
Introduction
Chimeric antigen receptor (CAR) T-cell therapy, an innovative immune effector cell therapy approach that utilizes genetically modified T cells to eliminate cancer cells, has demonstrated remarkable efficacy in the treatment of certain hematologic malignancies and holds promise for autoimmune diseases and solid tumors. The generation of CAR T cells involves a leukapheresis to collect patient’s T cells from the bloodstream and their ex vivo modification to express CARs, synthetic fusion receptors that redirect T-cell effector function to the tumor.1 CARs consist of an extracellular domain that typically includes a single-chain variable fragment (scFv) conferring specificity to the target antigen, a transmembrane domain and an intracellular signaling domain comprised of CD3ζ and co-stimulatory domains that trigger T-cell activation upon antigen recognition.
While capable of producing long-lasting remission in malignancies that are resistant to conventional treatments, CAR T-cell therapy is associated with potentially severe toxicity, which can lead to organ damage and even death.
Unveiling the complexity of CAR T-cell toxicity
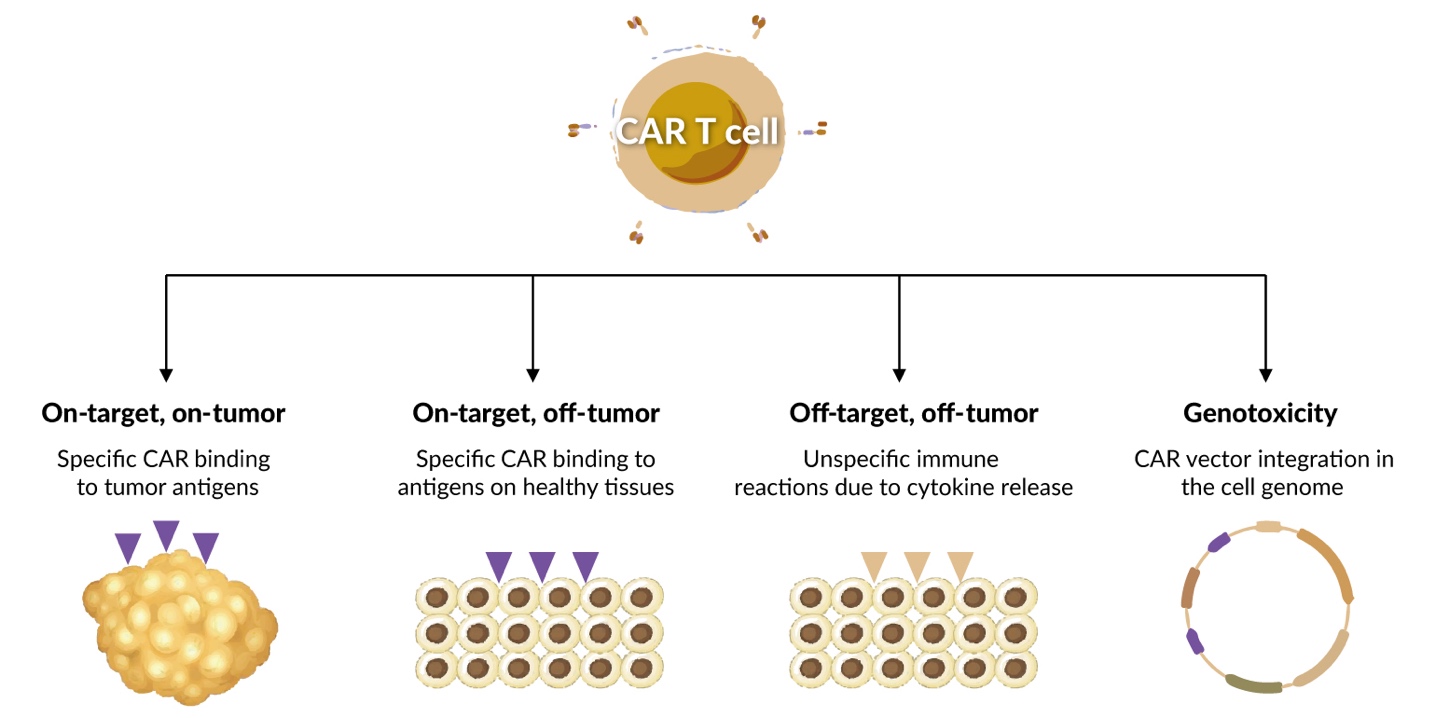
CAR T cells may induce toxicity through several mechanisms (Figure 1).2–4 On-target, on-tumor toxicity is caused by specific CAR binding to cognate antigens expressed on tumor cells. In the case of massive and rapid tumor cell death, this could lead to tumor cell lysis syndrome, a life-threatening condition associated with metabolic derangement, arrhythmias and renal failure in patients with high tumor burden.5 Moreover, successful CAR T-cell activation and proliferation, may result in an excessive immune response that will subsequently recruit and activate bystander cells such as monocytes, macrophages and dendritic cells. This leads to massive production of cytokines and chemokines, including interleukin (IL)-6, IL-10, interferon (IFN)-γ, IL-2, IL-4, tumor necrosis factor (TNF)-α and IL-17, leading to cytokine release syndrome (CRS), the most frequent side effect of the treatment.6 CRS manifests as fever and chills and, in severe cases, results in life-threatening conditions, including capillary leak and organ dysfunction. In addition to CRS, neurological toxicities, collectively referred to as immune effector cell-associated neurotoxicity syndrome (ICANS), can occur. ICANS, or CAR T cell-related encephalopathy (CRES), manifests as confusion, acute delirium, tremor and global aphasia and may progress to severe neurotoxic effects, such as seizures, status epilepticus, cerebral edema and coma.7 ICANS is caused by peripheral immune overactivation, blood-brain barrier dysfunction and central nervous system (CNS) inflammation. In addition, there is some evidence that CD19 is also expressed on perivascular cells within the CNS.8 ICANS is frequently observed following CRS but can also occur without prior CRS.
_t_cell-induced_toxicity.jpeg)
