
Introduction
Dysregulation of hemostasis-related pathways is common in patients with cancer and the risk of thromboembolic and bleeding complications in these patients are well documented and require a thorough benefit/risk assessment for those requiring anticoagulation.1,2 The global health burden due to venous thromboembolism (VTE), comprising pulmonary embolism and deep vein thrombosis, is substantial, with 10 million cases reported worldwide each year, including approximately one million in the European Union.3 Active cancer patients account for approximately 20% of all VTE cases,4 with 2- to 9-fold higher risk for VTE compared with individuals without cancer,5–7 particularly in the case of advanced metastatic malignancies.2 Several risk factors can affect the risk of VTE, including age, sex, comorbidities, tumor type and disease stage,8,9 and VTE itself can be a predictor of poor survival outcomes, possibly reflecting a more aggressive disease.10 In Switzerland, the mortality rates of patients with pulmonary embolism or deep vein thrombosis within 90 days following diagnosis are 6.1% and 2.7%, respectively.11 In contrast, the European multicenter RIETE study has reported much higher mortality rates up to 90 days following diagnosis: 14% in pulmonary embolism plus deep vein thrombosis, 11.0% in isolated pulmonary embolism and 6.3% in deep vein thrombosis, which may be due to differences in data collection, access to diagnostic assessment and therapy.
Combined thrombophilia and bleeding risk in cancer patients
Cancer patients are challenging, as an increased risk of thrombosis and bleeding narrows the therapeutic window for antithrombotic treatment. The process of hemostasis involves several interlinked steps: constriction of the blood vessel, formation of a temporary platelet plug, activation of the coagulation signaling cascade and formation of a fibrin plug (the final clot), resulting in the cessation of bleeding.12 While hemostasis is the physiological defense mechanism against bleeding, thrombosis represents a pathological excess of thrombus formation that obstructs blood flow. Virchow’s triad describes three elements that contribute to thrombosis: endothelial injury, vascular stasis, and hypercoagulability or thrombophilia. These factors are also involved in the pathophysiology of VTE in cancer patients. Changes in tumor biology, coagulation activation and inflammation further characterizes the pathogenesis of cancer-associated thrombosis.2 Most patients with active cancer exhibit chronic and systemic activation of coagulation, with a variety of pathophysiological changes that favor thrombosis, including platelet activation, direct coagulation factor activation, decreased hepatic natural anticoagulant synthesis, reduced hepatic clearance of coagulation factors, thrombotic microparticles and, in rare cases, the presence of antiphospholipid antibodies and thrombotic microangiopathy.13 Thromboinflammation plays an important role not only in VTE but also in the context of seeding the ground for metastatic disease.14–16
On the other hand, bleeding complications are also more common in patients with cancer compared with the general population.17–21 Approximately 10% of all patients with cancer experience at least one bleeding episode, and the incidence of bleeding increases to 30% in patients with hematologic malignancies.22 The causes of increased bleeding risk include local tumor invasion, angiogenesis and abnormal tumor vasculature, prior radiation therapy or chemotherapy, thrombocytopenia related to cancer or chemotherapy and the use of certain drugs, such as immunotherapeutic agents (bevacizumab), nonsteroidal anti-inflammatory drugs and anticoagulants. In a pooled analysis of data collected from patients treated with anticoagulants at multiple US healthcare organizations, cumulative bleeding incidence at six months after initiation of anticoagulation therapy was higher in cancer patients