Introduction
As the global population ages, cancer has become increasingly prevalent among older adults, presenting unique challenges for oncologic treatment. Age-related physiological changes, such as impaired organ function (i.e., renal or cardiac), frailty, reduced bone marrow reserves and altered pharmacokinetics, complicate treatment decisions and affect outcomes.1–3
Accordingly, older cancer patients often present with a high burden of comorbidities and prevalence of geriatric syndromes, such as frailty. The latter is defined as a state of reduced physiological reserve and increased vulnerability to physical stressors.4 Frailty alone is a particularly strong predictor of adverse outcomes in oncology, impacting survival, treatment response and quality of life (QoL).5–8 It increases the risks of treatment-related toxicities, often leading to under- or over-treatment, which compromises outcomes. The growing number of older cancer patients highlights the importance of developing personalized cancer therapies that strike a balance between effectiveness and tolerability, especially for frail older adults, demanding thorough informed decision-making processes focusing on the patient’s personal preferences.
Immune checkpoint inhibitors (ICIs), which target immune-regulatory pathways such as programmed cell death protein 1 (PD-1)/programmed death-ligand 1 (PD-L1) and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), have revolutionized cancer treatment by enhancing the ability of the immune system to eliminate tumor cells.9,10 However, the aging immune system undergoes complex alterations, collectively referred to as immunosenescence.11 These changes include a decline in naïve T cell populations, reduced immune surveillance and a pro-inflammatory state termed “inflammagin”,12–14 all of which can influence the effectiveness of ICIs. Despite their promise, ICIs remain insufficiently investigated in frail, older patients due to their limited representation in clinical trials, predominantly enrolling younger and fitter individuals. Existing data on the safety and efficacy of ICIs in frail populations are sparse, raising concerns regarding the generalizability of trial outcomes. Immune-related adverse events (irAEs) associated with ICIs, ranging from mild skin reactions to severe organ inflammation,15 may pose additional concerns in frail older adults who may have less capacity to recover from such toxicities.
Understanding the interplay between frailty, immunosenescence and ICI therapy is critical for optimizing cancer care in older adults. Present frailty can modulate the immune microenvironment, potentially impacting the efficacy and tolerability of ICIs. Moreover, standardized tools to assess frailty are not routinely incorporated into oncological practice or clinical trial designs. This lack of robust frailty-focused research generates a significant gap in evidence-based guidelines for managing older, frail patients with ICIs. This review article summarizes the key findings from recent studies evaluating the safety and efficacy of ICIs in older and frail patient populations.
Impact of age on outcomes with immunotherapy in patients with melanoma
In this study by Betof et al., data were retrospectively collected from 254 patients with metastatic melanoma treated with anti-PD-1 and/or PD-L1 monoclonal antibodies (mAbs) at Massachusetts General Hospital (MGH) and Vanderbilt University Medical Center from May 2009 to April 2015.16 Of the 254 patients included, 22.4% were <50 years old, 33.5% were aged 50–64 years, 25.6% were aged 65–74 years and 18.5% were ≥75 years old. Younger patients were more likely to have a BRAF mutation (p=0.0001). Among those with a BRAF mutation (n=59), 71.2% received BRAF-targeted therapy prior to initiating PD-1 inhibitor therapy. Most patients received anti-PD-1 therapy (92.5%).
The median follow-up was 16.0 months.16 After PD-1 inhibitor initiation, the median overall survival (OS) for the entire cohort was 22.0 months and was comparable between age groups (age <50 years, 22.9 months; age 50–64 years, 25.3 months; age 65–74 years, 22.0 months; age ≥75 years, 24.3 months). Multivariable Cox proportional hazard model (reference group ≥75 years) showed no significant difference in OS according to age (HR for <50 years group: 0.9 [95% CI: 0.5–1.8]; HR for 50–64 years group: 0.9 [95% CI: 0.5–1.6]; HR for 65–74 years group: 0.8 [95% CI: 0.6–1.6]).
