Epidemiology of melanoma
Over the last few decades, the global incidence and mortality of melanoma cases have steadily increased, and it is now the fifth most common cancer in both males and females in Europe and the United States.1,2 In Europe, the annual incidence of melanoma varies between 3−5 cases/100,000 people in Mediterranean countries and 12–35 cases/100,000 people in Nordic countries, with projections showing that the overall rate in the European Union is expected to increase by 29% by 2040.3 To highlight the impact on Switzerland, it has both the highest rate of melanoma with an age-standardized rate of 27 cases per year/100,000 people4,5 and the most expensive direct melanoma-related healthcare costs per capita (7,300 euros) among selected European countries.6 Cutaneous melanoma constitutes the fourth most prevalent malignancy among males and females in Switzerland, accounting for approximately 6% of cancer cases.7 The predicted prevalence for 2025 is anticipated to be 65% higher in comparison to the available data from 2010.8 While the increases in melanoma cases are predicted to taper off in the near future,9 improving the treatment of this disease remains of great importance.
Current treatment options for melanoma
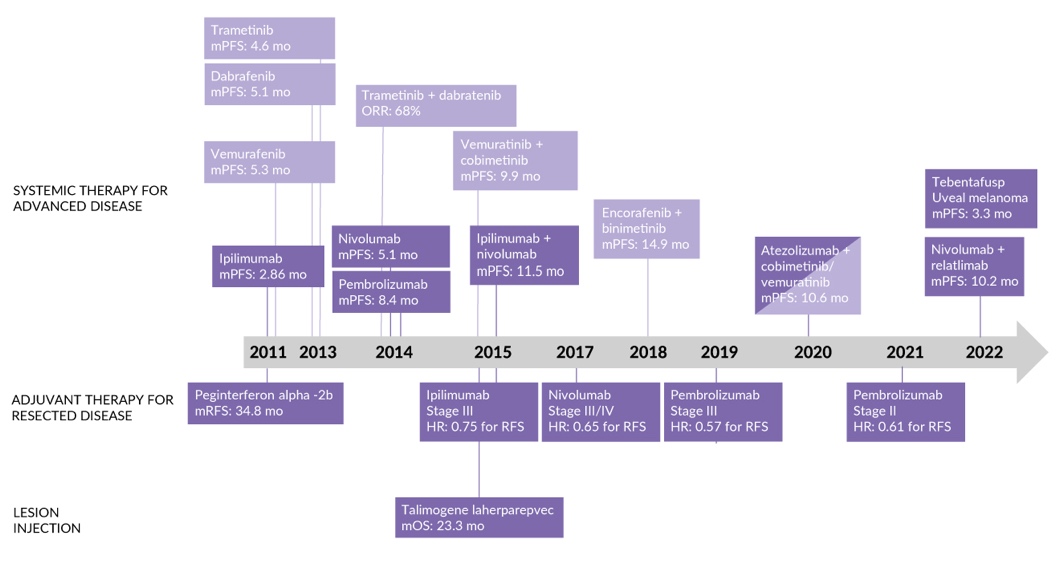
In the case of a primary tumor, surgical excision is recommended. In ulcerated tumors or those with a thickness ≥0.8 mm, a sentinel lymph node biopsy is recommended.4,10 In the case of completely resected advanced melanoma with macroscopic metastases, adjuvant systemic therapy should be offered.11 The recent expansion of the therapeutic armamentarium for advanced melanoma (Figure 1) has led to an increase in survival rates. These therapeutic approaches include immune checkpoint inhibitors (ICIs) and targeted therapies. ICIs include the anti-programmed cell death protein 1 (PD-1) or programmed death-ligand 1 (PD-L1) antibodies pembrolizumab, nivolumab and atezolizumab; anti-cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) antibody ipilimumab and anti-lymphocyte-activation gene 3 (LAG-3) antibody relatlimab. Tebentafusp, a T-cell receptor–bispecific fusion protein that targets glycoprotein 100 and CD3, prolonged overall survival (OS) in patients with metastatic uveal melanoma.12 Furthermore, oncolytic viruses offer a novel therapeutic strategy to selectively eliminate tumor cells and istimulate antitumor immune responses. Talimogene laherparepvec (T-VEC), a genetically modified herpes simplex virus (HSV), has demonstrated encouraging therapeutic activity in advanced melanoma, both as a monotherapy or in combination with other immunotherapeutic agents.13,14 Targeted therapy with BRAF/MEKi combinations includes encorafenib plus binimetinib, dabrafenib plus trametinib and vemurafenib plus cobimetinib. More recently, the FDA granted accelerated approval for adoptive cell therapy using tumor-infiltrating lymphocytes (TILs).15 With so many available options, optimization of treatment sequence has become more important. In Switzerland, physicians generally follow the current guidelines,11 with more patients receiving immunotherapy rather than targeted therapy in the first-line setting (70.7% vs 29.3%).16,17
The majority of cutaneous melanomas carry a driver mutation in the MAPK pathway, with the most commonly affected gene being BRAF.18,19 Activating mutations in BRAF lead to consecutive signaling that promotes the development of melanoma. BRAF inhibitor vemurafenib as monotherapy provided good, albeit transient, responses in patients with rapid development of resistance. In the phase III BRIM-3 trial, treatment with vemurafenib resulted in a 74%-reduction in the risk of death or disease progression versus dacarbazine (HR: 0.26 [95% CI: 0.20−0.33]; p<0.001).20 The confirmed objective response rate was 48% (including two patients with complete response [CR] out of 219) in the vemurafenib arm and 5% in the dacarbazine arm (p<0.001). MEK inhibitor trametinib, which targets another protein in the MAPK pathway, showed similar results with good, but short-lived responses. In the phase III METRIC trial, trametinib monotherapy yielded a median progression-free survival (PFS) of 4.8 months compared with 1.5 months with chemotherapy (HR: 0.45 [95% CI: 0.33−0.63]; p<0.001), with 6-month OS rates of 81% versus 67%.21 The response rate was 22% with trametinib and 8% with chemotherapy. Finally, combination therapy with BRAF/MEKi was associated not only with improved responses but also tolerability. However, similarly to single agents, resistance eventually develops with the median PFS ranging from 9.9 months with vemurafenib plus cobimetinib22 to 14.9 months with encorafenib plus binimetinib.23
_approvals_for_therapies_in_advanced_mel.jpeg)
Highlighting the benefit of recent therapeutic advances, a study using the Dutch Melanoma Treatment Registry (n=6,324) reported considerably prolonged OS in patients treated between 2013 and 2019, with median OS gradually increasing from 11.3 months for patients diagnosed in 2013 to 33.3 months for patients those diagnosed in 2019.25,26 Even better improvements in survival outcomes have been reported in individual studies.26 However, unmet needs among patients with advanced melanoma remain; these include combating drug resistance, as well as reducing high levels of adverse events (AEs) associated with some therapies.27 Many melanoma trials continue to provide updates on long-term follow-up or prospectively evaluate new therapy combinations to tackle ongoing unmet needs. The next section provides recent updates on selected clinical trials that investigate novel treatment options for patients with advanced melanoma (summarized in Table 1).
