Introduction
As the sixth most common cancer among women,1 endometrial cancer presents a global healthcare challenge. The global incident cases of endometrial cancer increased 2.3 times from 187,190 in 1990 to 435,040 in 2019; this rise is particularly evident in high-income regions or countries.2 Endometrial cancer primarily affects older patients (>60 years of age), although it can also occur in younger women.3 In Switzerland, endometrial cancer is the fifth most common cancer among women, accounting for 4.2% of cases, with nearly 1,000 patients being diagnosed each year and slightly more than 200 deaths per year.4–6 Although the age-standardized incidence of endometrial/uterine cancers of unspecified origin has been decreasing in Switzerland current models predict this trend to level off in the near future.4 In general, long-term remission rates are high for localized disease, with a 5-year survival rate of 95%.7 However, there is an unmet need among patients with advanced or metastatic endometrial cancer, where 5-year survival rate drops to 18%.
Molecular classification of endometrial cancer
Recent advancements, first due to the launch of the Cancer Genome Atlas (TGCA) Research Network and later with the development of the Proactive Molecular Risk Classifier for Endometrial Cancer (ProMisE) system, have improved the molecular characterization of endometrial cancer subtypes. These advancements provide a greater understanding of the drivers of disease in these tumors and better inform the rationale behind the development of novel therapies for patients with endometrial cancer. The ProMisE system classifies endometrial tumors into four distinct subtypes: POLE-mutated (POLEmut), deficient mismatch repair (dMMR), p53 wild-type and p53 abnormal.8,9 The benefit of the ProMisE system is that it removes some of the interobserver variability that can occur when using clinicopathological features (e.g., cancer stage, histologic grade and tumor subtype) in endometrial cancer staging.10–12
Rationale for targeted therapies and immunotherapies
Generally, the standard of care (SoC) for patients with advanced disease is carboplatin and paclitaxel. At the same time, no SoC exists in the second line, but doxorubicin and paclitaxel are considered the most active therapies.13 However, outcomes among patients with advanced or recurrent disease remain poor and many targeted therapies are under assessment in clinical trials.14–20 The National Cancer Institute (NCI) Gynecological Cancers Steering Committee has prioritized and published a list of potential targets and therapeutic opportunities in endometrial cancer.21 Among them are DNA repair and hormone receptor pathways, the phosphatidylinositol-3-kinase (PI3K)/protein kinase B (AKT)/mammalian target of rapamycin (mTOR) pathway, human epidermal growth factor receptor 2 (HER2) pathway, immune- and obesity-related pathways, the Wnt pathway, as well as ubiquitin-ligase complexes and chromatin remodeling. Immunotherapy has proven to be a particularly valuable therapeutic option for patients with advanced or recurrent endometrial cancer22–24; however, not all patients respond to this treatment. Thus, there is an unmet need to develop more robust screening and treatment options for broader patient populations. Poly (ADP-ribose) polymerase (PARP) inhibitors have previously shown great success in treating patients with ovarian and triple-negative breast cancers, particularly in tumors with DNA repair pathway defects, such as homologous recombination deficient (HRD) tumors25,26; similar defects are seen in endometrial cancer (e.g., mutations p53 and PTEN).19,27,28 POLEmut and microsatellite instability (MSI)/dMMR tumors, which represent 7–12% and 30% of endometrial tumors, respectively, are highly immunogenic as they have a high mutational burden, leading to the production of a large number of neoantigens.29–31 The tumor microenvironment, including the presence of intraepithelial CD3+ and CD8+ tumor-infiltrating lymphocytes,32,33 can aid immunotherapy; immune checkpoint proteins such as programmed cell death protein 1 (PD-1)/programmed death-ligand 1 (PD-L1) are also often upregulated in the tumor microenvironment.29 For these reasons, POLEmut and MSI/dMMR tumors respond well to checkpoint inhibitors such as pembrolizumab, nivolumab, dostarlimab and avelumab.19 Based on the available evidence, the current data support the rationale of researching novel immunotherapies across all subtypes of endometrial cancer.
Current treatment landscape in advanced or recurrent endometrial cancer
Single-agent immunotherapy in advanced/recurrent endometrial cancer
The benefits of single-agent immune checkpoint inhibitors have been investigated in several phase I/II studies of patients with pretreated metastatic, advanced, recurrent or persistent endometrial cancer: KEYNOTE-158 (NCT02628067), PHAEDRA (NCT03015129), GARNET (NCT02715284), KEYNOTE-28 (NCT02054806), as well as small pembrolizumab (NCT02899793) and avelumab (NCT02912572 trials.34–38 Notably, when looking at separate cohorts, patients with dMMR and/or MSI-high (MSI-H) disease performed far better than those with proficient mismatch repair (MMRp) and/or MSI-negative disease. The safety profile of single-agent immunotherapy in these trials was consistent with that observed previously and no treatment-associated deaths were reported.