compared with those without cancer regardless of anticoagulant used (20.2% vs 12.6% with warfarin, 16.7% vs 12.1% with rivaroxaban, 13.2% vs 9.7% with low-molecular-weight heparins and 14.5% vs 9.3% with apixaban, respectively; p<0.001 for all comparisons).17 Among identified risk factors predisposing to bleeding were metastatic disease, advanced-stage chronic kidney disease, obesity and platelet counts <100 G/L. Patients with primary gastrointestinal malignancies, in particular, tumors of the luminal gastrointestinal tract, as well as genitourinary cancers, had a higher incidence of bleeding compared to patients with other cancer types.17,23
Coagulation cascade
To better understand the pitfalls in clinical management of anticoagulation in cancer patients, a thorough understanding of the coagulation cascade and the required tests is mandatory. Interpretation of these tests can be complicated by the fact that inflammatory conditions in cancer can interfere with standard coagulation assays and need to be recognized in order to draw correct conclusions. The current cellular model of the coagulation cascade includes the following stages: initiation, amplification, propagation and stabilization (Figure 1).24,25 During this process, platelets act as hemostasis-maintaining cells and are critical for injury-sensing, aggregation (adhering to collagen and each other) and thrombus formation.26,27 During cancer progression platelets also play an important role in propagating inflammation and neoangiogenesis, as well as metastasis.14,15 In cancer patients, coagulation cascade can be overactivated, leading to latent or even overt disseminated intravascular coagulopathy (DIC). Another cancer-related phenomenon can be thrombotic microangiopathy (TMA), which is characterized by thrombosis and mechanical hemolysis in capillaries and arterioles due to endothelial injury and can be life-threatening without immediate treatment of the propagating malignancy.

Antithrombotic agents
Antithrombotic agents are classified into two main types: antiplatelet agents and anticoagulants.28 Antiplatelet agents disrupt primary hemostasis by inactivating platelet-induced clot formation (aggregation), whereas anticoagulants act on the coagulation cascade and prevent fibrin polymerization (clot formation). Historically, commonly used anticoagulants included heparins (both unfractionated and low-molecular-weight heparin) and vitamin K antagonists (VKAs), such as phenprocoumon, acenocoumarol and coumadin (warfarin).29,30 The modern armamentarium includes direct oral anticoagulants (DOACs), acting on FXa (apixaban, rivaroxaban, edoxaban) or FIIa (dabigatran) (Table 1).31 The advantages of these novel agents are rapid onset of action, a relatively lower potential for drug interactions and lack of need for constant monitoring.32 Notably, the pharmacokinetic properties of each DOAC can be variably affected by the renal and liver function of the patient.33
The first DOAC to be approved was dabigatran, a direct thrombin inhibitor that reversibly binds to the active site on the thrombin molecule, preventing the thrombin-mediated activation of coagulation factors.34 It is approved for stroke prevention in atrial fibrillation (AF) and the treatment/prevention of deep vein thrombosis and pulmonary embolism. Similar to other DOACs, dabigatran offers rapid onset of action, predictable pharmacokinetics and fixed dosing.
Rivaroxaban, apixaban and edoxaban act as FXa inhibitors within the coagulation cascade.35 These agents are used for the prevention of stroke, as well as the treatment/prevention of deep vein thrombosis and pulmonary embolism, and are characterized by convenient administration, predictable pharmacokinetics and reduced risk of major bleeding. However, a major limitation is that some of these compounds lack specific reversal agents. Renal function and drug interactions should be considered when selecting appropriate antithrombotic treatment.