Immunotherapy approaches
Unresectable, metastatic melanoma
KEYNOTE-006 (NCT01866319)
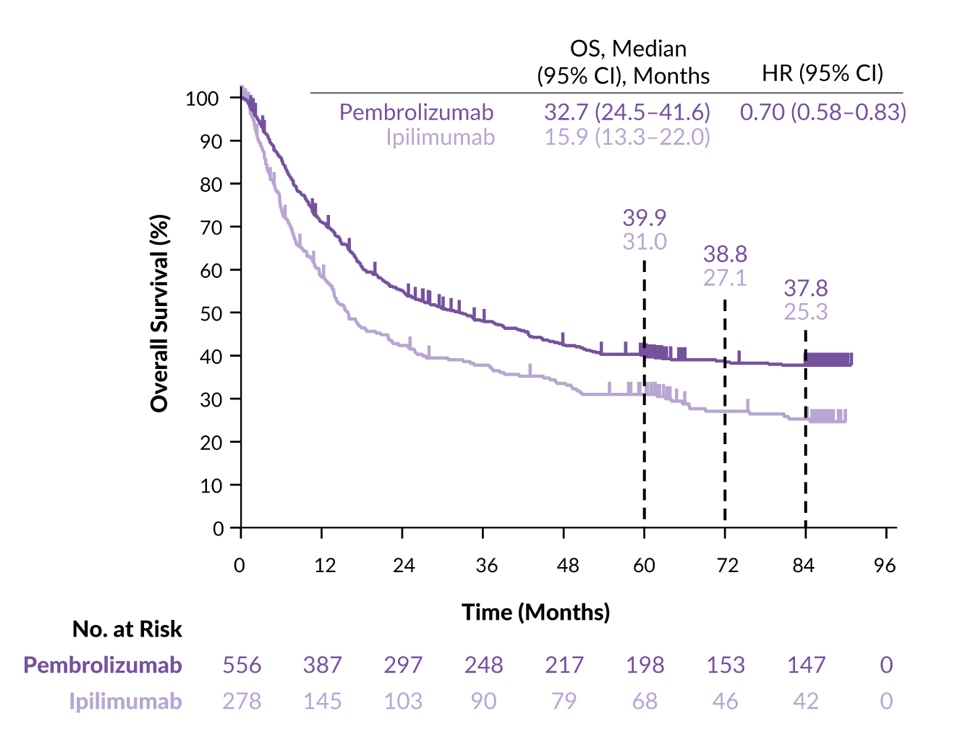
In this open-label, phase III trial, 834 patients with advanced melanoma who were treated with up to one prior systemic therapy were randomized 1:1:1 to receive the PD-1 inhibitor pembrolizumab every two weeks, pembrolizumab every three weeks or the CTLA-4 inhibitor ipilimumab (standard of care [SoC] at that time).30 The primary endpoints were PFS and OS. After a median follow-up of 57.7 months, PFS was significantly prolonged in the pembrolizumab groups (combined) versus ipilimumab (8.4 months vs 3.4 months; HR: 0.57 [95% CI: 0.48–0.67]; p<0.0001).29 Grade 3–4 treatment-related AEs (TRAEs) occurred in 17% of patients receiving pembrolizumab versus 20% receiving ipilimumab, including colitis (2% vs 6%), diarrhea (2% vs 3%) and fatigue (<1% vs 1%).
Seven-year follow-up analysis supported the previous reports, with a longer OS with pembrolizumab compared with ipilimumab (median, 32.7 months vs 15.9 months; HR: 0.70 [95% CI: 0.58–0.83]) and 7-year OS rates of 37.8% versus 25.3%, respectively (Figure 2).28 Pembrolizumab provided OS benefits regardless of BRAF mutational status, prior BRAF/MEKi treatment or select prognostic characteristics such as elevated lactate dehydrogenase (LDH), large tumor size and brain metastasis. The 7-year modified PFS rate was 23.8% versus 13.3%, respectively. In patients who completed ≥94 weeks of pembrolizumab treatment, the 5-year OS and modified PFS rates were 92.9% and 70.1%, respectively. These 7-year data support the long-term survival benefit of pembrolizumab versus ipilimumab in patients with advanced melanoma. Pembrolizumab58 and ipilimumab59 are approved by Swissmedic for the treatment of metastatic or unresectable melanoma.