In KEYNOTE-158, the efficacy of anti-PD-1 monoclonal antibody (mAb) pembrolizumab was assessed in patients with recurrent/metastatic non-colorectal cancer (n=233, 90 patients had MSI-H/dMMR endometrial cancer).35,39 The primary endpoint was the objective response rate (ORR) per Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1, assessed by independent central radiologic review. Treatment with pembrolizumab led to an ORR of 48%, while the median duration of response (DoR) was not reached; 68% of responders were estimated to have a DoR of ≥3 years and a median progression-free survival (PFS) was 13.1 months. Overall survival (OS) data were immature at the time of analysis. Treatment-related adverse events (TRAEs) were reported in 76% of patients (grade 3–4, 12%).
A phase II study (NCT02899793) assessed pembrolizumab in patients with dMMR/MSI-H recurrent or persistent endometrial cancer with a median of one prior line of chemotherapy (n=25).34 Lynch/Lynch-like tumors were present in 75% of patients, while the rest had sporadic endometrial cancer. The primary endpoint was ORR. In patients with Lynch/Lynch-like tumors, the ORR was significantly higher than in those with sporadic disease (100% vs 44%; p=0.024). The 3-year PFS and OS rates were 100% versus 30% (p=0.017) and 100% versus 43% (p=0.043), respectively. These results suggest that Lynch status may be of prognostic value in determining treatment options for dMMR/MSI-H disease. However, the advantages of immunotherapy in Lynch tumors compared with other non-Lynch dMMR tumors have not been confirmed in some larger trials.40
In the non-randomized PHAEDRA trial, patients with dMMR or MMRp pretreated advanced endometrial cancer (n=71) received anti-PD-L1 mAb durvalumab.36 The primary endpoint was objective tumor response rate (OTRR). The study demonstrated higher efficacy of durvalumab in the dMMR cohort compared with patients with MMRp tumors, with OTRR of 47% versus 3% and a median PFS of 8.3 months versus 1.8 months, respectively. The 12-month OS rates were 71% in dMMR patients versus 51% in those with MMRp, with the median OS not reached for dMMR versus 12 months for MMRp. Notably, patients with dMMR disease were more likely to have received durvalumab as first-line therapy (60% vs 8%). In terms of safety, AEs were reported in 93% of patients, with 14 patients having immune-related AE.
In a phase II study (NCT02912572) investigating the efficacy of anti-PD-L1 mAb avelumab in 33 patients with chemotherapy-pretreated dMMR or MMRp recurrent endometrial cancer, this anti-PD-L1 antibody demonstrated greater efficacy in the dMMR versus MMRp subgroups (ORR, 26.7% vs 6.3%; median PFS, 4.4 months vs 1.9 months), respectively.37 This result was particularly noteworthy, considering that the population in question was heavily pre-treated, with 71% of patients having received ≥2 prior lines of therapy.
GARNET, the largest single-agent immune checkpoint inhibitor trial in solid tumors, enrolled patients with dMMR/MSI-H and MMRp/microsatellite stable (MSS) advanced or recurrent after ≤2 prior lines of treatment.38 This trial showed a clear benefit with PD-1-targeting mAb dostarlimab in patients with dMMR/MSI-H versus MMRp/MSS disease (ORR, 45.5% vs 15.4%; median DoR, not reached vs 19.4 months; median PFS, 6.0 months vs 2.7 months; median OS, not reached vs 16.9 months), respectively.38,41
In the phase Ib KEYNOTE-28 trial, patients likely to respond to treatment with pembrolizumab were selected based on PD-L1 expression.42 A small cohort of patients with previously treated locally advanced or metastatic PD-L1-positive disease achieved an unfavorable ORR of 13.0%, with a median PFS of 1.8 months and a median OS of not reached. The safety profile was consistent with previous data and no treatment-associated deaths were observed.
Combination immunotherapy in advanced/recurrent endometrial cancer
The phase III KEYNOTE-775 trial (endometrial cancer cohort, n=300) assessed the benefit of pembrolizumab plus tyrosine kinase inhibitor lenvatinib combination therapy versus the physician’s choice of chemotherapy (doxorubicin or paclitaxel) in patients with advanced, recurrent or metastatic endometrial cancer.43 The coprimary endpoints were PFS and OS. Patients were stratified according to MMR status (dMMR tumors, 16% of the total population). Long-term follow-up supports the benefit of lenvatinib plus pembrolizumab compared with chemotherapy in PFS (MMRp, HR: 0.60 [95% CI: 0.50–0.72]; overall population, HR: 0.56 [95% CI: 0.47–0.66]), OS (MMRp, HR: 0.68 [95% CI: 0.56–0.84]; overall population, HR: 0.62; [95% CI: 0.51–0.75]) and ORR (MMRp, 32.4% vs 15.1%; all-comers, 33.8% vs 14.7%).44 OS, PFS and ORR favored lenvatinib plus pembrolizumab in all subgroups of interest. No new safety signals were observed, with slightly higher rates of grade ≥3 TEAEs in the combination arm compared with the chemotherapy arm (90.1% vs 73.7%) and similar rates of grade 5 TEAEs in both arms (6.4% vs 5.2%). Treatment discontinuations due to TEAEs occurred more frequently with lenvatinib plus pembrolizumab (39.2%) compared with chemotherapy (8.0%).
