus 3.0 months for placebo. Additionally, the risk of death was reduced by 22% (p=0.009), with a 4-year OS of 51.4% in the midostaurin group compared to 44.3% in the placebo group. These results led to the global approval of midostaurin as a standard therapeutic option for newly diagnosed FLT3-mutant AML.
Long-term results from the 10-year follow-up, presented at ASH 2024, confirmed the durability of the EFS benefit.51 The median EFS remained 8.2 months for midostaurin versus 3.0 months for placebo (Figure 1), while the 10-year OS was marginally higher for those receiving midostaurin, at 43.7% compared to 38.6% for placebo.
_with_midostaurin_(mido)_at_10_years_follow-up_in_the_rafity_tria.jpg)
Subgroup analysis confirmed midostaurin’s benefits across all FLT3 mutation subtypes, including both high- and low-allelic-ratio FLT3-ITD and FLT3-TKD mutations.51 Patients with co-mutated NPM1 demonstrated notably better outcomes, reinforcing the relevance of genomic interplay in treatment response. Gender-specific analyses revealed significant OS benefits in men (10-year OS rate, 47.3%) but not in women, highlighting the need for further exploration of biological or treatment-related disparities.
Additionally, the trial emphasized the critical role of allogeneic HSCT in first complete remission (CR1).51 Transplanted patients achieved a 10-year OS of 56%, compared to 35.8% for non-transplanted patients. Among CR1 recipients, midostaurin showed an additional survival trend, with an OS rate of 61.5% compared to 49% for placebo, further underscoring the importance of midostaurin treatment in the induction phase to improve long-term survival rates post-transplantation. Of note, randomization to maintenance therapy with midostaurin reduced the cumulative incidence of relapse in the European LeukemiaNet (ELN) 2017 favorable and intermediate risk patients – but not in those with adverse risk disease (HR: 0.71, 0.47 and 1.01, respectively). Maintenance with midostaurin had no effect on OS, however, treatment-related deaths were higher in the midostaurin group (17 vs 5), arguing for for long-term monitoring and toxicity management.
Long-term results from the RATIFY trial demonstrate that midostaurin, when combined with ChT, provides a durable EFS benefit for FLT3-mutant AML patients.51 While the OS advantage diminished over time, likely due to aging and evolving treatments, these findings underscore the importance of FLT3-targeted therapies, HSCT in CR1 and the value of long-term follow-ups in advancing precision medicine for AML.
Gilteritinib in R/R AML