The median progression-free survival (PFS) for the entire cohort was 5.4 months after initiation of PD-1 inhibitor therapy and was similar between age groups (age <50 years: 4.1 months; age 50–64 years: 6.5 months; age 65–74 years: 5.4 months; age ≥75 years: 7.9 months).16 There was no significant difference in PFS for older versus younger patients (HR age <50 years: 1.0 [95% CI: 0.5–1.8]); HR age 50–64 years: 0.8 [95% CI: 0.5–1.4]; HR age 65–74 years: 0.8 [95% CI: 0.5–1.5]).
In terms of safety, 43.3% of patients experienced any irAEs.16 The most common toxicities were dermatitis (10.6%) and colitis (9.8%). The incidence of arthritis was significantly higher among patients aged 65–74 years (10.8%; p=0.02). Patients aged ≥75 years had non-significantly higher incidences of thyroiditis or endocrine-related toxicity. Notably, there were no significant differences in colitis, hepatitis or pneumonitis between age groups.
Multiorgan immune-related adverse events during treatment with atezolizumab
This post hoc pooled analysis was performed using individual patient data from the OAK (NCT02008227), POPLAR (NCT01903993), BIRCH (NCT02031458) and FIR (NCT01846416) trials.17 Only atezolizumab-treated cohorts were included. The primary objectives were the incidence, grades and time course of irAEs associated with atezolizumab. The secondary objectives were the incidence and grades of treatment-related AEs (TRAEs), PFS and OS.
The analysis included 1,548 patients (age, 57–70 years) who received at least one dose of atezolizumab.17 One or more TRAEs occurred in 65% of patients, with grade 3–5 TRAEs reported in 13% of patients. A total of 730 irAE episodes were reported in 424 patients (27%) who had at least one irAE. The median time of onset was 49 days. Overall, 12% of irAEs occurred within the first 42 days of atezolizumab use. Patients with irAEs were more likely to be Asian and have good performance status (PS), lower C-reactive protein (CRP) levels, differential changes in white cell subpopulations, a good Lung Immune Prognostic Index (LIPI) score and a lower neutrophil-to-lymphocyte ratio score.
Overall, 7.5% of the 730 episodes of irAEs resulted in hospitalization, which was required in almost half of grade 3–4 events and in 5.7% of grade 1–2 events.17 A total of 15% of irAE episodes were treated with systemic corticosteroids; of these, 30% were grade 1–2. Atezolizumab was interrupted in 14% of all episodes and was permanently discontinued in 2.5%. At the time of the last follow-up, 60% of irAE episodes were resolved and 28% of patients had ongoing irAEs. One death due to irAEs (pneumonitis) was reported. Five patients required second-line immunosuppressants for the treatment of irAEs after systemic corticosteroid failure.
Of the 424 patients with irAEs, 340 had one organ-specific irAE (80.2%), while multi-organ irAEs occurred in 5.4% of all atezolizumab-treated patients and 19.8% of all patients with irAEs.17 Most patients with multiorgan irAEs (83.3%) had two organ systems affected by irAEs, 15.5% had three and one patient had four; 12 patients had concurrent-onset irAEs. Patients experiencing multiorgan irAEs were more likely to be Caucasian with an Eastern Cooperative Oncology Group (ECOG) PS of 0, lower baseline CRP level and lower neutrophil-lymphocyte ratio than those who developed single-organ irAEs.
The development of multiorgan irAEs was associated with improved clinical outcomes.17 The objective response rate (ORR) was significantly higher among those who developed multiorgan irAE than those with single-organ irAEs or had no irAEs (42% vs 23% and 12%; odds ratio of 5.32 for multiorgan irAEs and 2.18 for single-organ irAEs [p<0.0001]). Patients with multiorgan irAEs versus single-organ irAEs and no irAEs experienced significantly improved both median PFS (7.2 months vs 4.2 months and 2.7 months; p≤0.001) and median OS (not reached vs 20.1 months and 10.3 months; p<0.001). The HR measured using a time-dependent Cox regression model for OS was 0.47 (95% CI: 0.28–0.78) for multiorgan irAEs (vs no irAEs) and 0.69 (95% CI: 0.57–0.85) for single-organ irAEs (vs no irAEs) (p<0.0001). However, neither the occurrence of multiorgan irAEs (HR: 0.92 [95% CI: 0.62–1.35) nor single-organ irAEs (HR: 0.95 [95% CI: 0.81–1.11]; p=0.74) was associated with an improved PFS in the time-dependent Cox model.