First-line immunotherapy in metastatic/recurrent endometrial cancer
Following the success of immunotherapy in heavily pretreated patients, a number of phase III trials have investigated the combination of immunotherapy with chemotherapy at early recurrence, including RUBY, NRG-GY018, AtTEnd and DUO-E. These trials have reported remarkable PFS and OS benefits with immunotherapy plus chemotherapy, with one pooled analysis from 2,320 patients across these trials showing a significant improvement in PFS compared to chemotherapy alone (HR: 0.70 [95% CI: 0.62–0.79]) across all patient groups, with a particular benefit in dMMR/MSI-H tumors (n=563; HR: 0.33 [95% CI: 0.23–0.43]).45 Some trials showing no benefit of immunotherapy include the phase II MITO END-3 (NCT03503786) and phase III LEAP-001 (NCT03884101) trials.
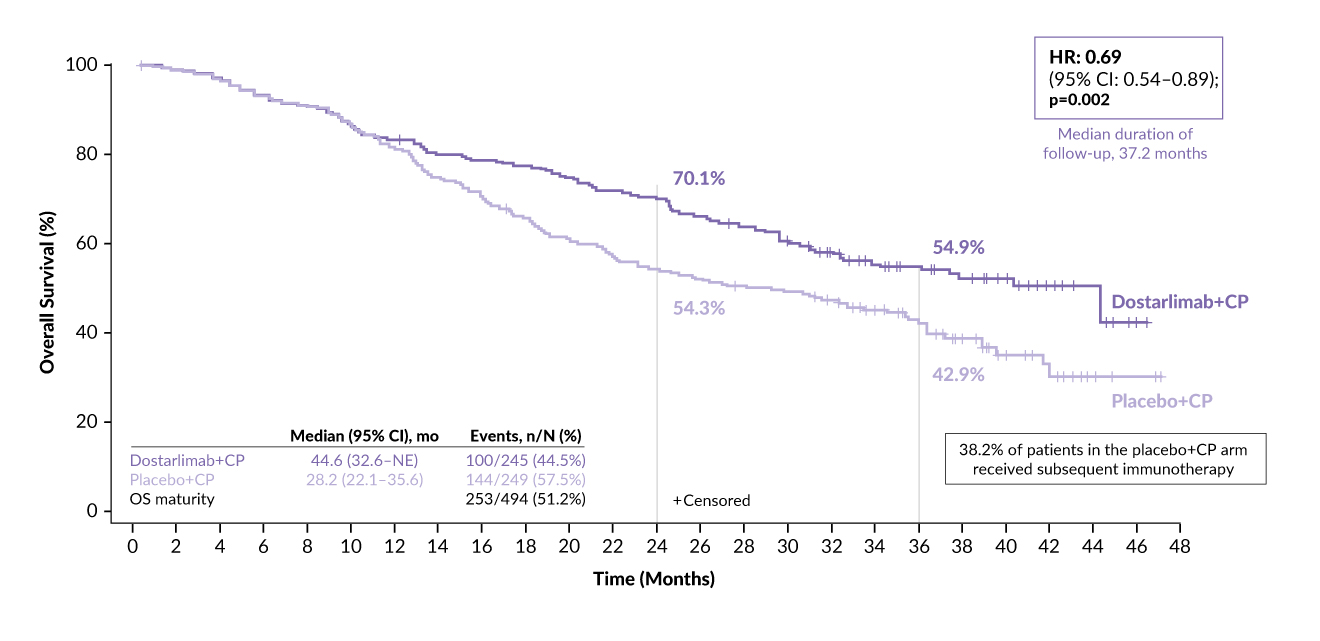
The phase III RUBY trial (NCT03981796) evaluated dostarlimab plus chemotherapy with or without the addition of niraparib in the maintenance setting in patients (n=494) with advanced or recurrent endometrial cancer.23,24,46 Part 1 of this study assessed dostarlimab plus SoC chemotherapy (carboplatin/paclitaxel) followed by dostarlimab compared with chemotherapy plus placebo followed by placebo. The co-primary endpoints were PFS per RECIST version 1.1 and OS. With a median follow-up of 24.8 months, patients in the dostarlimab arm had an improved PFS versus the control arm.23,24 In the dMMR/MSI-H population, the median PFS was not reached versus 7.7 months (HR: 0.28 [95% CI: 0.16–0.50]; p<0.001), with 24-month PFS rates of 61.4% versus 15.7% with dostarlimab versus placebo, respectively. In the overall population, the 24-month PFS rates were 36.1% versus 18.1%, respectively (HR: 0.64 [95% CI: 0.51–0.80]; p<0.0001). The OS rates at 24 months were 71.3% with dostarlimab versus 56.0% with placebo (HR: 0.64 [95% CI: 0.46–0.87]; p=0.0021).