Coagulation assays
Global coagulation assays that evaluate deficiencies in coagulation factors include activated partial thromboplastin time (aPTT), prothrombin time (PT) and thrombin time (TT) (Table 2). While routine laboratory monitoring is not required in patients treated with DOACs, performing such assessments is relatively easy using specific calibrated assays in individual situations.37 It is important to note that DOACs, as well as inflammation in cancer, can interfere with the standard functional coagulation assays, aPTT and PT, limiting their utility in this context.38 For dabigatran, dilute TT and ecarin clotting time assays (anti-FIIa assay) have shown high sensitivity.37 In patients treated with rivaroxaban, the best correlation with plasma concentration has been observed with specific DOAC-calibrated anti-FXa assays. Similarly, for both apixaban and edoxaban, calibrated anti-FXa assays show the strongest correlation with plasma concentration. If specific calibrated assays are not available, an equivalent common anti-FXa assay might also be used to measure residual DOAC activity.39 The anti-platelet activity (light transmission platelet aggregation by Born for aspirin, clopidogrel and ticagrelor, whole blood platelet aggregation using Multiplate® for aspirin, clopidogrel and ticagrelor, point of care testing VerifyNow® for aspirin and ticagrelor)40 can only be assessed in specialized centers and are not routinely available, but may be useful to identify insufficient anti-platelet effect in patients with myeloproliferative disorders and high thromboembolic risk.41
Risk assessment for development of venous thromboembolism
Cancer patients are at a higher risk of developing venous and arterial thromboembolism, as outlined above. The National Institute for Health and Care Excellence (NICE) and European Society for Medical Oncology (ESMO) guidelines recommend the use of validated risk assessment models (RAMs) to assess the risk of VTE.42,43 Among many models developed, the Caprini RAM is one of the most commonly used tools. It weighs several different risk factors, providing an overall risk score based on the number of risk factors (Table 3).44 Based on the Caprini RAM, low-risk patients (score of 0–4) require no extended VTE prophylaxis, while those deemed at moderate risk (score of 5–8) or high risk (score of ≥9) received extended prophylaxis (for 10 and 30 days, respectively). Among high-risk patients with cancer, implementing this model led to a 58% decrease in VTE rates compared with the pre-intervention group (7 to 3% rate of VTE).44
Notably, while many RAMS have been developed to predict the risk of VTE, a recent systematic review found that the predictive accuracy of available RAMs in cancer patients, including the Caprini RAM, the Padua prediction score, IMPROVE models, the Geneva risk score and the Kucher score, is generally weak.45 However, even a small predictive benefit provided by these models may be of clinical value.
The CHADS2 score utilizes a point-based risk stratification scheme for the assessment of stroke risk. The European Society of Cardiology (ESC) guidelines recommend using the CHA2DS2-VASc score as a risk assessment tool for stroke; however, its use in cancer patients has not been validated as this population was excluded.46 This scoring system assesses the risk of stroke in patients with AF: two points are given for stroke, transient ischemic attack or age ≥75 years; one point is given for diabetes mellitus, vascular disease, age 65–75 years or female sex.47,48 Anticoagulant therapy is recommended if the CHA2DS2-VASc score is ≥2 in men or ≥3 in women and therapy should also be considered if the CHA2DS2-VASc score is ≥1 in men or ≥2 in women.49 It is important to note that while the CHA2DS2-VASc score was designed to identify patients at low risk of stroke in the general population, thereby indicating those for whom anticoagulation should be avoided and the evidence for its use in cancer patients remains scarce.
Efficacy of DOACs in cancer patients compared with the general population