ICIs in older adults with melanoma and other cutaneous malignancies: The Wilmot Cancer Institute experience
This study by Archibald et al. included 120 patients with a diagnosis of melanoma (cutaneous, mucosal or ocular), Merkel cell carcinoma and other cutaneous malignancy treated with ipilimumab, nivolumab or pembrolizumab between 1 January 2011 and 3 April 2017 in the Wilmot Cancer Institute (WCI) at the University of Rochester Medical Center.18 Among all 120 patients receiving ICI therapy, 52 were ≥70 and 68 were <70 years old. Nine patients underwent formal geriatric assessment (GA) (age, 75–92 years): three were evaluated as fit, two as vulnerable and four as frail. In the absence of formal GA, the frail subgroup was defined as any patient having an ECOG PS ≥3, Charlson Comorbidity Index (CCI) score ≥11 and/or falls in the prior six months (n=26 aged ≥70 years). A greater proportion of patients aged <70 years received potentially more toxic regimens than those aged ≥70 years, with dual checkpoint blockade with ipilimumab plus nivolumab given to 5.9% versus 0% of patients, respectively and ipilimumab 3 mg/kg administered to 54% versus 33%.
Overall, 38% of patients experienced irAEs on first-line ICI therapy. Severe irAEs were reported in 22.8% of patients in the overall cohort.18 When stratified by age, 44.1% of younger patients and 21.4% of older patients had irAEs (p=0.158); these percentages were 25.4% versus 19.6% for severe irAEs (p=0.464). Reported irAEs included colitis (n=10), dermatitis (n=8), hypophysitis (n=7), transaminitis (n=6), thyroiditis requiring replacement therapy (n= 5), inflammatory arthritis (n=4), pneumonitis (n=4), immune-mediated myelosuppression (n=1) and immune-mediated systemic inflammation in the absence of infection (n=1). In the older subgroup, irAEs were mainly managed with treatment discontinuation and immunomodulatory medication. Three patients died due to irAEs (age ≥70 years, n=2; age <70 years, n=1).
In the entire study population, 39.3% of patients had a response to first-line ICI therapy.18 There was no significant difference between younger versus older patients, with an overall response occurring in 35.1% versus 44.0% of patients, respectively (p=0.346). Similarly, no significant difference was reported in the response rate between younger and older patients when stratified by disease type (cutaneous vs non-cutaneous).
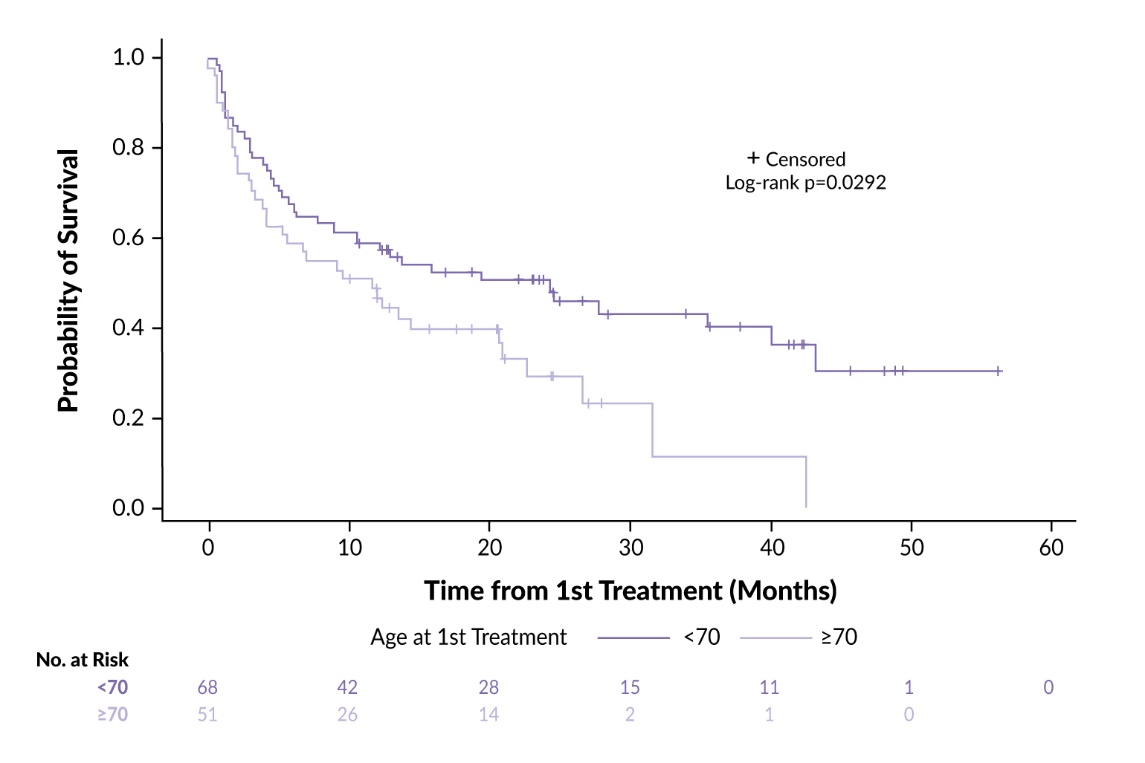
Regarding OS, the older subgroup achieved worse survival outcomes (p=0.029).18 The median OS for patients aged ≥70 was 11.7 months compared with 24.3 months for those aged <70 years (Figure 1). There was a trend toward improved OS in older patients with an ECOG PS <3 compared with those with an ECOG PS of 3 (median OS, 12.0 months vs 1.9 months). This difference is highly relevant, even though it did not reach statistical significance due to the small sample size, particularly in the context of melanoma. Most patients died due to progressive disease (age ≥70 years, 81%; age <70 years, 92%). Among the nine patients with an ECOG PS of 3, seven died, none of whom due to an irAE; 67% died of progressive disease.