_in_the_keynote-006_study.jpeg)
CheckMate 067 (NCT01844505)
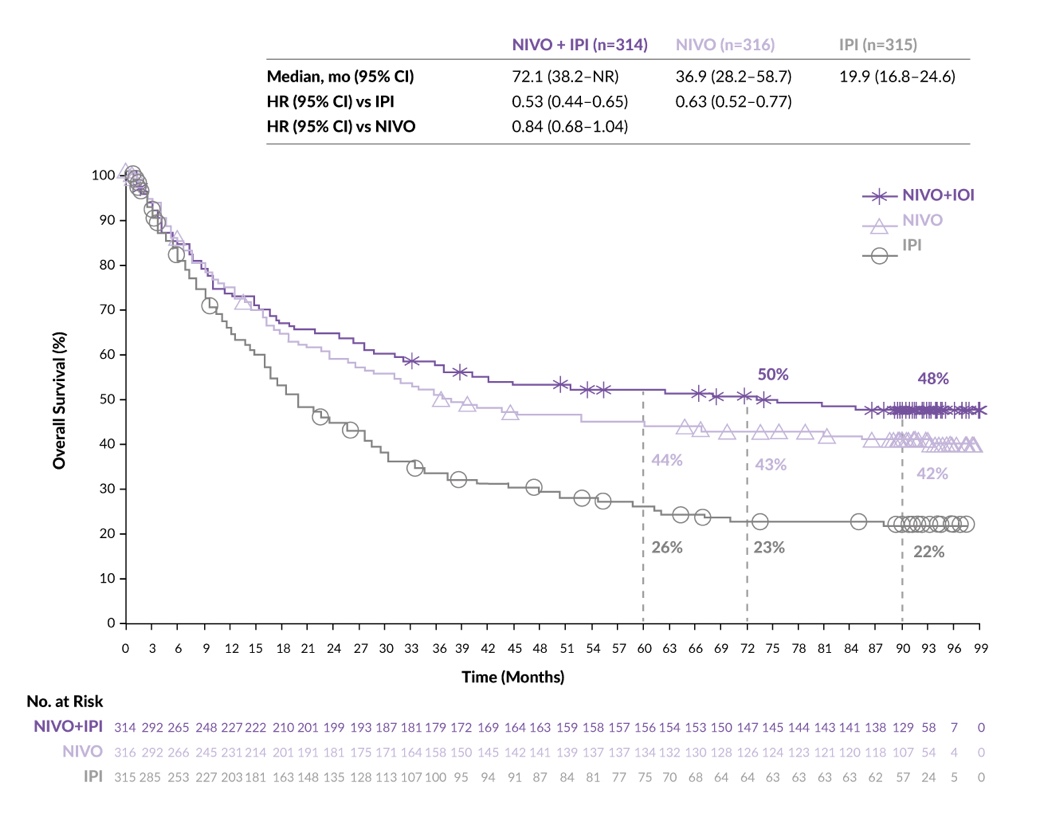
The PD-1 inhibitor nivolumab is approved in Switzerland for the treatment of unresectable or metastatic melanoma both as a monotherapy and in combination with ipilimumab.60 In this randomized, double-blind, phase III trial, 945 patients with previously untreated unresectable stage III or stage IV melanoma were randomized 1:1:1 to receive either nivolumab plus ipilimumab, nivolumab alone or ipilimumab alone.22 Coprimary endpoints were PFS and OS. The study was only powered to compare both nivolumab-containing arms with ipilimumab monotherapy. Nivolumab plus ipilimumab demonstrated durable clinical benefits at a minimum follow-up of 6.5 years, with a median OS of 72.1 months and a 6.5-year OS rate of 49%. The median melanoma-specific survival (MSS) was not reached (NR) and the MSS rate was 56%.26
At a minimum follow-up of 7.5 years, the median OS remained stable at 72.1 months with nivolumab plus ipilimumab versus 36.9 months with nivolumab versus 19.9 months with ipilimumab (Figure 3).36 The 7.5-year OS rates were 48% and 42% versus 22%. The median MSS was NR with nivolumab plus ipilimumab and 49.4 months with nivolumab alone versus 21.9 months with ipilimumab alone; the objective response rate (ORR) was 58% versus 45% versus 19%, respectively. The median duration of response (DoR) was NR versus 90.8 months versus 19.2 months in the nivolumab plus ipilimumab, nivolumab alone and ipilimumab alone arms, respectively. No new safety signals were observed since the previous analyses, which reported grade 3–4 TRAE rates of 59% and 24% versus 28% with nivolumab plus ipilimumab and nivolumab alone versus ipilimumab alone, with diarrhea being the most frequent grade 3–4 TRAE in the combination arm (10% and 3% vs 6%).26 In conclusion, an extended 7.5-year follow-up confirms the superiority of nivolumab-containing regimens over ipilimumab.