In the updated analysis of RUBY presented at the SGO 2024 meeting, dostarlimab continued to provide OS benefit compared with placebo at a median follow-up of 37.2 months.47 In the overall population, the median OS was 44.6 months versus 28.2 months (HR: 0.69 [95% CI: 0.54–0.89]; p=0.002), corresponding to a 31% reduction in the risk of death (Figure 1). A pre-specified exploratory analysis of the MMRp/MSS population showed a clinically meaningful trend in reduced risk of death by 21% (HR: 0.79 [95% CI: 0.602–1.044]) and a clinically meaningful improvement in median OS (34.0 months vs 27.0 months) with dostarlimab versus placebo, respectively. These data demonstrate that RUBY is the first clinical trial to achieve a statistically significant and clinically meaningful improvement in OS for immuno-oncology therapy in combination with chemotherapy in the overall population of patients with primary advanced or recurrent endometrial cancer. The addition of dostarlimab to chemotherapy may potentially benefit a broader population of patients with this type of cancer. Supported by the RUBY results, dostarlimab plus carboplatin and paclitaxel followed by single-agent dostarlimab received Food and Drug Administration (FDA) approval for treating patients with dMMR/MSI-H advanced or recurrent endometrial cancer.48

The phase III NRG-GY018 trial (NCT03914612) investigated the safety and efficacy of pembrolizumab plus carboplatin and paclitaxel in patients (n=816) with stage III/IVA, stage IVB, or recurrent endometrial cancer.49,50 The primary endpoint was investigator-assessed PFS in dMMR and MMRp populations.49 Pembrolizumab treatment led to greater benefits in efficacy compared with placebo both in patients with dMMR (ORR, 82% vs 71%; median DoR, 28.7 months vs 6.2. months; HR: 0.22 [95% CI: 0.13–0.37]; p<0.0001]) and MMRp (ORR, 71% vs 58%; median DoR, 9.2 months vs 6.2 months; HR: 0.47 [95% CI: 0.34–0.64]; p<0.0001]) disease. In the 12-month analysis, PFS rates in the dMMR cohort were 74% in the pembrolizumab group versus 38% in the placebo group (HR: 0.30 [95% CI: 0.19–0.48; p<0.0001), translating into a 70% difference in relative risk.49 In the MMRp cohort, the median PFS was 13.1 months with pembrolizumab versus 8.7 months with placebo (HR: 0.54 [95% CI: 0.41–0.71; p<0.0001). Although the OS data are still immature, an interim analysis of the trial suggested a trend favoring pembrolizumab over placebo. The median OS was 27.9 months versus 27.4 months (HR: 0.79 [95% CI: 0.53–1.17]; p=0.1157) with pembrolizumab versus placebo among patients with MMRp and not reached in either arm (HR: 0.55 [95% CI: 0.25–1.19]; p=0.0617) in the dMMR population.51 An analysis by PD-L1 expression status (combined positive score <1 vs combined positive score ≥1), showed that PFS improved regardless of expression level. The AEs reported in this trial were as expected for pembrolizumab and combination chemotherapy,49 with a similar incidence of immune-mediated toxicities as previously reported with pembrolizumab monotherapy.39 These subgroup analyses support the consistent benefit of combining pembrolizumab with chemotherapy in the relevant subgroups, even those with prior systemic adjuvant chemotherapy, newly diagnosed, advanced, or recurrent disease, and those with more aggressive disease.