In a subgroup analysis, among 40 patients with cutaneous melanoma on first-line PD-1 monotherapy, the ORR was 57.9% for patients aged <70 years (n=21) versus 63.2% for patients aged ≥70 years (n=19) and the rates of severe irAEs were 28.6% versus 31.6%.18 No difference in rates of irAEs was observed between the two age groups (52.4% vs 63.2%; p=0.324).
_of_patients_treated_with_immune_checkpoint_inhibitors_(icis)_by_age_.jpeg)
Frailty and checkpoint inhibitor toxicity in older patients with melanoma
This prospective, observational study evaluated the incidence of grade ≥3 irAEs in patients with melanoma aged ≥70 years who were about to start ICI therapy (nivolumab or pembrolizumab) and were screened using Geriatric-8 (G8) assessment.19 A total of 92 patients were included in the analysis, 26 (29%) of whom were classified as frail. Fit patients were significantly younger and had a better World Health Organization (WHO) PS at baseline compared with frail patients; other baseline characteristics were not significantly different between the fit and frail groups.
The analysis demonstrated that grade ≥3 irAEs occurred in 20% of patients. There was no significant difference in the incidence of grade ≥3 irAEs between fit and frail patients (17% vs 27%; p=0.26).19 However, frail patients were admitted to the hospital because of irAEs significantly more often than fit patients (29% vs 54%; p=0.02) and showed a trend toward increased length of hospitalization (5 vs 8 days; p=0.06). Moreover, more frequent use of immunosuppressants or ICI discontinuation for irAEs were reported in the frail group (36% vs 58%; p=0.06). These data show that frailty may be an indicator of irAE-related adverse sequelae, such as hospital admission suggesting that screening for frailty can be of added value in the decision-making process for older patients who qualify for ICI therapy.
Geriatric assessments in patients with lung cancer and melanoma treated with ICIs: The ELDERS study
The ELDERS study was a prospective observational study including two cohorts: older patients (≥70 years old) and younger patients (<70 years old).20 Participants with advanced/metastatic non-small-cell lung cancer (NSCLC) or melanoma starting single-agent ICI were eligible. The older cohort was assessed for frailty using G8 screening, which, when positive (<15 points), was followed by a holistic set of geriatric assessments. The primary endpoint was the incidence of grade 3–5 irAEs.