_in_the_checkmate_067_study.jpeg)
CheckMate 069 (NCT01927419)
This double-blind, phase II study randomized 142 patients with treatment-naïve unresectable stage III or IV melanoma in a 2:1 ratio to receive ipilimumab plus nivolumab (combination) or ipilimumab plus placebo (ipilimumab monotherapy).42 The primary endpoint was ORR in patients with BRAFV600 wild-type tumors. Patients who received a combination of ipilimumab and nivolumab exhibited a higher ORR compared with those who received ipilimumab monotherapy (61% vs 11%; p<0.001). The median PFS was NR versus 4.4 months, respectively (HR: 0.40 [95% CI: 0.23–0.68]; p<0.001). At a median follow-up of 24.5 months, the 2-year OS rates were 63.8% in the combination arm and 53.6% in the ipilimumab alone arm, with the median OS being NR in either arm (HR: 0.74 [95% CI: 0.43–1.26]; p=0.26).40 No difference in the 2-year OS rates was observed between BRAF-mutated and BRAF wild-type tumors. Grade 3−4 TRAEs were reported in 54% of patients who received nivolumab plus ipilimumab versus 20% of those who received ipilimumab alone. The most common 3−4 TRAEs included colitis (13%) and increased alanine aminotransferase (11%) in the combination arm compared with diarrhea (11%) and hypophysitis (4%) in the ipilimumab alone arm.
A recent single-cell RNA-sequencing (scRNAseq) analysis performed on a subset of samples from CheckMate-069 patients (n=52) further revealed a decrease in the ‘suppressive’ phenotype of regulatory T cells (Tregs) in responders, as indicated by the selective downregulation of EZH2 and FOXP3 expression.41 A higher CD8-central-memory cell proportion at C3D1 and lower Treg cell proportion at baseline were found to predict the response to ipilimumab plus nivolumab or ipilimumab alone, respectively. Furthermore, the response to anti-CTLA4 therapy could be predicted using the CD8+ T effector memory/Treg ratio.
RELATIVITY-047 (NCT03470922)
The dual checkpoint inhibitor combination of nivolumab and the LAG-3 inhibitor relatlimab was investigated in the global, double-blind, randomized, phase II/III RELATIVITY-047 study.44 A total of 714 patients with treatment-naïve metastatic or unresectable melanoma received nivolumab plus relatlimab (n=355) or nivolumab alone (n=359). The primary endpoint was PFS. At the initial data cut-off with a median follow-up of 13.2 months, patients in the nivolumab plus relatlimab arm experienced a significantly longer median PFS compared with those in the nivolumab alone arm (10.1 months vs 4.6 months; HR: 0.75 [95% CI: 0.62–0.92]; p=0.006).
Adjuvant therapy for resected melanoma
KEYNOTE-716 (NCT03553836)
This double-blinded, randomized, phase III study investigated adjuvant pembrolizumab versus placebo in patients with resected, high-risk, stage IIB-C melanoma.33 In total, 976 patients were randomized 1:1 to receive pembrolizumab or placebo. The primary endpoint was recurrence-free survival (RFS). With a median follow-up of 39.4 months, treatment with adjuvant pembrolizumab was superior to placebo at improving median RFS (NR vs NR; HR: 0.62 [95% CI: 0.49–0.79]) and distant metastasis-free survival (DMFS) (NR vs NR; HR: 0.59 [95% CI: 0.44–0.79]).32 The 36-month RFS and DMFS rates were both higher with pembrolizumab than with placebo (76.2% vs 63.4% and 84.4% vs 74.7%). The results were similar regardless of the cancer stage at baseline (stage IIB vs IIC). No new safety signals were observed. The most common grade ≥3 AEs were hypertension (3% vs 4%), diarrhea (2% vs <1%), rash (1% vs <1%), autoimmune hepatitis (1% vs <1%) and increased lipase (1% vs 2%) with pembrolizumab and placebo, respectively.31
KEYNOTE-054 (NCT02362594)
Patients with completely resected stage III melanoma were randomized to receive either pembrolizumab (n=514) or placebo (n=505) in this double-blind, phase III study.34 The primary endpoints were RFS in the intention-to-treat (ITT) population and patients with PD-L1-positive tumors (n=853).34 At a median follow-up of 15 months, treatment with pembrolizumab led to improvements in the 1-year RFS rate over placebo in the ITT population (75.4% vs 61.0%; HR: 0.57 [98.4% CI: 0.43–0.74]; p<0.001) and the PD-L1-positive subgroup (77.1% vs 62.6%; HR: 0.54 [95% CI: 0.42–0.69]; p<0.001). The rates of grade 3–5 TRAE were 14.7% in the pembrolizumab group and 3.4% in the placebo group.
Five-year follow-up data continue to support the use of pembrolizumab compared with placebo in this patient population, demonstrating improved 5-year RFS rates (55.4% vs 38.3%; HR: 0.61 [95% CI: 0.51–0.72]) and 5-year distant MFS rates (60.6% vs 44.5%; HR: 0.62 [95% CI: 0.52–0.75]).35 Similar results were reported in the PD-L1-positive subgroup.