Insights from the phase III ADMIRAL trial (NCT02421939) demonstrated that gilteritinib significantly improved OS in R/R FLT3-mutated AML compared to salvage chemotherapy.52 A median OS of 9.3 months marked a substantial improvement over historical outcomes, making gilteritinib a new standard for relapsed patients. Additionally, the phase III COMMODORE trial (NCT03182244) confirmed that gilteritinib notably enhanced OS and EFS in a primarily Asian patient population, reinforcing the findings of the ADMIRAL trial on the efficacy of gilteritinib in FLT3-mutated R/R AML regardless of ethnicity.53
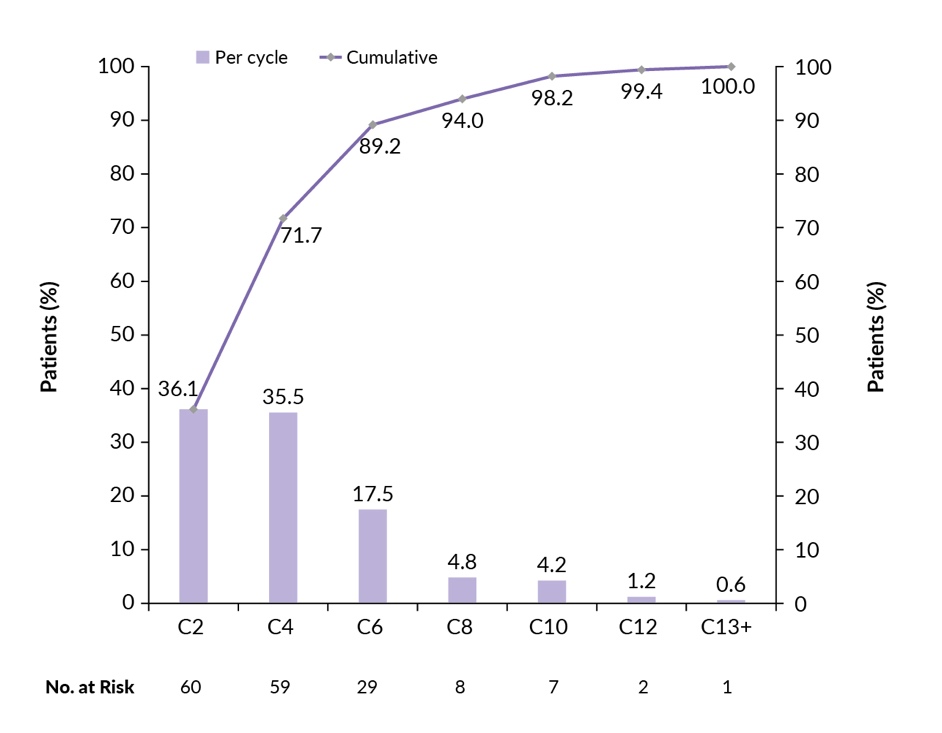
The post hoc pooled analysis of the gliteritinib arms of the ADMIRAL and COMMODORE trials was presented at ASH 2024, analyzing the timing of response to gliteritinib monotherapy.54 The study focused on early responders (ERs), who achieved composite complete remission (CRc) by cycle 2, and late responders (LRs), who achieved CRc after cycle 3. CRc was defined as the sum of complete remission (CR), CR with incomplete hematologic recovery (CRi) and CR with incomplete platelet recovery (CRp).
The analysis included 205 gliteritinib-treated CRc responders.54 Most patients (almost 90%) achieved CRc within six cycles of gliteritinib monotherapy (Figure 2). LRs (38.7%) were more likely than ERs (21.7%) to achieve complete remission with full count recovery and undergo hematopoietic stem cell transplantation (HSCT) in CR (60.0% vs. 21.4%). The median OS was longer for LRs (10 months) compared to ERs (9 months), with better 12- and 24-month OS rates for LRs. LRs also experienced fewer drug-related grade 3 or higher adverse events (AEs) and lower rates of treatment discontinuation due to relapse or progression compared to ERs. These findings suggest that continuing gliteritinib monotherapy in patients with R/R FLT3 mutated AML, particularly in those who tolerate the drug, can lead to late and sustained remission. The study highlights the need to differentiate the timing of response assessment and treatment continuation decisions for gliteritinib from those for salvage ChT.

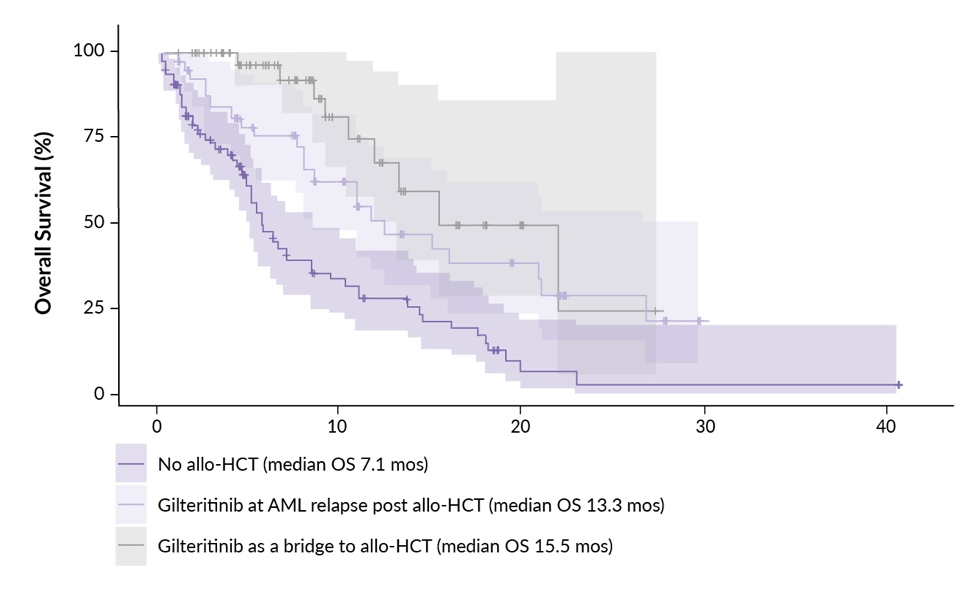
Real-world data further support these findings.55 Results of a retrospective, multicenter, observational analysis conducted across 22 Italian centers were also presented at ASH 2024. It included 149 adult patients with R/R FLT3-mutated AML (relapsed, n=107; refractory, n=42) who received gilteritinib as salvage therapy. Treatment was administered either under an early-access program starting January 24, 2018, or after approval of gilteritinib by the Italian Drug Agency (AIFA) in May 2020. The study assessed treatment response, EFS and OS using the European LeukemiaNet 2017 criteria.4 Gilteritinib was used as monotherapy in 53% of patients, while 47% underwent allogeneic HSCT either post-relapse or as a bridge to transplant.