A total of 140 patients were enrolled, with 43% of them pretreated and pembrolizumab constituting 92% of treatments on study.20 The older cohort had a significantly higher comorbidity burden (p<0.001) and polypharmacy (p=0.004). While 50% of older patients had a positive G8 screening, 60% on this frail subgroup had a PS score of 0 or 1. There was no significant difference in the incidence of grade 3–5 irAEs between the older and younger cohorts. The use of ICI in older patients was not associated with more high-grade toxicity. The G8 screening identified a subgroup with a higher risk of AEs, and its implementation should be considered in the context of ICI.
Cemiplimab in older patients with squamous cell carcinoma
Treatment options for advanced cutaneous squamous cell carcinoma (cSCC) in older patients are limited owing to concerns regarding treatment tolerability. Several studies have demonstrated the successful use of the anti-PD-1 mAb cemiplimab in older patients with cSCC. In immunocompromised and immunocompetent patients aged >75 years (median age, 83 years) diagnosed with locally advanced or metastatic cSCC who were treated with cemiplimab or pembrolizumab, the median PFS was 8.94 months at the median follow-up of 35.6 months, with the disease control rate (DCR) of 91.4% and complete response (CR) rate of 17.1%.21 TRAEs occurred in 85.6% of patients, predominantly grades 1 or 2. The French CAREPI Study Group conducted a real-life analysis of 245 patients (median age, 77 years) with locally advanced and metastatic SCC. With a median follow-up of 12.6 months, the median PFS was 7.9 months, while the duration of response (DoR) and median OS were not reached. One-year OS was 73% for patients with an ECOG PS <2 compared with 36% for those with PS ≥2. Severe TRAEs were reported in 9% of patients, including one fatal case of toxic epidermal necrolysis.22 An Italian retrospective, observational, multicenter study included 131 patients with advanced cSCC, with a median age of 79 years. The ORR was 58% and the DCR was 71.7%.23 Real-world data from a retrospective cohort study conducted in the Netherlands confirmed the feasibility of cemiplimab for older patients (median age, 76 years) with advanced cSCC. Cemiplimab was well tolerated by geriatric patients with severe comorbidities, achieving a response in 52% of patients, including CR rate of 22%. Common AEs included fatigue (49%), pruritus (32%) and elevated alkaline phosphatase levels (29%).24
Notably, very old patients also responded well to treatment. An 86-year-old patient with an ECOG PS of 3 received four cycles of cemiplimab, achieving a partial response as the best overall response, with only grade 1 AEs such as increased creatine phosphokinase, aspartate aminotransferase and hypomagnesemia.24 Additionally, a 90-year-old patient with metastatic cSCC treated with cemiplimab and locoregional radiotherapy showed significant clinical improvement without severe AEs.25 Together, these data show that cemiplimab is an efficacious and safe treatment option for older patients with cSCC, including those with significant comorbidities and very advanced age.
The efficacy of ICIs in older patients: A meta-analysis and meta-regression
This meta-analysis included a total of 30 randomized controlled trials (RCTs) (phase III, n=28; phase II/III, n=1; phase II, n=1) that reported OS (25 RCTs) and PFS (14 RCTs).26 Of these, 16 trials used PD-1 inhibitors (nivolumab, n=8; pembrolizumab, n=8), six used PD-L1 inhibitors (avelumab, n=2; atezolizumab, n=3; durvalumab, n=1) and six used anti- CTLA-4 (tremelimumab, n=2; ipilimumab, n=4; combination of nivolumab with ipilimumab, n=2). Fourteen RCTs were conducted in first-line settings and 16 RCTs evaluated treatment after previous failure of systemic therapies. NSCLC and melanoma accounted for 39% and 20%, respectively; most trials were performed on NSCLC (n=12) and melanoma (n=6).
The analysis demonstrated no statistically significant difference in OS and PFS for patients across age groups who received immunotherapy.26 The HR for OS between the treatment and comparator groups was 0.77 (95% CI: 0.70–0.85) in the younger age group and 0.77 (95% CI: 0.70–0.85) in the older age group. The HR for PFS between the treatment and comparator groups was 0.75 (95% CI: 0.57–0.99) in the younger age group and 0.82 (95% CI: 0.67–1.01) in the older age group. The subgroup difference among three different age groups (age <65 vs ≥65 vs ≥75 years) based on random-effects models was not statistically significant in terms of OS (p=0.095) and PFS (p=0.613).