A cohort study of 18,495 adults with recurrent VTE showed that DOACs performed better compared with warfarin in reducing the incidence of VTE, with an event rate per 100 person-years of 2.92 (95% CI: 2.29–3.54) versus 4.14 (95% CI: 3.90–4.38).50 In addition, DOACs versus warfarin were associated with a lower rate of hospitalizations for hemorrhage (event rate per 100 person-years: 1.02 [95% CI: 0.66–1.39] vs 1.81 [95% CI: 1.66–1.97]) and all-cause death (event rate per 100 person-years: 3.79 [95% CI: 3.09–4.49] vs 5.40 [95% CI: 5.13–5.66]). Several randomized controlled clinical trials have evaluated the efficacy and safety of DOACs in patients with cancer-associated VTE. While reporting lower VTE recurrence and non-inferiority compared with low-molecular-weight heparins, the studies produced inconsistent results in terms of bleeding risk with DOACs in patients with active cancer or a recent history of cancer. The Hokusai VTE Cancer20 and SELECT-D21 trials demonstrated higher rates of major bleeding and clinically relevant non-major bleeding with edoxaban and rivaroxaban, respectively, than with dalteparin. However, in the ADAM VTE51 and CARAVAGGIO52 trials, apixaban did not increase the risk of major bleeding events. A systematic review and meta-analysis of the data from 2607 patients enrolled in these studies53 showed that the use of DOACs was associated with a 32% lower risk of recurrent VTE (RR: 0.68 [95% CI: 0.39–1.17]; I2=0%) and a 36% higher risk of major bleeding (RR: 1.36 [95% CI: 0.55–3.35]; I2=15%) compared with dalteparin, although these effects did not reach statistical significance. Similarly, there was a non-significant trend towards a decrease in the risk of the composite outcome of recurrent VTE or major bleeding with DOACs versus dalteparin (RR: 0.86 [95% CI: 0.60–1.23]; I2=0%). These data support the use of DOACs as an acceptable therapeutic option for patients with cancer-associated VTE but suggest that these agents should be avoided in individuals at high risk of bleeding, especially patients with gastrointestinal or genitourinary cancers, and an individualized benefit/risk assessment is required considering general (age, comorbidities and comedications) as well as cancer-specific factors (cancer type and stage).54 A meta-analysis of studies comparing DOACs with aspirin in patients with multiple myeloma further showed that thrombophylaxis with DOACs was associated with significantly lower rates of VTE (odds ratio: 0.33 [95% CI: 0.16–0.68]; p<0.001).55
The data further showed favorable clinical outcomes with specific DOACs compared with traditional options. In the ROCKET AF trial, no difference was found in the risk of bleeding in patients receiving rivaroxaban versus warfarin (14.9% vs 14.5%; HR: 1.03 [95% CI: 0.96–1.11]; p=0.442).56 However, patients in the rivaroxaban arm experienced significantly fewer deaths from major bleeding (0.24% vs 0.48%; p=0.003) and intracranial bleeding (0.77% vs 1.18%; p<0.05).
Both apixaban and edoxaban have demonstrated remarkable efficacy in reducing the bleeding risk versus warfarin in patients with AF.57,58 In the ARISTOTLE trial, apixaban was more effective than warfarin in reducing stroke or systemic embolism with a consistent effect across age groups.57 Compared with warfarin, treatment with apixaban also led to improvements in the rates of major bleeding with a consistent treatment effect across age groups (interaction with continuous age, p=0.63), as well as reduced the rate of intracranial hemorrhage in patients aged 65–74 years (HR: 0.35 [95% CI: 0.20–0.60]) and among those aged ≥75 years (HR: 0.34 [95% CI: 0.20–0.57]). Furthermore, a meta-analysis of randomized controlled trials showed that patients receiving edoxaban versus warfarin experienced significant reductions in the incidence of cardiovascular death (relative risk [RR]: 0.86 [95% CI: 0.80–0.93]; I2: 0.0%), major bleeding (RR: 0.65 [95% CI: 0.59–0.71]; I2: 75.6%) and non-major bleeding (RR: 0.80 [95% CI: 0.77–0.84]; I2: 79.3%).58 Studies on AF usually excluded cancer patients, therefore, the risk-benefit has to be individualized, depending on the specific cancer-inherent bleeding risk, as outlined above.54
Bleeding risk assessment in cancer patients compared with the general population
The International Medical Prevention Registry on Venous Thromboembolism (IMPROVE) study aimed to assess the incidence rates of in-hospital bleeding and identify risk factors at admission associated with short-term in-hospital bleeding risk in acutely ill medical patients.59 The investigators identified 11 factors that were independently associated with major and clinically relevant non-major bleeding, including active gastroduodenal ulcer, prior bleeding, low platelet count, age, hepatic or renal failure, intensive care unit (ICU) stay, central venous catheter, rheumatic disease, cancer and male sex. Based on these criteria, the IMPROVE bleeding risk score (Table 4) classifies patients into high- (≥7 points) and low-risk (<7 points) categories. Several external validation studies confirmed good discriminatory power of the score to predict bleeding in acutely ill patients within 14 days after hospital admission.60–63 A note of caution has to be expressed, as the IMPROVE bleeding score does not account for cancer-specific bleeding and thrombosis risk.