Key results showed that 50% of patients achieved CR/CRi, with a median OS of 10.6 months and EFS of 4.64 months.55 Patients undergoing allogeneic HSCT after gilteritinib had better outcomes, with a median OS of 15.5 months compared to 7.1 months for gilteritinib-only treatment (Figure 3). These findings align with those of the ADMIRAL trial,52 highlighting gilteritinib as an effective treatment option and a potential bridge to transplant.55 Further analysis of the full cohort is ongoing.
_outcomes_in_patients_receiving_gliteritinib_with_or_witho.jpeg)
Crenolanib in newly diagnosed and R/R FLT3 mutated AML
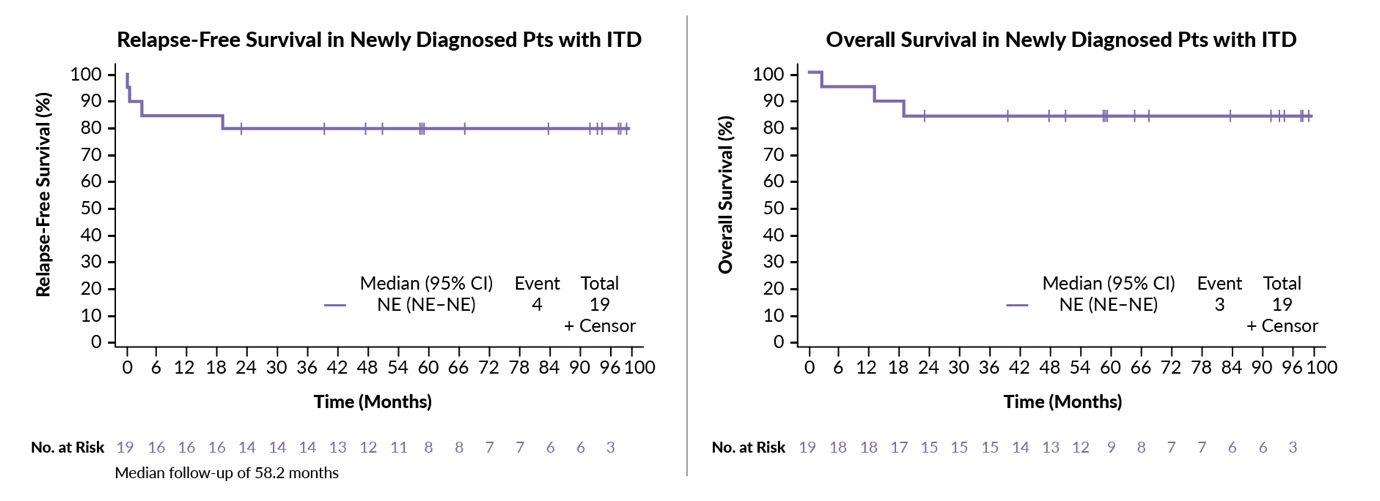
Crenolanib, a second-generation potent inhibitor targeting both FLT3-ITD and FLT3-TKD mutations, was evaluated in a phase II pilot study (ARO-006; NCT02400255) presented at ASH 2024.49,56 This study assessed the safety and efficacy of crenolanib maintenance therapy in 30 adult patients (median age, 53.5 years) with FLT3-mutated AML following allogeneic HSCT.56 Newly diagnosed FLT3-ITD patients transplanted in first remission achieved an OS of 84% and relapse-free survival (RFS) of 79% (Figure 4). Crenolanib demonstrated a favorable safety profile. Common AEs included nausea (57%), vomiting (47%) and diarrhea (47%), which were generally manageable with supportive care. Over a median follow-up of approximately five years, daily crenolanib maintenance was well tolerated, with no significant myelosuppression or worsening of graft-versus-host disease (GvHD), and only five reported GvHD cases. Notably, no patient exhibited severe hepatic toxicity. Pivotal trials are planned to validate these results and further investigate the role of crenolanib in the post-transplant setting.