Further analysis revealed that in trials with positive outcomes in terms of OS (16/26 trials) and PFS (12/15 trials), the HRs were comparable for both OS (younger group, HR: 0.67 [95% CI: 0.64–0.71]; older group, HR: 0.68 [95% CI: 0.62–0.74]; p=0.85) and PFS (HR: 0.60 for younger vs HR: 0.71 for older patients; p=0.11).26
Subgroup analyses demonstrated no significant difference in both OS and PFS between age groups when stratified by line of treatment (first line and subsequent), type of immunotherapy (anti-PD-1 or anti-PD-L1, anti-CTLA-4, combination of both) and primary tumor type (NSCLC, melanoma and others), except for the melanoma subgroup showing significant differences for PFS between the younger and older patients (p=0.04).26
Comparison of ICI efficacy between younger and older patients: A systematic review and meta-analysis
This was an independent review of PubMed from January 1966 to September 2015.27 Clinical trials that met the following criteria were included: (1) phase II and III trials in patients with cancer; (2) random assignment of participants to treatment with ICI or a control regimen that did not include an ICI; and (3) subgroup comparisons of OS and/or PFS based on age. The primary objective was to compare OS and the secondary objective was to compare PFS between younger and older patients treated with ICIs.
Eight phase III and one phase II RCTs were included in this meta-analysis, with a total of 5,265 patients (ICIs: 2,925; controls: 2,340) from three ipilimumab trials, one tremelimumab trial, four nivolumab trials and one pembrolizumab trial.27 The underlying malignancies included melanoma (five trials), NSCLC (two trials), prostate cancer (one trial) and renal cell carcinoma (one trial).
A total of 4,725 patients from eight trials were included in the OS analysis.27 The pooled HR for OS showed a significant difference between ICIs and controls for both younger patients (HR: 0.75 [95% CI: 0.68–0.82]; p<0.001) and older patients (HR: 0.73 [95% CI: 0.62–0.87]; p<0.001). There was no statistically significant difference in the pooled HRs for OS between the subgroups of younger and older patients (p=0.96). Regarding type of ICIs (anti-CTLA-4 mAb vs anti-PD1 mAb), a significant improvement in OS with anti-CTLA-4 mAbs was observed in both younger and older patients (cut-off age, 65–70 years). In the subgroup of patients receiving anti-PD1 mAb, improved OS was observed in patients treated with anti-PD1 mAb aged <65 and 65–75 years. Exploratory subgroup analysis according to tumor type (melanoma vs others) showed a consistent survival benefit of ICIs in both younger and older groups.
In three anti-PD-1 mAb trials (n=1,394), the pooled PFS data of the younger group (<65 years) favored ICI therapy (HR: 0.58 [95% CI: 0.40–0.84]; p=0.004).27 For the older group, PFS was not significantly different between ICIs and controls, with a trend toward improvement with ICIs (HR: 0.77 [95% CI: 0.58–1.01]; p=0.06). There was no significant difference between the younger and older subgroups (p=0.23).
Discussion
The use of ICIs in the treatment of frail older patients represents a critical area of oncological and geriatric research. While ICIs have demonstrated efficacy in extending survival and improving outcomes across diverse age groups, their application in frail patients remains challenging, primarily due to increased vulnerability to irAEs and the need for individualized treatment considerations.
Evidence regarding the impact of age and frailty on ICI efficacy and toxicity
In this review, we could show that there is reliable and consistent evidence suggesting that neither ICI efficacy nor toxicity is age-dependent. However, many of the referenced studies were meta-analyses from randomized clinical trials, in which highly selected patient populations are enrolled, which are unlikely to include frail patients. The age cut-off in most analyses was 70 or 75 years. However, in daily clinical practice we often weigh treatment decisions in relevantly older patients aged >85 years. These patients are more likely to be frail and there is hardly any evidence for this specific population. Of all the studies referenced in this review, only one study included a functional assessment in addition to age, showing a drastically detrimental effect of poor PS in older patients with malignant melanoma starting ICI therapy. While age alone might not be predictive of efficacy and/or toxicity, older age paired with frailty (as approximated by PS) appears to influence these outcomes. Nevertheless, ICIs appear to demonstrate overall tolerability and safety in older patients with a good ECOG PS (0–1) that is comparable to those observed in younger patients.