In the phase III AtTEnd study (NCT03603184), patients with stage III or IV newly diagnosed or recurrent endometrial cancer (n=549) were randomized to receive anti-PD-L1 mAb atezolizumab or placebo, plus carboplatin and paclitaxel, followed by atezolizumab or placebo maintenance.52 The co-primary endpoints with a hierarchical approach were PFS (dMMR population) and PFS/OS in the overall population.52 At a median follow-up of 28.3 months in the overall population, patients receiving atezolizumab achieved a statistically significant improvement in median PFS compared with those receiving placebo (10.1 months vs 8.9 months; HR: 0.74 [95% CI: 0.61–0.91]; log-rank p=0.0219). The PFS improvement with atezolizumab versus placebo was even greater in the dMMR group patients at a median follow-up of 26.2 months (not estimable vs 6.9 months; HR: 0.36 [95% CI: 0.23–0.57]; p=0.0005).52 At 43% data maturity, the interim analysis showed a trend for longer median OS in the atezolizumab arm compared with the placebo arm (38.7 months vs 30.2 months; HR: 0.82 [95% CI: 0.63–1.07]; log-rank p=0.0483).52 Similar to the median PFS, the reported median OS improvement was even greater in the dMMR population among patients receiving atezolizumab versus placebo (not estimable vs 25.7 months; HR: 0.41 [95% CI: 0.22–0.76]). The safety profile for atezolizumab plus chemotherapy was manageable and consistent with previously reported data.52 An exploratory subgroup analysis of patients with MMRp disease did not show any benefit for atezolizumab versus placebo in terms of PFS (HR: 0.92 [95% CI: 0.73–1.16]) or OS (HR: 1.00 [95% CI: 0.74–1.35]), contrary to the benefit of PD-1-targeting agents in this population, as reported in RUBY and NRG-GY018.
The results of the phase II MITO END-3 and phase III LEAP-001 trials were less promising than those reported in RUBY, NRG-GY018 and AtTEnd. MITO END-3 (NCT03503786) assessed the efficacy of adding avelumab to carboplatin and paclitaxel in patients with stage III–IV or recurrent endometrial cancer (n=125); however, with a median follow-up of 23.3 months, it failed to meet its primary endpoint of PFS in the intention-to-treat (ITT) population.53 Patients receiving carboplatin and paclitaxel experienced a slightly better median PFS than those in the avelumab arm (9.9 months vs 9.6 months; HR: 0.78 [60% CI: 0.65–0.93]; one-tailed p=0.085). The median OS was 27.4 months in the carboplatin and paclitaxel arm but not yet reached in the avelumab arm (HR: 1.13 [95% CI: 0.62–2.07]; p=0.91). Treatment with avelumab also led to a higher incidence of serious AEs compared with the carboplatin and paclitaxel arm (24 events vs seven events).
The LEAP-001 study (NCT03884101) assessed the benefit of first-line pembrolizumab plus lenvatinib compared with carboplatin and paclitaxel in patients with advanced or recurrent endometrial cancer (n=842).54–56 This study failed to meet the co-primary endpoints of PFS and OS.53,56 At a median follow-up of 38.4 months, the final analysis for MMRp patients showed no benefit pembrolizumab/lenvatinib versus chemotherapy, either for median PFS (9.6 months vs 10.2 months; HR: 0.99 [95% CI: 0.82–1.21]) or median OS (30.9 months vs 29.4 months; HR: 0.93 [95% CI: 0.77–1.12]). However, combination therapy was more effective than chemotherapy in dMMR patients, as well as in a subgroup of MMRp patients who received prior neoadjuvant or adjuvant chemotherapy, at providing durable improvements to both PFS and OS, supporting its use in these populations. While the rates of any-grade AEs were similar, lenvatinib/pembrolizumab resulted in more dose interruptions and discontinuations compared with chemotherapy (71.7% vs 40.9% and 47.4% vs 19.5%, respectively). Regarding any-grade AEs of special interest, the lenvatinib/pembrolizumab combination was comparable with pembrolizumab monotherapy, except for increases in hypothyroidism (62.3%), hyperthyroidism (16.4%), and colitis (5.2%).