On-target, off-tumor toxicity is caused by the specific CAR binding to tumor-associated antigens (TAAs), which are also present in healthy tissues, leading to their damage. Its typical manifestation is long-term B-cell aplasia with consecutive hypogammaglobulinemia after CAR T-cell therapy of B-cell lymphoid malignancies caused by the redirection of CD19-targeting CAR T cells against normal B cells simultaneously with malignant CD19-positive (CD19+) blasts.9
Bone marrow inflammation, caused by CAR-T cells targeting healthy (and malignant) B cells in the marrow, may be one explanation for prolonged cytopenias of one or several blood cell lineages (off-target, off-tumor reactivity).10 Another example of off-target off-tumor reactivity is chronic toxicity due to the expansion of myeloid-derived suppressor cells in response to Th2-biased cytokine production caused by chronic CD4+ CAR T-cell activation.11 Off-target toxicity can result in various adverse events (AEs) depending on the affected tissues and organs, and is difficult to predict, making it a significant concern in CAR T-cell therapy. Finally, there is a potential risk of CAR T-cell genotoxicity and predisposition to secondary cancers due to the integration of CAR-expressing vectors into the cell genome and insertional mutagenesis, which has recently been communicated by the US Food and Drug Administration (FDA), since the FDA had become aware of 22 cases of T-cell cancers that occurred after treatment with CAR T-cell products (with a total of more than 27,000 doses of CAR-T cells infused).12 In three of these cases genetic sequencing was performed to date, and the CAR transgene has been detected in the malignant clone.
Choosing the right target for CAR T cells: approaches and challenges
The choice of the target antigen is crucial for the effectiveness and safety of CAR T-cell therapy. Selecting the right target can be challenging because of the weak immunogenicity of many TAAs, making them less responsive to CAR T-cell therapy. Furthermore, most target antigens are not restricted to the tumor tissue and are expressed on normal cells, with their engagement contributing to the side effects of the treatment. Currently, more than 1,300 clinical trials involving CAR T cells are registered at ClinicalTrials.gov. They investigated a wide range of TAAs as potential targets, including both validated antigens such as CD1913–18 and B-cell maturation antigen (BCMA),19,20 as well as novel molecules. Lesser-known emerging potential targets for CAR T-cell therapy are listed in Table 1. The simultaneous targeting of multiple antigens, such as a combination of CD19 and CD22, has also been considered to minimize tumor escape due to antigen loss.21 Preclinical models do not always accurately reflect the toxicity profiles of CAR T cells in humans, making the prediction of treatment side effects difficult, especially for first-in-human trials of novel target antigens. Additionally, the complexity of cellular and signaling processes triggered by T-cell engagement makes overcoming CAR T-cell toxicity a significant challenge and one major research goal in this field.