Efficacy and frailty: Impact of reduced physiological reserve
Despite the advanced age of many patients with cancer, ICIs exhibit efficacy that is consistent across different populations, including older adults. However, frailty can be associated with a higher risk of severe toxicity.28 In frail patients, reduced immunological and functional reserves may affect treatment response, potentially attenuating the benefits of ICIs. Furthermore, frailty is associated with increased comorbidities and baseline systemic inflammation, which further predisposes to poor outcomes. Regarding the intersection of frailty and treatment tolerance, employing frailty screening tools such as the Frailty Index and the Frailty Phenotype can help predict the likelihood of severe immune-related toxicities and guide therapy modifications. Interventions such as tailored nutritional plans and resistance training can significantly reduce frailty in older cancer patients, thereby enhancing treatment tolerance and improving clinical outcomes. Given the link between aging and metabolic dysfunction, existing data highlight the association between dietary factors and frailty and indicate that insufficient intake of protein, vitamins C, D, E and calcium is particularly associated with an increased risk of frailty.29 Conversely, overnutrition and obesity have also been shown to elevate the risk of frailty, reflecting the complex interplay between nutrition and health in older adults. Protein supplementation in frail older individuals can help mitigate frailty-related risks. Combining dietary improvements with resistance exercise has demonstrated potential in preserving or increasing muscle mass, effectively addressing the nutrition-frailty cycle and improving overall physical function.
Among other important factors to consider are socioeconomic disparities that significantly impact frailty and access to cancer care among older adults.30 Individuals from lower socioeconomic backgrounds often experience higher levels of frailty due to limited access to healthcare, inadequate nutrition and increased exposure to environmental stressors. These challenges can lead to delayed cancer diagnoses and reduced treatment options, exacerbating health outcomes. Structural inequities in health determinants and the accessibility and delivery of healthcare services must be addressed to reduce frailty and improve health outcomes in vulnerable populations, particularly in older adults.
Toxicity and AEs in frail patients
Frail individuals experience a disproportionate burden of immune-related toxicities, particularly irAEs, during ICI therapy. These toxicities, which range from mild dermatologic reactions to severe organ dysfunction, occur at higher rates in frail patients, often necessitating hospitalization or intensive supportive care. Frailty-associated impairments in immune regulation and metabolic function may further exacerbate irAE severity. Early treatment discontinuation or dose modifications due to irAEs are common in this population and may compromise the intended therapeutic benefits of ICIs, underscoring the importance of careful patient selection for ICI treatment. The toxicity profiles of different ICIs in older adults are generally comparable to those in younger patients. Anti-CTLA-4 therapy is associated with a higher incidence of AEs than anti-PD-(L)1 therapy, and combination therapy is associated with a higher incidence of AEs than monotherapy. CTLA-4 inhibitors more frequently cause colitis and dermatitis, whereas PD-1/PD-L1 inhibitors often cause pneumonia and thyroid dysfunction.
Quality of life and functional status
In the treatment of frail older adults, the preservation of QoL and functional independence often appears more in line with patient expectations compared with focusing on survival outcomes primarily. ICIs, while extending survival in many cases, are associated with treatment-related toxicities that can negatively impact QoL, particularly in frail patients with a limited adaptive capacity. This highlights the importance of patient-centered discussions that incorporate the individual’s values, preferences and overall treatment goals into therapeutic decision-making. Such discussions often require the involvement of informal caregivers or care facility staff, especially when patients face cognitive or physical limitations. Effective decision making relies on shared input, clear communication and careful consideration of caregiver capacity, supported by tools such as comprehensive geriatric assessments to align treatments with patient-specific goals. Timely end-of-life (EoL) discussions are essential to ensure that treatment decisions align with patient preferences and values, particularly in advanced stages of illness. Early integration of EoL discussions can prevent aggressive treatments in the last stages of life and align care with patient values.
Importantly, psychological factors such as depression, anxiety and emotional resilience play a significant role in determining therapeutic outcomes in older patients with cancer. These factors can influence treatment adherence, recovery and overall QoL, often compounding the challenges posed by physical frailty. Addressing psychological health through supportive care and mental health interventions is crucial for optimizing therapeutic outcomes and ensuring a holistic approach to cancer treatment in older adults.