The Hypertension, Abnormal renal/liver function, Stroke, Bleeding, Labile International Normalized Ratio (INR), Elderly, Drugs or alcohol use (HAS-BLED) score was developed to estimate the 1-year risk of major bleeding in patients treated with warfarin who were included in the Euro Heart Survey on AF.64 This score assigns one point for each of the following risk factors for major bleeding: uncontrolled hypertension (systolic blood pressure >160 mmHg), abnormal liver or renal function (including chronic dialysis, transplantation, or creatinine levels >2.26 mg/dL), prior stroke, bleeding history or predisposition, labile INR, age ≥65 years, concomitant use of aspirin or nonsteroidal anti-inflammatory drugs and excessive use of alcohol (Table 5). A score ≥3 indicates a high risk of bleeding. The HAS-BLED score has demonstrated strong predictive validity for major bleeding events, including intracranial hemorrhage, and superiority over other scoring systems.65–69 It is recommended for routine clinical use in patients with AF receiving anticoagulants but, again, was not validated for cancer patients.70,71
Although many tools have been developed for the evaluation of bleeding risk in the general population, data on their validation in cancer patients are limited. The post hoc analysis of the Hokusai VTE Cancer study which aimed to externally validate seven bleeding risk scores, including ACCP-VTE, HAS-BLED, Hokusai, Kuijer, Martinez, RIETE and VTE-BLEED, demonstrated poor to moderate predictive performance of these scores (C-statistics: 0.50–0.57) in a cohort of patients who received edoxaban or dalteparin for treatment of cancer-associated thrombosis.73 Pragmatic classification based on cancer type (gastrointestinal, genitourinary or other) showed marginally better estimates of clinically relevant bleeding risk. Improved results were achieved using a novel competing risk-adjusted prediction model, CAT-BLEED, based on clinical predictors for clinically relevant bleeding within six months after the diagnosis of cancer-associated thrombosis, with non-bleeding-related mortality as the competing event (C-statistics: 0.63 [95% CI: 0.58–0.68]). Similarly, poor to moderate predictive performance of the TE-BLEED, HAS-BLED, ORBIT and ATRIA models (C-statistics: 0.59–0.61) was observed in patients with a new cancer episode during anticoagulant therapy.74 Overall, these data indicate an unmet need for novel models that can better predict thrombosis and bleeding risk in cancer patients.
Dietary and drug-drug interactions with DOACs
When assessing the suitability of antithrombotic drugs in patients, it is also important to consider the presence of food and drug-drug interactions (DDIs), especially in patients treated with a broad range of anti-neoplastic treatments. Despite expecting fewer DDIs with DOACs relative to VKAs, there are still numerous considerations when deciding on the most adequate therapy and the available information continues to expand.
DOACs are associated with significant re-secretion via the P-glycoprotein (P-gp) transporter after absorption in the gut.75 The P-gp transporter also plays a role in renal clearance, and its involvement can lead to increased competition and subsequently increased DOAC plasma levels.75,76 This is particularly concerning patients with AF, as P-gp inhibitors, such as verapamil, dronedarone, amiodarone and quinidine, are used in their treatment. In terms of liver metabolism, dabigatran does not interact with CYP3A4 enzymes, whereas rivaroxaban and apixaban are moderately metabolized by these enzymes, with minimal edoxaban involvement (<4% elimination). Due to the DDIs with P-gp and CYP3A4 inhibitors, the use of DOACs with these agents is not recommended.77 Furthermore, various DDIs have been observed between DOACs and antivirals, anti-epileptics, antibiotics, antifungals and dexamethasone, even at low doses.75,78,79
Caution is also advised when DOACs are used concomitantly with certain targeted anticancer therapies because such combinations may lead to increased bleeding risks (Table 6). For example, a higher risk of bleeding has been observed in patients receiving Bruton’s tyrosine kinase inhibitors and vascular endothelial growth factor inhibitors.80
In terms of diet, many supplements are known to interact with DOACs, potentially affecting the risk of bleeding.75 One study reported the use of dietary supplements with potential interactions (e.g., herbal teas, turmeric, Chinese herbs/ginger/ginkgo biloba, and St John’s wort) in patients receiving apixaban.81 These supplements do not interact with DOACs in terms of direct drug-drug interactions, but are known to induce an anti-platelet effect, thus increasing the risk of bleeding due to combined platelet inhibition. Overall, 14.7% of patients took aspirin daily and the use of at least one other over-the-counter drug was reported in 17.2% of daily aspirin users. The use of acetaminophen as needed was common (51.1%). This study also noted a large knowledge gap among patients regarding the risks associated with the concomitant use of dietary supplements or other medications with anticoagulant therapy, highlighting the need for better patient education and routine inquiry for any use of contraindicated medications.