_and_overall_survival_(os)_on_crenolanib_maintenance_after_allo.jpeg)
Quizartinib’s role in frontline therapy
Quizartinib has emerged as a potent treatment option for FLT3-ITD-mutated AML. Two studies presented at the 66th ASH Annual Meeting & Exposition by Dr Sudhir Unni57 and Dr Michelle Hyunju Lee58 compared the efficacy of quizartinib and midostaurin in patients with FLT3-ITD mutated AML, highlighting quizartinib’s potential advantages in this high-risk population. The first study utilized a matching-adjusted indirect comparison (MAIC) of data from the QuANTUM-First46 (quizartinib) and RATIFY23 (midostaurin) trials.57 Adjustments for baseline differences, such as age, platelet counts, and NPM1 mutation status, were made using propensity score weighting. Quizartinib significantly reduced relapse rates compared to midostaurin (HR for CIR MAIC-adjusted: 0.42), suggesting deeper and longer remission durations. While quizartinib showed numerically favorable OS (HR MAIC-adjusted: 0.82) and similar CRc rates, these differences were not statistically significant.57
The second study was a real-world retrospective analysis conducted across five US academic hospitals.58 It compared quizartinib and midostaurin in newly diagnosed FLT3-ITD-positive AML patients treated with standard cytarabine and anthracycline (7+3) induction and ongoing intensive post-remission treatment. Quizartinib achieved a significantly higher CRc rate (85% vs 73%; p=0.004) and eliminated the need for re-induction therapy, compared to 17.3% of midostaurin-treated patients. No relapses were observed in the quizartinib group during the limited follow-up, while 32% of midostaurin-treated patients relapsed. Quizartinib also resulted in fewer treatment interruptions (5% vs 25.5%; p=0.04), with comparable safety profiles between the two groups.
Overall, both studies underscore quizartinib’s effectiveness in achieving higher CRc rates and reducing relapse risk compared to midostaurin.57,58 The MAIC analysis highlighted the significant advantage of quizartinib in relapse prevention, while the real-world study demonstrated better CRc rates, fewer re-induction requirements, and similar safety outcomes.
Conclusion
This review summarizes the current treatment landscape of FLT3-mutated AML and tracks the evolution of its treatment over three decades. Midostaurin serves as a pivotal breakthrough, becoming the first FLT3-targeting therapy for newly diagnosed patients and setting the stage for further advancements. Insights from ASH 2024 bring attention to second-generation inhibitors such as gilteritinib, recognized for its efficacy in R/R AML; crenolanib, showing promise in post-transplant maintenance; and quizartinib, demonstrating higher and deeper remission rates and a reduced risk of relapse in frontline therapy. Real-world data and ongoing trials emphasize the potential of personalized approaches, yet underscore that challenges such as relapse and resistance persist. This review highlights a continuing need for innovation to refine therapeutic strategies to improve sustained remissions and survival outcomes for this complex and higher-risk AML population.
Conflict of interest
The author received advisory board honoraria in 2023/2024 from Otskua, Servier and JAZZ and holds patents with the University of Tübingen (U.S. 13/753,354, WO 2012/016979, PCT/EP2011/063283, further patent submitted). These funding entities did not play a role in the development of the manuscript and did not influence its content in any way.
Funding
The article processing charges (APC) were supported by Daiichi Sankyo. The sponsor did not have any role in the development of the manuscript and did not influence its content in any way.
Author contributions
The author has created and approved the final manuscript.