CheckMate 238 (NCT02388906)
In this randomized, double-blind, phase III trial, 906 patients with resected stage IIIB, IIIC or IV melanoma were randomized at a 1:1 ratio to receive adjuvant nivolumab or ipilimumab.39 The primary endpoint was RFS and the key secondary endpoint was OS. At 4-year follow-up, treatment with nivolumab was more effective than ipilimumab at delaying recurrence (4-year RFS, 51.7% vs 41.2%; HR: 0.71 [95% CI: 0.60–0.86]; p=0.0003), but showed similar 4-year OS rates (77.9% vs 76.6%; HR: 0.87 [95% CI: 0.66–1.14]; p=0.31).37
A recently published updated 5-year efficacy results demonstrated that the median RFS remained superior with nivolumab compared with ipilimumab (HR: 0.72 [95% CI: 0.60–0.86]), with 5-year rates of 50% versus 39%.38 Five-year DMFS were also slightly improved with nivolumab versus ipilimumab (58% vs 51%; HR: 0.79 [95% CI: 0.63–0.99]). OS did not significantly differ between the arms (HR: 0.86 [95% CI: 0.66–1.12]) with the median OS NR in either arm and 5-year OS rates of 76% with nivolumab versus 72% with ipilimumab (75% data maturity). Biomarker analysis demonstrated that, across all treatment arms, factors associated with improved RFS and OS included higher tumor mutational burden, tumor PD-L1 expression, intratumoral CD8+ T cells, IFNγ-associated gene expression signature and lower levels of peripheral serum C-reactive protein; however, these factors had a limited clinically meaningful predictive value. In summary, the study confirmed sustained, long-term improvement in RFS and DMFS, as well as high OS rates with adjuvant nivolumab in patients with resected melanoma at a high risk of recurrence.
With a median follow-up of 19.3 months, the PFS benefit with nivolumab plus relatlimab compared with nivolumab alone remained similar to previously reported data (median PFS, 10.2 months vs 4.6 months; HR: 0.78 [95% CI: 0.64–0.94]).43 Median OS was NR with nivolumab plus relatlimab versus 34.1 months with nivolumab alone, however this difference did not reach statistical significance (HR: 0.80 [95% CI: 0.64–1.01]; p=0.059 [prespecified value for statistical significance, p≤0.043]). A greater number of patients in the combination arm achieved an objective response (ORR, 43% vs 33% with nivolumab alone). The safety profile of the combination treatment was consistent with the initial data, with patients experiencing a higher incidence of grade 3–4 TRAEs compared with the monotherapy arm (21% vs 11%). Patients in the combination arm were at a higher risk of treatment-related discontinuations of any grade (15% vs 7%) and treatment-related deaths of any grade (1% vs <1%). In summary, inhibition of two immune checkpoints, LAG-3 and PD-1, provided a greater PFS benefit than inhibition of PD-1 alone in this patient population. The combination is approved in Switzerland for the treatment of treatment-naïve unresectable or metastatic melanoma with PD-L1 expression <1%.61
Immunotherapy in the neoadjuvant setting
While the SoC for high-risk stage III melanoma is surgery followed by systemic therapy, the success of immunotherapy in the adjuvant and unresectable/metastatic settings has prompted its use as neoadjuvant therapy as well.
SWOG 1801 (NCT03698019)
In this phase II trial, patients with resectable stage IIIB–IVC melanoma were randomized to receive three doses of neoadjuvant pembrolizumab followed by surgery and adjuvant pembrolizumab (the neoadjuvant–adjuvant arm, n=154) or to surgery and adjuvant pembrolizumab (the adjuvant-only arm, n=159) for approximately one year or until progressive disease (PD) or unacceptable toxicity.62 The primary endpoint was event-free survival (EFS). At a median follow-up of 14.7 months, patients in the neoadjuvant–adjuvant arm had significantly longer EFS compared with the adjuvant-only arm (total number of events, 38 vs 67; p=0.004). At two years, EFS rates were 72% versus 49%, respectively. The rates of grade ≥3 TRAEs were 12% versus 14% in the neoadjuvant–adjuvant versus adjuvant-only arm, with no new safety signals identified.
NADINA (NCT04949113)
In this investigator-initiated, international phase III trial, 423 patients with resectable stage III melanoma who had not been previously treated with ICIs or BRAF/MEKi were randomized to receive two cycles of neoadjuvant ipilimumab plus nivolumab followed by therapeutic lymph node dissection (n=212) or to surgery followed by 12 cycles of adjuvant nivolumab (n=211).63 In the neoadjuvant arm, only patients who did not achieve a major pathologic response received adjuvant treatment. The primary end point was EFS.
At a median follow-up of 9.9 months, the estimated 12-month EFS rates were 83.7% in the neoadjuvant arm versus 57.2% in the adjuvant arm, with the difference in restricted mean survival time of 8.0 months (HR for progression, recurrence or death: 0.32 [99.9% CI: 0.15–0.66]; p<0.001).63 The benefits of neoadjuvant therapy were evident independently of the BRAF mutation status. In the neoadjuvant arm, the estimated 12-month RFS was 95.1% in patients with a major pathological response, 76.1% among those with a partial response (PR) and 57.0% among non-responders. Grade ≥3 AEs related to systemic treatment were reported in 29.7% of patients in the neoadjuvant arm and in 14.7% of patients in the adjuvant arm. These data demonstrate that the neoadjuvant immunotherapy followed by surgery and response-driven adjuvant therapy achieves better outcomes than the current SoC (adjuvant immunotherapy alone). The study is ongoing, with the data for OS, DMFS and quality of life are awaited.