Perioperative risk assessment in patients receiving antithrombotics
An additional challenge for cancer patients is their frequent exposure to surgical interventions. Guidelines on the perioperative management of anticoagulants and antiplatelet agents83 provide general recommendations for a standardized approach to assess the risk of thromboembolism and perioperative bleeding, which may help guide the management of cancer patients. Again, bleeding and thrombosis can be a combined issue for cancer patients, requiring an individual risk/benefit assessment.
The Clinical Excellence Commission outlines several considerations when assessing the risk of arterial and venous thromboembolism, including types of mechanical heart valves, the CHADS2 score (which assesses stroke risk) and patients’ history of VTE.83 Thrombosis risk is estimated by the prescribing physician as low, moderate or high based on the patient’s condition and the presence of risk factors (Table 7). The CHADS2 score is used to estimate the annual risk of stroke in patients with non-valvular AF who are not taking an anticoagulant. It is recommended to use the CHADS2 score, rather than the CHA2DS2VASc score, based on a landmark study that assessed the risk of bleeding and thromboembolism in patients with AF receiving perioperative bridging anticoagulant therapy.84 These recommendations also rank various surgical procedures by the risk of bleeding into minimal-risk, low-risk (2-day risk of major bleeding <2%) and high-risk (2-day risk of major bleeding >2%) (Table 8). Minimal-risk surgeries include cataract procedures, implantation of a cardioverter-defibrillator or pacemaker and minor dermatological and dental procedures; low-risk procedures include shoulder/foot/hand surgery, arthroscopy and other certain types of surgical interventions; high-risk procedures include major orthopedic, cardiac and intra-abdominal surgery (e.g., bowel or visceral organ resection), surgeries in highly vascularized organs and certain urologic procedures, inter alia.
Perioperative management in patients receiving antithrombotics
Patients with cancer who are undergoing surgical resection are at significantly increased risk of peri- and post-operative VTE compared with patients with non-malignant diseases.85,86 Furthermore, AF rate is notably higher in cancer patients, with AF being one of the primary clinical indications for long-term anticoagulant therapy.87–89 For effective perioperative management, several key factors should be considered following point-of-care coagulation testing, bleeding risk, the effects of surgery on hemostasis, the administration of transfusions and coagulation factor concentrates.90,91
Prior to surgery and under the guidance of a specialist, anticoagulation therapy with VKAs, anti-Xa drugs or antithrombin agents should be discontinued; the time of discontinuation will vary depending on the antithrombotic agent used (Table 9).90,92 When possible, patients may be transitioned to a shorter-acting anticoagulant such as heparin or low-molecular-weight heparin. Non-aspirin antiplatelet agents, including thienopyridines such as clopidogrel, ticagrelor or prasugrel, should be discontinued promptly before surgery, while the use of aspirin can be assessed on a case-by-case basis.91 When adjusting anticoagulation therapy, it is important to balance the risk of thrombosis versus increased bleeding. Intraoperative bleeding may be reduced using blood management protocols, reversal of anticoagulants and antifibrinolytics for prophylaxis in cases of excessive blood loss and acute normovolemic hemodilution. During major postoperative bleeding, the patient’s status can quickly change from hemorrhagic to prothrombotic, as hypercoagulability can emerge as an acute-phase response to the provision of antithrombotics. If pharmacological VTE prophylaxis is contraindicated, mechanical methods of prophylaxis can be employed, including graduated compression stockings and intermittent pneumatic compression.43 If the risk of VTE is very high, a combination of mechanical and pharmacological prophylaxis may be considered.