KEYNOTE-c93 (NCT05173987) is a phase III trial evaluating the efficacy of first-line pembrolizumab monotherapy versus SoC carboplatin and paclitaxel in patients with dMMR advanced or recurrent endometrial cancer; recruitment is ongoing and the primary study completion is expected in July 2027.57,58
PARP inhibitors
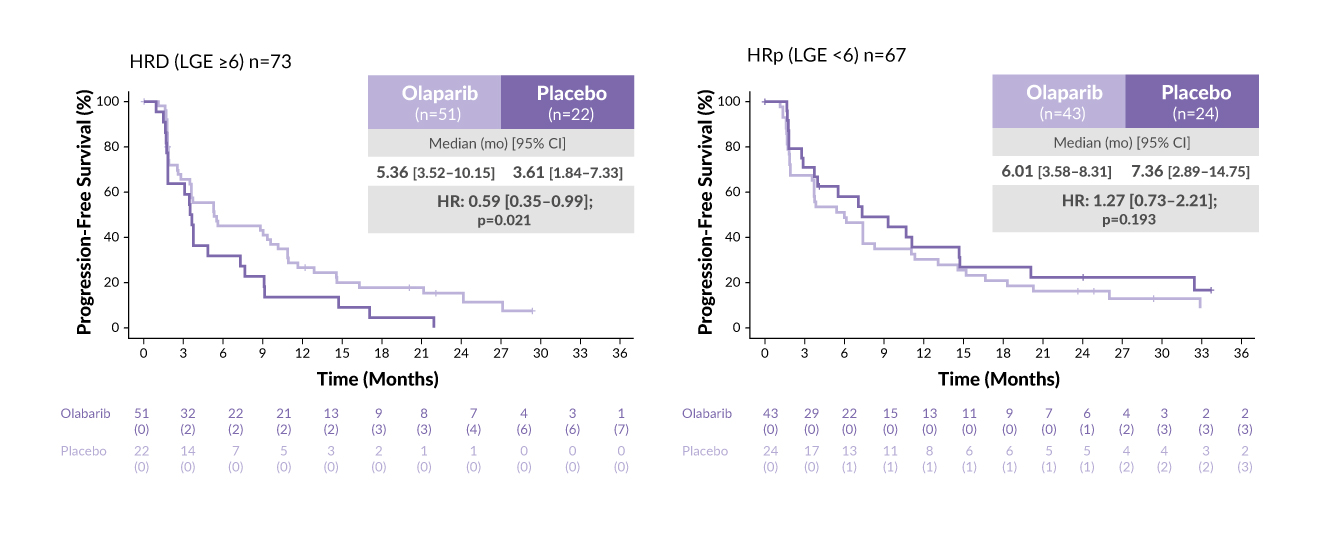
UTOLA (NCT03914612) is a randomized, double-blind, placebo-controlled, phase II study assessing the efficacy of maintenance olaparib versus placebo in patients (n=147) with advanced or recurrent endometrial cancer.59 Patients were stratified by p53 status, MMR status and response to the previous chemotherapy. The primary endpoint was PFS in the ITT population, and a prespecified PFS analysis was performed according to HRD status defined by the number of large genomic events. The molecular classification showed that 53% of tumors were p53 mutated, 35% had no specific molecular profile, 12% had dMMR and one tumor was POLEmut. Overall, 52% of patients were HRD-positive and 74% of patients with p53 mutated tumors were HRD-positive. Adding maintenance olaparib led to numerical improvement in PFS in the ITT population (5.6 months vs 4.0 months with placebo; HR: 0.94, p=0.36) and p53 mutated subgroup (5.6 months vs 3.6 months; HR: 0.75, p=0.12), whereas a statistically significant improvement was observed in the HRD subgroup (5.4 months vs 3.6 months; HR: 0.59, p=0.021) (Figure 2).59 However, patients with p53 wild-type tumors did not benefit from the addition of olaparib (6.0 months vs 7.7 months; HR: 1.13, p=0.329). In this study, no difference was observed in OS in any subgroup. The safety profile of olaparib was similar to that seen in other tumor types. These data support further investigation into the benefit of PARP inhibitors in prolonging PFS in patients with HRD, advanced or recurrent endometrial cancer.59
_according_to_homologous_recombination_deficiency_(hrd)_sta.jpg)
Part 2 of the phase III RUBY trial (NCT03981796) evaluated dostarlimab plus chemotherapy with or without the addition of niraparib in the maintenance setting of advanced or recurrent endometrial cancer.23,24,46 Patients (n=291) were randomized 2:1 to receive dostarlimab plus chemotherapy, followed by dostarlimab plus niraparib as maintenance therapy (n=192) or chemotherapy plus placebo followed by placebo (n=99). The primary endpoint was investigator-assessed PFS. The trial met its primary endpoint, with patients in the combination arm experiencing improved survival outcomes compared with those in the control arm. At a median follow-up of 19 months, the median PFS in the overall population was 14.5 months versus 8.3 months (HR: 0.60 [95% CI: 0.43–0.82]), with a statistically significant 40% reduction in the risk of disease progression or death (HR: 0.60 [95% CI: 0.43–0.82]).46 Similar results were reported among MMRp/microsatellite stable patients.
Grade ≥3 AEs were more frequent in the treatment arm than in the control arm (84% vs 49%, respectively) and the rates of immune-related AEs were also higher in the treatment arm (36.6% vs 6.3%). Discontinuation of dostarlimab/niraparib due to TEAEs was more frequent than that for their respective placebo (24.1% vs 5.2% and 15.7% vs 4.2%, respectively).