Clinical implications and recommendations
For frail older patients, careful weighing of the risks and benefits during decision making is essential to ensure optimal patient outcomes. Incorporating levels of health literacy and engaging primary care physicians alongside oncologists and geriatricians can enhance the decision-making process. Comprehensive Geriatric Assessment (CGA)31 performed before initiating ICIs can help in evaluating frailty, comorbidities, functional status and cognitive health in order to identify patients who are most likely to benefit from ICI therapy and initiate assessment-driven non-oncological recommendations and interventions when needed.
GA is a critical tool for identifying vulnerabilities, such as physical, cognitive and nutritional deficiencies, in older patients. Findings from the American Society of Clinical Oncology (ASCO) guidelines32 emphasize the value of tools such as the Practical Geriatric Assessment (PGA), which can streamline assessments, ensuring that domains such as comorbidities, polypharmacy and social support are systematically addressed before initiating ICIs. The GAP70+ trial demonstrated that GA-guided interventions significantly reduced treatment-related toxicity,33 underscoring their relevance in geriatric oncology and suggesting that they should be integrated into the clinical care of older patients with advanced cancer and ageing-related conditions. The International Society of Geriatric Oncology (SIOG) recommends thorough GA to evaluate comorbidities, functional status and potential vulnerabilities in older patients,34–36 which would help identify individuals who are most likely to benefit from ICI therapy and tailor treatment plans accordingly. The position paper published by the Young SIOG reviews the use of ICIs in older adults with a focus on NSCLC patients.37 It provides recommendations to address data gaps in this population by incorporating functional measures of frailty and patient-reported outcomes, as well as including biological markers of immunosenescence in clinical trials to evaluate the impact of age-related immune changes on treatment efficacy and toxicity.
In summary, the use of ICIs in frail populations requires a multidisciplinary approach and close coordination among oncologists, geriatricians and allied healthcare professionals to manage treatment expectations, optimize supportive care and ensure optimal patient-centered outcomes.
Perspective
Since older and/or frail patients are underrepresented in registrational trials38 and no prospective evidence exists regarding the efficacy and safety of dose-reduced platinum-doublet chemotherapy in combination with anti-PD-(L)1 ICIs — regimens frequently used in older and frail patients in daily practice — an opportunity arises to participate in an innovative Swiss trial set to open soon. Planned to start in Q1/2025, this study titled “Dose-reduced platinum-doublet chemotherapy in combination with cemiplimab versus cemiplimab monotherapy in older and/or frail patients with metastatic NSCLC with PD-L1 <50%” is conducted by the Swiss Group for Clinical Cancer Research (Schweizer Arbeitsgemeinschaft für Klinische Krebsforschung, or SAKK) and led by Dr Laetitia Mauti from Cantonal Hospital Winterthur (KSW). In this trial, the G8 screening tool will help identify patients at risk of increased treatment toxicity and those who may benefit from CGA.
Conclusions
ICIs offer promising treatment options for older patients with cancer; however, frailty might significantly affect their efficacy and safety. Frail patients exhibit higher rates of AEs and may have less favorable outcomes, indicating a need for careful patient selection and tailored treatment approaches. Future research should focus on integrating frailty assessments into clinical trials and developing frailty-specific treatment strategies, interventions and guidelines, including tailored dosing regimens and enhanced toxicity management, to optimize the use of ICIs while minimizing risks in this vulnerable population. Expanding the evidence base through real-world studies focusing on frail populations can provide insights into optimizing dosing regimens, toxicity management and patient selection criteria.
Conflict of interest
Marcus Vetter received honoraria for consultancy from GSK, Roche, Novartis, ExactSciences, Pfizer, Stemline, AbbVie and ASC Oncology. Nina Neuendorff received honoraria and travel support by Janssen-Cilag, Medac, Novartis, Pfizer, Abbvie, Hexal and Jazz Pharmaceutical. These funding entities did not play any role in the development of the manuscript and did not influence its content in any way. Other authors have declared that the manuscript was written in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors have declared that no financial support was received from any organization for the submitted article.
Author contributions
All authors contributed to and approved the final manuscript.