BRAF/MEK inhibitors
Unresectable, metastatic melanoma
COLUMBUS (NCT01909453)
In this phase III study, 577 patients with locally advanced, unresectable or metastatic BRAFV600-mutated melanoma who were treatment-naïve or had received one line of immunotherapy and no prior BRAF/MEKi were randomized 1:1:1 to receive the BRAF/MEKi combination therapy with encorafenib plus binimetinib, a monotherapy with selective BRAFV600E mutation inhibitor vemurafenib or encorafenib monotherapy.45 The primary endpoint of PFS for encorafenib plus binimetinib versus vemurafenib was reported at 16.6 months follow-up (median PFS, 14.9 months vs 7.3 months; HR: 0.54 [95% CI: 0.41–0.71]; p<0.0001). A 5-year follow-up continued to support the efficacy and consistent safety profile of encorafenib plus binimetinib versus vemurafenib (PFS rate, 23% vs 10%; OS rate, 35% vs 21%; median DoR, 18.6 months vs 12.3 months; disease control rate [DCR], 92% vs 81%).23
At the 7-year follow-up, patients who received encorafenib plus binimetinib continued to achieve benefits compared with those who received vemurafenib monotherapy (PFS rate, 21.2% vs 6.4%; OS rate, 27.4% vs 18.2%).46 Over 30% of patients in the combination arm experienced treatment-emergent AEs (TEAEs) such as nausea, diarrhea, vomiting, arthralgia and fatigue. The most common grade 3–4 TEAEs were increased levels of γ-glutamyl transferase, blood creatine phosphokinase and alanine transaminase, as well as hypertension and anemia. The rates of discontinuation due to AEs remained similar across the arms (16–20%). These results confirm the long-term, sustained efficacy of encorafenib plus binimetinib, with no new safety signals identified. The combination is approved in Switzerland for the treatment of metastatic or unresectable BRAFV600-mutated melanoma.64,65
Neoadjuvant treatment of resectable melanoma
NCT02231775
In this phase II study, patients with stage III or oligometastatic stage IV BRAFV600E or BRAFV600K-mutated melanoma and no previous exposure to BRAF/MEKi were randomized 1:2 to receive upfront surgery and consideration for adjuvant therapy (SoC arm, n=7) or neoadjuvant plus adjuvant dabrafenib and trametinib (n=14).66 The primary endpoint was EFS. At a median follow-up of 18.6 months, significantly more patients in the neoadjuvant plus adjuvant arm were alive and progression-free compared with the SoC arm (ten [71%] patients vs 0). The median EFS was 19.7 months with neoadjuvant therapy versus 2.9 months with SoC (HR: 0.016 [95% CI: 0.00012–0.14]; p<0.0001). Neoadjuvant plus adjuvant dabrafenib and trametinib were well tolerated, with no reported grade 4 AEs or treatment-related deaths and most common grade 3 AE being diarrhea.
BRAF/MEK and ICI combination regimens
Unresectable melanoma
IMspire150 (NCT02908672)
In this phase III clinical trial, 514 patients with newly diagnosed unresectable BRAFV600-mutated advanced melanoma received combination therapy with either the PD-L1 inhibitor atezolizumab plus BRAF/MEKis vemurafenib and cobimetinib (n=256) or placebo plus vemurafenib and cobimetinib (control) (n=258).48 The primary endpoint was PFS. In the primary analysis, treatment with the atezolizumab-containing regimen achieved significantly longer PFS compared with the placebo-containing regimen (median, 15.1 months vs 10.6 months; HR: 0.78 [95% CI: 0.63−0.97]; p=0.025).
In the second interim analysis, the median follow-up was 29.1 months versus 22.8 months in the atezolizumab arm versus the control arm.47 The median OS was 39.0 months versus 25.8 months among patients receiving atezolizumab versus control (HR: 0.84 [95% CI: 0.66–1.06]; p=0.14). The rates of the most common grade 3–4 AEs were similar between the atezolizumab and control arms, including increased levels of lipase (23% vs 22%), blood creatine phosphokinase (22% vs 18%) and alanine aminotransferase (14% vs 9%). While the final analysis of OS is still pending, these interim OS data do not show a significant benefit of adding atezolizumab to vemurafenib and cobimetinib in patients with BRAFV600-mutated advanced melanoma. The combination of atezolizumab plus vemurafenib and cobimetinib is approved in Switzerland for the treatment of metastatic or unresectable BRAFV600-mutated melanoma.67
Combination therapy in the neoadjuvant setting
NeoACTIVATE (NCT03554083)
The combination of immunotherapy and targeted therapy prior to surgery was evaluated in the phase II trial that enrolled patients with stage III melanoma.68 Patients received either neoadjuvant vemurafenib, cobimetinib and atezolizumab (BRAF-mutated tumors, n=15) or cobimetinib and atezolizumab (BRAF-wild-type tumors, n=15) followed by therapeutic lymph node dissection and adjuvant atezolizumab. Pathologic response (≤50% viable tumor) and major pathologic response (≤10% viable tumor) were achieved in 86.7% and 66.7% of patients with BRAF-mutated tumors and 53.3% and 33.3% of patients with BRAF-wild-type tumors, respectively. Grade ≥3 AEs (mostly dermatologic) were reported in 63% of patients during neoadjuvant treatment.