An example of severe toxicity in response to a novel target antigen is an early case report on the administration of T cells transduced with an ERBB2-targeting CAR based on the humanized monoclonal antibody trastuzumab, published in 2010.32 The patient was a 39-year-old female with metastatic ERBB2+ colon cancer metastatic to the lungs and liver and refractory to multiple standard therapies. An optimized γ-retroviral CAR vector containing CD28, 4-1BB and CD3ζ signaling domains was used to transduce autologous peripheral blood lymphocytes. The patient received ERBB2 CAR-transduced cells on the day following the last dose of the lymphodepleting regimen. Within 15 minutes after infusion, she experienced respiratory distress and pulmonary edema. The patient was intubated one hour post-infusion, developed severe hypotension requiring vasopressors, experienced two cardiac arrests in the next 12 hours and died after five days despite intensive medical intervention.
Postmortem examination revealed systemic ischemia and microangiopathic injury in multiple organs, diffuse alveolar damage in the lungs and generalized rhabdomyolysis.32 The highest level of CAR-expressing cells was detected in the lung and abdominal/mediastinal lymph nodes, with no preferential accumulation at metastatic sites. Serum samples showed markedly increased levels of IFN-γ, granulocyte macrophage-colony stimulating factor (GM-CSF), TNF-α, IL-6 and IL-10, which were consistent with a cytokine storm. The postulated cause of death was the transfer of highly active ERBB2-targeting CAR T cells, recognition of ERBB2 receptors in normal lung cells, release of inflammatory cytokines, pulmonary toxicity with edema, cascading cytokine storm and multiple organ failure. The investigators speculated that a large number of CAR T cells localized to the lung immediately after infusion and released cytokines owing to the recognition of low ERBB2 levels on lung epithelial cells.
Rare toxicities and complications of CAR T-cell therapy
In addition to the frequent toxicities described above, CAR T-cell infusion may result in a diverse array of rare AEs. According to published data from clinical trials and case reports, rare toxicities of CAR T-cell products can be grouped into several major categories. (1) Toxicity may be related to cellular infiltrations, inflammation and local cytokine secretion, especially when local inflammation affects critical locations. (2) As CAR T cells can easily reach neuronal tissues, they may affect neuronal structures or functions. (3) CAR T-cell infusion can lead to immune dysfunction, resulting in infectious complications. (4) Cardiovascular complications are prevalent in frail and heavily pretreated patients, with cytokine release contributing to cardiac dysfunction. (5) Since chemo- and radiotherapy often exert a genotoxic effect favoring the occurrence of secondary tumors, a chronically inflamed bone marrow environment and heavy pretreatment prior to CAR T-cell therapy may create conditions promoting hematopoietic complications and malignant transformations, including myelodysplastic syndrome (MDS) and acute myeloid leukemia (AML), particularly when clonal hematopoiesis of indeterminate potential (CHIP) is already present. (6) As mentioned above, rare cases of T-cell malignancies have been reported following CAR T-cell therapy, in some of which integration of the CAR-related genetic information was detected. (7) Finally, there are other complications for which the causal relationship with CAR T-cell therapy is not always convincingly demonstrated. The following sections discuss examples of rare CAR T-cell toxicities related to cytokine release, cellular infiltrations and neural tissue damage.