In the case of urgent reversal of VKAs prothrombin complex concentrates (PCCs) can be administered, while vitamin K can be used for nonurgent reversal agent, unless rapid restoration of anticoagulation following surgery is needed.93 Antifibrinolytics such as tranexamic acid may be used as prophylaxis in patients with excessive blood loss.94 When coagulopathy is suspected, several approaches can be used to assess patient status, including standard coagulation tests like INR, aPTT and fibrinogen concentration, alongside viscoelastic assays, such as thromboelastography, rotational thromboelastometry and platelet count.90,91
The ESMO clinical practice guidelines recommend continuing with postoperative thromboprophylaxis for at least 10 days.43 However, as the mean time from major surgery to VTE occurrence is 17 days, with 30% of patients experiencing VTE beyond 21 days post-surgery, the extension of postoperative prophylaxis beyond 10 days may be appropriate in selected patients, including those undergoing major orthopedic surgery, open abdominal or pelvic surgery or laparoscopic colorectal cancer surgery.
Data from the SWIss Venous ThromboEmbolism Registry (SWIVTER) showed that 40% of patients with cancer who were at high risk of VTE did not receive any form of prophylaxis prior to the onset of acute VTE, highlighting an unmet clinical need for these patients.95 The inadequate pharmacological thromboprophylaxis may be explained by the increased risk of bleeding among these patients, the presence of chemotherapy-induced thrombocytopenia, concerns of reduced quality of life due to daily injections or an issue of cost-benefit. However, if the primary concern is an increased risk of bleeding, mechanical thromboprophylaxis should be considered in such patients. The lack of prophylaxis reported among high-risk cancer patients is supported by similar results from the RIETE and IMPROVE registries.95–97
Emergency management of bleeding
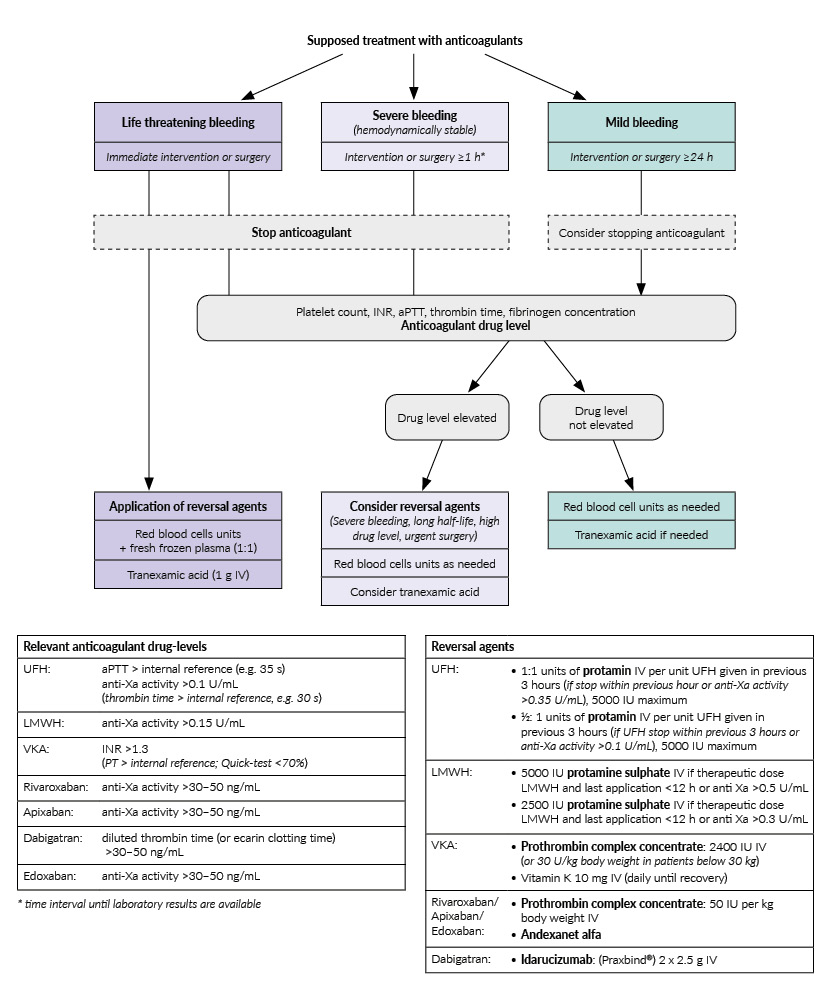
Cancer patients are prone to bleeding complications. In emergency scenarios, where the last dose of the anticoagulant is unknown, the initial step should include discontinuing the anticoagulant, particularly in the case of an extreme bleeding event, and assessing the anticoagulant blood level. In the case of DOACs, their concentration can be prolonged in patients with renal failure, which can be common in emergency admissions.98 When severe bleeding occurs, reversal agents may be considered; if the bleeding is life-threatening, reversal agents should be used immediately (Figure 2).36,98