Treatment sequencing
Unresectable, metastatic melanoma
SECOMBIT (NCT02631447)
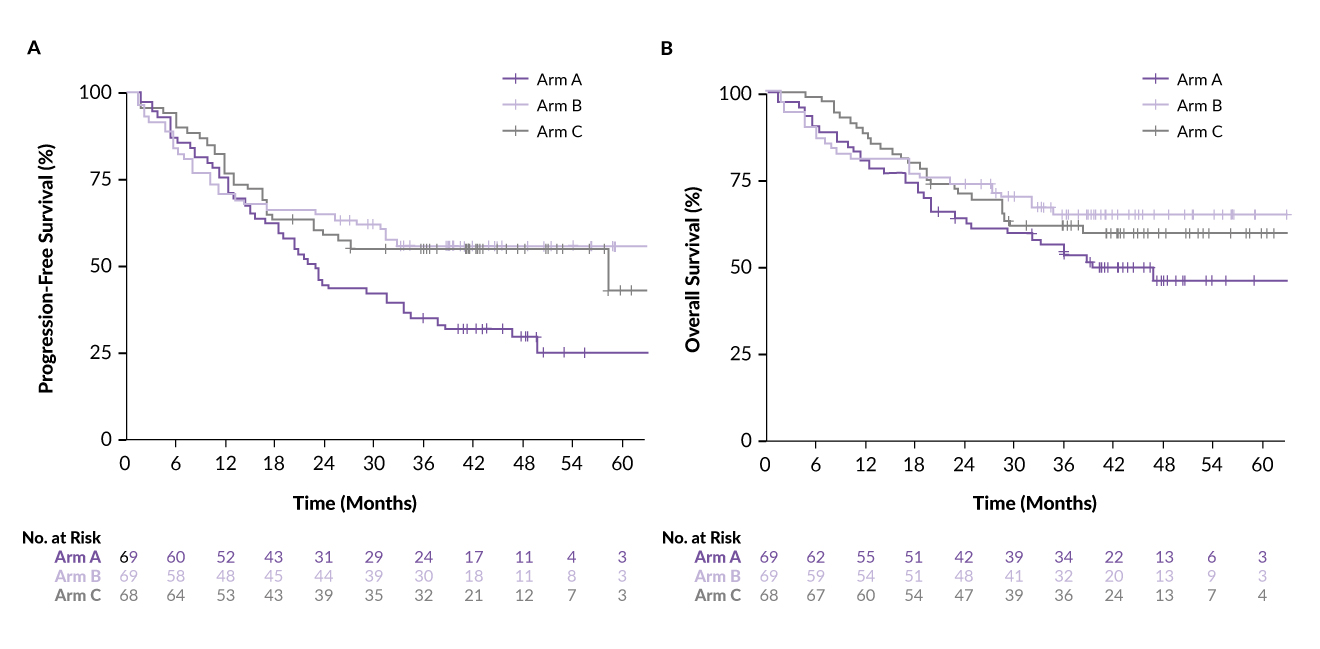
This open-label, phase II study evaluated the sequential use of immunotherapy using dual blockade of PD-1 and CTLA-4 and targeted therapy using the BRAF/MEKi combination in metastatic BRAFV600-mutated melanoma.50 A total of 209 patients were randomized 1:1:1 into one of three treatment arms: Arm A (encorafenib plus binimetinib until PD followed by ipilimumab plus nivolumab), Arm B (ipilimumab plus nivolumab until PD followed by encorafenib plus binimetinib) and Arm C (encorafenib plus binimetinib for eight weeks followed by ipilimumab plus nivolumab until PD followed by encorafenib plus binimetinib). The primary endpoint of OS (median OS >15 months) was met in each arm. At a median follow-up of 37.1 months, 2- and 3-year OS rates were 62% and 53% in Arm A, 73% and 63% in Arm B and 69% and 60% in Arm C, respectively.51
A 4-year follow-up confirmed the long-term benefit of first-line immunotherapy.49 The 3- and 4-year total PFS (time from randomization until second progression) rates for Arms A, B and C were 34% and 29% for Arm A, 55% and 55% for Arm B and 54% and 54% for Arm C, respectively (Figure 4A). OS rates at 3 and 4 years were 53% and 46% for Arm A 64% and 64% for Arm B, and 61% and 59% for Arm C, respectively (Figure 4B). In summary, sequential immunotherapy and targeted therapy provide clinically meaningful survival benefits for patients with BRAFV600-mutated melanoma.
_progression-free_survival_(pfs)_and_b)_overall_survival_(os)_in_the_secombit_study.jpg)
DREAMseq (NCT02224781)
In this phase III clinical trial, patients with unresectable treatment-naïve BRAF-mutated advanced melanoma were randomized to receive either ICI with ipilimumab/nivolumab upfront (Arm A) and change to BRAF/MEKi with dabrafenib/trametinib at progression (Arm C), or to receive BRAF/MEKi upfront (Arm B) and change to ICI upon progression (Arm D).69 The primary endpoint was the 2-year OS rate. Patients randomized to receive upfront ICI demonstrated a significantly improved 2-year OS rate of 71.8% compared with 51.5% in patients randomized to receive BRAF/MEKi upfront (p=0.01). These results are in line with the SECOMBIT data50 and suggest that in metastatic disease, first-line therapy with ICI shows better long-term outcomes, irrespective of BRAF mutation status.
Tumor-infiltrating lymphocytes
Adoptive cell therapy with TILs is a novel immunotherapy-based therapeutic modality developed in recent years.24 Using T cells isolated from patient’s tumors or genetically modified T cells expressing T-cell receptors specific to tumor antigens, the cancer cells can be specifically and effectively targeted, with reduced cross-reactivity against normal tissues. These therapies can therefore overcome some of the limitations of ICI. Therapies based on genetically modified autologous TILs have shown promising results in phase II/III trials for metastatic melanoma, with long-term clinical benefit even in patients progressing on ICIs and/or BRAF/MEKi.70,71
Advanced melanoma
NCT02278887
In this multicenter, open-label, phase III trial, 168 patients with unresectable stage IIIC or IV melanoma were randomized at 1:1 ratio to receive TILs or ipilimumab.71 The primary endpoint was PFS. In the ITT population, TIL therapy significantly prolonged PFS in the ITT population compared with ipilimumab, with median PFS of 7.2 months versus 3.1 months, respectively (HR: 0.50 [95% CI: 0.35–0.72]; p<0.001). The ORR was 49% versus 21% and the median OS was 25.8 months versus 18.9 months in the TIL arm versus ipilimumab arm, respectively. Grade ≥3 TRAEs occurred in all patients treated with TILs compared with 57% of those who received ipilimumab. TRAEs in the TIL arm were mostly comprised of chemotherapy-related myelosuppression.