In a phase II study (NCT03617679), the effect of maintenance rucaparib was assessed in patients with advanced or recurrent endometrial cancer.60 Although the trial ended early, with 79 patients recruited, it met its primary endpoint of improved PFS. The baseline characteristics were balanced between both arms of this trial; approximately one-third had stage III disease, half had stage IV disease and 25–30% were in the recurrent setting. In comparison with the placebo arm, patients in the rucaparib arm had significantly prolonged PFS (median, 28.1 months vs 8.7 months; HR: 0.45 [95% CI: 0.26–0.80]; p=0.005). The median OS was not reached with rucaparib versus 28.4 months with placebo (HR: 0.48 [95% CI: 0.23–1.03]; p=0.055). TRAEs were as expected based on previous data from rucaparib in other tumors, with nausea, fatigue, anemia, thrombocytopenia and elevated aspartate transaminase/alanine transaminase levels being the most commonly reported. Grade ≥3 TRAEs were reported in 36% of patients receiving rucaparib, and TRAEs leading to dose interruptions, reductions and discontinuations occurred in 36%, 33% and 8% of patients receiving rucaparib, respectively.
The benefit of durvalumab was assessed in the DUO-E trial (NCT04269200) where patients with newly diagnosed stage III or IV or recurrent endometrial cancer (n=718) received durvalumab plus carboplatin and paclitaxel followed by maintenance durvalumab plus the PARP inhibitor olaparib.22,61 Patients were randomized 1:1:1 into three arms: Arm 1, carboplatin and paclitaxel plus durvalumab placebo followed by placebo maintenance (control); Arm 2, carboplatin and paclitaxel plus durvalumab followed by maintenance durvalumab plus olaparib placebo; Arm 3, carboplatin and paclitaxel plus durvalumab followed by maintenance durvalumab plus olaparib.52,61 The coprimary endpoints were investigator-assessed PFS per RECIST version 1.1 in the durvalumab arm versus control and the durvalumab plus olaparib arm versus control. In the ITT population, the durvalumab arm had a statistically significant 29% lower risk of disease progression or death versus the control arm (median PFS, 10.2 months vs 9.6 months; HR: 0.71 [95% CI: 0.57−0.89]; p=0.003). The durvalumab plus olaparib arm had a statistically significant 45% lower risk of disease progression or death versus the control arm (median PFS, 15.1 months vs 9.6 months; HR: 0.55 [95% CI: 0.43−0.69]; p<0.001).22,61 The interim OS data, while being immature (27.7%), showed a trend towards benefit with the addition of durvalumab (durvalumab vs control, HR: 0.77 [95% CI: 0.56–1.07]; p=0.120; durvalumab plus olaparib vs control, HR: 0.59 [95% CI: 0.42–0.83]; p=0.003). PFS subgroup analysis of patients with dMMR and MMRp showed that both durvalumab-containing arms had greater benefits than the control arm. In patients with MMRp disease, both durvalumab-containing arms showed a benefit over control. However, the reduction in the risk of progression or death was 29% higher in the olaparib-containing arm. The safety profiles of the treatment arms were generally consistent with those previously reported for the individual therapies.
Antibody-drug conjugates
Antibody-drug conjugates (ADCs) represent a promising new treatment modality for cancer.62 The ADC molecule consists of three main components: a highly selective monoclonal antibody for a tumor-associated antigen, a potent cytotoxic agent and a linker. ADCs are an active area of research in endometrial cancer, with several drugs targeting various tumor antigens being evaluated in ongoing clinical trials. Mirvetuximab soravtansine, an ADC targeting folate receptor (FR)α, exhibited evidence of clinical activity in combination with pembrolizumab in recurrent pMMR/MSS FRα -positive serous endometrial cancer.63
HER2 represents another potential therapeutic target in endometrial cancer. High HER2 expression has been reported in approximately 35% of patients with uterine serous carcinoma.64,65 The open-label, multicohort phase II DESTINY-PanTumor02 study (NCT04482309 evaluated HER2-directed ADC trastuzumab deruxtecan (T-DXd) in patients with HER2-expressing locally advanced or metastatic disease after ≥1 systemic treatment or without alternative treatments.66 A total of 267 patients across seven tumor cohorts, including endometrial, cervical, ovarian, bladder, biliary tract, pancreatic and other cancers, were enrolled. The primary endpoint was the investigator-assessed ORR. In the endometrial cancer cohort (n=40), 77.5% of patients had ≥2 prior lines of therapy.
In the primary analysis at a median follow-up of 12.75 months, patients in the endometrial cancer cohort displayed an ORR of 57.5%, as assessed by investigator and blinded independent central review, and the median DoR was not reached.66 The median PFS was 11.1 months, and the median OS was 26.0 months. The safety profile of T-DXd was consistent with previously reported data, including the incidence of interstitial lung disease. In this study, the magnitude of benefit for T-DXd therapy was the greatest among gynecological cancers, with the highest benefit among endometrial cancer patients.66 The DESTINY-PanTumor02 study is the first to report on HER2-directed ADC therapy in these gynecological tumors, showing durable responses and clinically meaningful rates of PFS and OS.66 Unsurprisingly, the patients with HER2 immunohistochemistry (IHC) 3+ tumors benefited most from T-DXd therapy.