Complications related to (CAR T) cell infiltration and inflammation and cytokine release
Hashimoto’s disease following CAR T-cell therapy
Hashimoto’s thyroiditis is an autoimmune disease characterized by an enlarged or nodular thyroid gland with clinical manifestations of hyperthyroidism or hypothyroidism. Several studies have suggested that it may be mediated by T cells, with an imbalance between Th helper and T-cell function playing a role in disease progression. Chen et al. (2022) described two cases of Hashimoto’s thyroiditis after CAR T-cell therapy for R/R diffuse large B-cell lymphoma (DLBCL).33 A 65-year-old male achieved complete remission at three months post-CAR T-cell infusion. Subsequent ultrasound examination revealed a thyroid nodule and localized inflammation. The patient had elevated thyroid peroxidase antibody and thyroglobulin antibody levels but normal thyroid function, with T3, T4, and TSH levels within the normal range. The second patient, a 52-year-old female achieved complete remission one month after CAR T-cell infusion. During the follow-up examination, she exhibited elevated thyroglobulin antibodies, thyroid microsomal antibodies and thyroid peroxidase antibodies, but normal thyroid function. Secondary Hashimoto’s thyroiditis was diagnosed in both cases. The mechanisms linking CAR T-cell therapy to inflammation of thyroid tissue are not entirely clear and require further investigation.
CRS-induced cervical edema
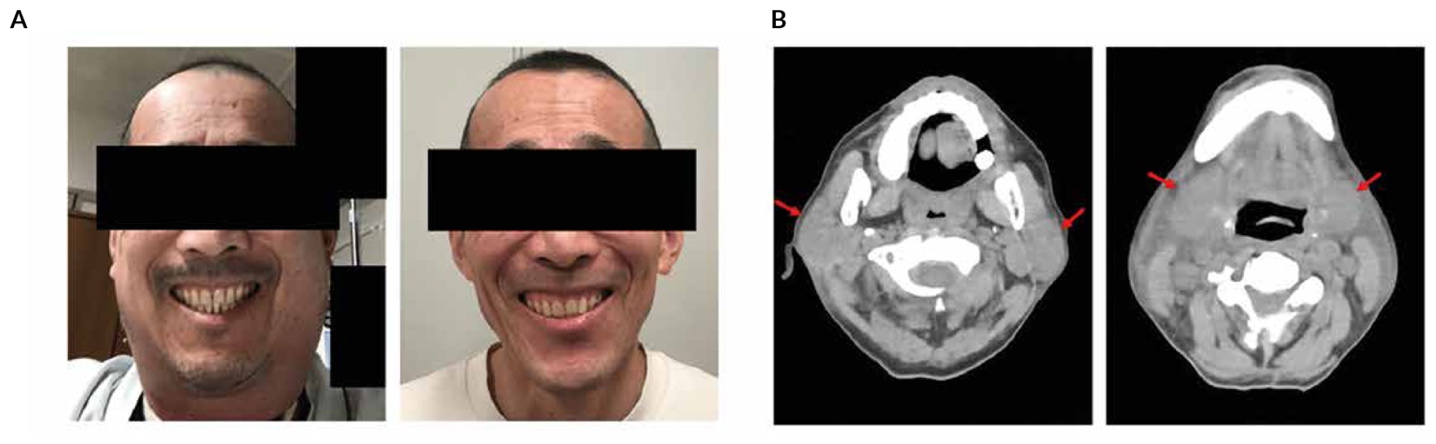
In addition to systemic CRS symptoms, CAR T-cell therapy may also cause rare acute inflammation at specific sites, known as localized CRS. High tumor burden increases the risk of developing localized CRS due to the expansion of CAR T-cells within the tumor mass. However, CRS-related cervical edema may be life-threatening even in patients without tumors in the neck area due to airway obstruction. A 60-year-old male patient received anti-CD19 CAR T-cell therapy with tisagenlecleucel (tisa-cel) for primary refractory DLBCL34 and experienced grade 1 CRS on Day 1, which required three doses of tocilizumab. On Day 5 he developed significant cervical edema without dyspnea or stridor (Figure 2), pancytopenia, slightly elevated C-reactive protein (CRP) and swelling of the bilateral parotid and submaxillary glands. Localized CRS was diagnosed in the salivary glands and surrounding tissues. The symptoms spontaneously improved on Day 7. Three months later, the patient had a complete metabolic response (CMR) and the cervical edema had resolved completely.