More specifically, idarucizumab is approved as a reversal agent for dabigatran.99 Andexanet alfa is the approved reversal agent for FXa inhibitors, apixaban and rivaroxaban; however, while it is also effective for edoxaban, it is not yet approved.100,101 Non-specific reversal agents that may be effective following DOAC administration include PCCs, activated PCC (aPCC) and recombinant human FVIIa101; other pro-coagulants like antifibrinolytics, including tranexamic acid and aminocaproic acid, or desmopressin may be considered in cases of associated coagulopathy or thrombopathy.75 Fresh frozen plasma may be beneficial for plasma volume expansion in large transfusions but does not reverse anticoagulation.101 For patients on VKAs, vitamin K and PCCs may be used for reversal, while protamine is a suitable agent for those receiving heparins.102

Conclusions
-
Cancer patients are highly heterogeneous with an increased combined risk of thrombosis as well as bleeding.
-
DOACs rivaroxaban, apixaban, edoxaban and dabigatran have been shown to be efficient and safe in cancer patients considering some precautions. Low-molecular weight heparins still remain a valid option.
-
Specific calibrated anti-FIIa/anti-FXa assays are recommended for the assessment of residual DOAC activity.
-
DOACs have several advantages over older antithrombotics, such as a rapid onset of action, lack of routine laboratory monitoring and fewer DDIs.
-
Although DOACs have fewer DDIs than older anticoagulants, it is still crucial to educate patients on the common contraindicated foods and medications that they may encounter.
-
Many tools are available to assess the risk of thrombosis and bleeding and may help in individualized treatment decisions; however, validation in cancer patients is usually lacking.
-
In case of emergencies, management flow-chars should be used with consideration of specific reversal agents idarucizumab (dabigatran) and andexanet alfa (rivaroxaban/apixaban).
Acknowledgements
We are grateful to Prof. Dr Dr Michael Nagler (University Institute for Clinical Chemistry, Inselspital, University Hospital Bern, Bern, Switzerland) for his valuable comments. We would also like to thank the editorial office of healthbook TIMES Oncology Hematology for their assistance in preparing the manuscript for publication.
Conflict of interest
J-D. S received lecture and advisory honoraria from Bayer, BMS Pfizer, CSL Behring, Sanofi, Siemens Diagnostics and Takeda. Other authors have declared that the study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors have declared that no financial support was received from any organization for the submitted work.
Author contributions
The authors have created and approved the final manuscript.