mTOR inhibitors
The PI3K/AKT/mTOR pathway plays a central role in the regulation of many cell functions, including cell growth, protein translation and apoptosis.67 Dysregulation of the mTOR signaling is frequently observed in endometrial cancer and has been associated with developing resistance to hormonal therapy.68 Several rapamycin-analog mTOR inhibitors, including ridaforolimus, temsirolimus and everolimus, have been evaluated in endometrial cancer as monotherapy or in combination with other agents. The phase II GOG-3007 study (NCT02228681 assessed the combination of everolimus and letrozole versus an alternating medroxyprogesterone acetate/tamoxifen (MT) regimen in patients with metastatic endometrial cancer.69 The primary endpoint was response rate. At a median follow-up of 37 months, responses were similar between the treatment arms (22%, including one complete response [CR] with everolimus/letrozole vs 25%, including three CRs with MT), and the median PFS was 6 months versus 4 months, respectively. In the subgroup of chemotherapy-naïve patients, the median PFS with everolimus/letrozole was 28 months (vs 5 months with MT), whereas in patients previously treated with chemotherapy, the median PFS was 4 months versus 3 months in the everolimus/letrozole arm versus the MT arm. Common grade 3 AEs reported in patients receiving everolimus and letrozole versus medroxyprogesterone acetate/tamoxifen were anemia (24% vs 6%) and mucositis (5% vs 0%). Grade 3 thromboembolic events were reported in 11% of patients in the comparator arm and in 0% of patients in the experimental arm.
The combination of temsirolimus and bevacizumab was investigated in a phase II study (NCT00723255) of patients with recurrent or persistent endometrial cancer and 1–2 prior cytotoxic regimens.70 Primary endpoints were PFS at 6 months and ORR per RECIST. Clinical responses occurred in 24.5% of patients (including one CR and 11 partial responses) and 46.9% of patients had a PFS ≥6 months, with a median PFS and OS of 5.6 months and 16.9 months, respectively. Unfortunately, significant toxicity was reported with this regimen, including three deaths possibly related to treatment.
CDK4/6 inhibitors
Mutations in the cyclin D1/cyclin-dependent kinase 4 and 6 (CDK4/6)/Rb pathway are frequently observed in hormone-dependent tumors, including endometrial cancer.71,72 Since, similarly to breast and ovarian cancers, progression of endometrioid adenocarcinoma is dependent on both estrogen receptor (ER) and CDK4/6 signaling, it was hypothesized that the combination of endocrine therapy with CDK4/6 inhibition might have a synergistic effect in patients with endometrial cancer. Several phase II studies investigated combinations of letrozole with CDK4/6 inhibitors, including palbociclib, abemaciclib and ribociclib. The PALEO study showed improved PFS with palbociclib plus letrozole versus letrozole alone (8.3 months vs 3 months) in patients with ER-positive advanced/recurrent endometrial cancer.73 The addition of ribociclib to letrozole demonstrated promising clinical activity in relapsed ER-positive endometrial cancer, with a median PFS of 5.4 months and the proportion of patients alive, progression-free and still on treatment at 12 weeks of 55%.74 Abemaciclib plus letrozole demonstrated an ORR of 30% and a median PFS of 9.1 months in patients with ER-positive recurrent endometrial cancer, with responses observed regardless of tumor grade, prior hormonal therapy or mismatch repair and progesterone receptor expression status.75 Despite promising results, most patients on this study either did not respond or developed resistance to treatment. Combining PI3K and CDK4/6 inhibitors may represent a novel strategy to further enhance treatment efficacy, as demonstrated in a patient with recurrent endometrial cancer who exhibited partial response to combined aromatase, CDK4/6 and PI3K inhibition using the combination of letrozole, abemaciclib and LY3023414.76
Conclusions
-
The incidence of endometrial cancer is high in Switzerland, representing a significant health and economic burden.
-
The use of molecular subtyping in patients with endometrial cancer has improved tumor staging and treatment decision-making.
-
Immunotherapy, both alone and in combination with other therapeutic agents, has proven to be very effective in patients with advanced or recurrent disease, who represent a difficult treatment population.
-
The data presented at the ESMO 2023 and SGO 2024 congresses further support the ongoing use of immunotherapy in combination with SoC chemotherapy as a treatment option for patients with advanced or metastatic endometrial cancer.
Conflict of interest
PD Dr Marcus Vetter received honoraria for consultancy from GSK, Roche, Novartis, Exact Sciences, Pfizer, Stemline, AbbVie and ASC Oncology. Prof. Matthew A. Powell received honoraria for consultancy from GSK, Merck, Eisai, AstraZeneca, Seagen and Immunogen. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way.
Funding
The authors have declared that no financial support was received from any organization for the submitted work.
Author contributions
All authors contributed to and approved the final manuscript.