C-144-01 (NCT02360579)
In this prospective, open-label, multicohort, nonrandomized phase II trial, 153 patients with advanced melanoma previously treated with ICIs and BRAF/MEK-targeted agents received a one-time autologous TIL cell therapy lifileucel.54 A recently presented data with an extended follow-up of 48.1 months showed an ORR of 31.4% and a median DoR of NR, with 1-, 2-, 3- and 4-year OS rates of 54.0%, 33.9%, 28.4% and 21.9%, respectively.55 All responders (n=48) including patients with early, late and deepened response demonstrated clinically meaningful 4-year OS rates, with a numerically higher OS rate (68.2%) observed in patients with deepened response (those who had stable disease [SD] and improved to confirmed PR or had PR and improved to confirmed CR). The safety profile was consistent with that previously reported for lymphodepletion and interleukin-2 (IL-2). In summary, investigational therapy with lifileucel demonstrated clinically meaningful activity and durable efficacy, leading to long-term survival benefits in heavily pretreated patients with advanced melanoma.
Collective analysis of three trials
In another study, data on 44 patients who received TIL therapy for advanced melanoma were collected from three clinical trials (NCT00937625, NCT02379195 and NCT02354690).56 Patients were followed for a minimum of five years. One patient achieved CR and seven patients achieved complete metabolic response (CMR). PR was observed in 14 patients and partial metabolic response (PMR) in six patients. At a median follow-up of 108 months, six of the seven patients with CMR were alive (one death was not related to melanoma) and five (71%) were progression-free. Early CMRs on [18F]2-fluoro-2-deoxy-d-glucose positron emission tomography-computed tomography (FDG-PET/CT) strongly predicted long-term survival after TIL therapy in these patients.
NCT04217473
This open-label, dose-escalating, multicenter, phase I trial evaluated the combination of multiple intravenous and intratumoral injections of the oncolytic adenovirus igrelimogene litadenorepvec (TILT-123) with TILs (administered without pre- or post-conditioning treatment regimens) in 16 patients with stage IV melanoma.57 The primary endpoint was the safety of TILT-123 and the secondary endpoints included the safety and efficacy of TILT-123 plus TILs. The most frequent TRAEs were fever (63%) and pain at the injection site (44%), with no increase in the severity of AEs associated with the combination regimen. In terms of efficacy, the study reported one durable CR, one ongoing PR and two cases of SD lasting for >10 months. These results suggest that this combination treatment may help avoid some of the toxicities associated with pre-conditioning chemotherapy or post-conditioning IL-2 therapy.
Discussion
Most of above discussed clinical trials have resulted in approval of new treatment regiments or have shaped treatment strategies using approved drugs. After the first trials with checkpoint inhibitors, which each demonstrated better outcomes than the previous, excitement and expectations were growing. However, it seems like the limitations of checkpoint inhibitors may have been reached as in metastatic disease, as no checkpoint combination or monotherapy has outperformed efficacy of ipilimumab and nivolumab yet. Relatlimab and nivolumab (RELATIVITY 047) may be an alternative for anti-PD1 monotherapy, however, the PD-L1<1%-restricted approval in Europe limits its use. Changing the structure to enhance efficacy is one strategy that is currently being explored.72 Targeting new immune checkpoints or investigating new combinations may be another strategy; however, choosing the right target and indication becomes crucial as a few phase III trials have demonstrated negative results lately.73,74 Furthermore, after changing SoC in other indications, including uveal melanoma, bispecific antibodies or immune-mobilizing monoclonal T-cell receptors (ImmTACs) are being investigated in melanoma.75
Given the very common secondary resistance, targeted therapy has less traction than immunotherapy in cutaneous melanoma. Nevertheless, new molecules, especially BRAF inhibitors, are being investigated76–78 and may delay development of resistance.
Neoadjuvant therapy in macroscopic stage III disease is already changing clinical practice. However, predictive biomarkers are needed in order to choose the right treatment strategy (monotherapy or combination), the role of subsequent adjuvant therapy should be investigated in larger groups, and survival data are still missing. Pushing the neoadjuvant approach to even earlier stages is an interesting approach and merits consideration.
Selection of patients for first-line mono- or combination therapy, the second-line approaches, treatment of special patient populations, such as patients with leptomeningeal disease or solid brain metastases, and rapid progression are just a few unmet needs that merit further investigation, not only in terms of clinical trials, but also on translational and clinical data level.
Conclusions
-
The incidence of melanoma in Switzerland remains high, which represents a significant health and economic burden.
-
Over the last decade, approved treatment options for patients with melanoma have expanded greatly, and many trials are planned or ongoing to optimize the use of currently available therapies.
-
There remain unmet medical needs, such as improving OS, reducing immune-related toxicity and improving care for selected subgroups of patients (e.g., anti-PD-1-resistant or refractory patients without BRAF mutation).
-
TIL therapy represents a novel addition to the current treatment armamentarium, with promising results in pretreated populations.
Conflict of interest
The authors have declared that the manuscript was written in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors have declared that no financial support was received from any organization for the submitted work.
Author contributions
All authors contributed to and approved the final manuscript.