-induced_cervical_edema._a)_gross_appearance_of_cervical_sw.jpeg)
The second case involved a 70-year-old male with stage III DLBCL who experienced grade 1 CRS on Day 2 post-infusion and was treated with tocilizumab.34 On Day 3 he developed significant cervical edema, a muffled voice, anemia, a slight decrease in leukocyte counts, an elevated CRP and swelling of the posterior pharyngeal wall and laryngeal arytenoid on laryngoscopy. The symptoms improved immediately after dexamethasone treatment.
The other two patients developed cervical edema after receiving CAR T-cells for acute lymphocytic leukemia (ALL). A 15-year-old boy with refractory ALL exhibited persistent high fever (>39 °C) from Day 1 after infusion of tisa-cel.35 Despite tocilizumab and methylprednisolone administration, cervical edema extended to the larynx on Day 3, causing dysphagia and hoarseness, but resolved within hours after dexamethasone treatment. The fever gradually subsided from Day 8, and the patient sustained remission for 15 months after infusion. A 61-year-old female with relapsed Philadelphia chromosome (Ph)-like B-cell ALL developed grade 2 CRS within 12 hours post anti-CD19 CAR T-cell infusion.36 She was treated with tocilizumab, non-steroidal anti-inflammatory drugs, steroids and antibiotics. On Day 8, she complained of foreign body sensation in the larynx, dyspnea and facial edema with a rapidly growing neck circumference. After oxygen inhalation and administration of torasemide, methylprednisolone and dexamethasone, most symptoms, apart from the swollen neck, were relieved. The patient remained in complete remission for one year but eventually died due to disease relapse.
This clinically very impressive cervical swelling appears to be not extremely rare, as we and others have also observed it (unpublished).
CRS complicated with rhabdomyolysis
Rhabdomyolysis is a syndrome that results from skeletal muscle injury, causing leakage of intracellular contents into the bloodstream, which can damage the heart and kidneys, leading to disability or death. A 22-year-old woman with R/R ALL and an extremely low body weight of 35 kg received sequential infusions of CD19 and CD22-targeted CAR T-cells.37 On Days 2−3, she experienced a fever of 40.3 oC, irritability, photophobia, confusion, dizziness, headache, blurred vision and vomiting. On Day 7, the patient developed severe pain in both lower limbs and myoglobin and creatine kinase levels were significantly elevated, indicating rhabdomyolysis complication of grade 3 CRS. Following treatment with corticosteroids, tocilizumab, plasma catheterization and blood purification, the symptoms improved, and muscle weakness resolved after rehabilitation. The patient achieved complete remission six weeks after CAR T-cell infusion. This case demonstrates that myalgia, a typical symptom of rhabdomyolysis, can easily be overlooked during severe CRS after CAR T-cell therapy. Myoglobin levels should be monitored when a patient presents with myalgia or symptoms of acute renal insufficiency.
CRS complicated by arthritis of large joints
A 34-year-old male patient received CD19 CAR T-cell therapy for relapsed ALL.38 On Day 6 he developed a fever (38.9 °C), swelling and bilateral pain in the large joints of the limbs, which was particularly excruciating in the right wrist, both knees and the left ankle. CRS aggravated with multiple arthritis was diagnosed. The fever resolved within one hour following the administration of tocilizumab, but the pain progressively aggravated, and ultrasound indicated effusion in the large joints. The pain was alleviated with a high-dose combination of analgesic drugs, including methylprednisolone, and joint mobility gradually recovered. This case demonstrates that CRS following CAR T-cell therapy can manifest with symptoms similar to rheumatoid arthritis, which can be controlled with corticosteroids rather than tocilizumab.
Third-space effusions of CAR T cells
CRS in the pleural cavity
Localized CRS in the pleural cavity typically presents with respiratory symptoms including cough, shortness of breath, chest tightness and asphyxia. A 28-year-old woman with DLBCL and a highly aggressive disease course, presenting with a mediastinal mass, cervical lymph node and chest involvement, experienced localized CRS after receiving CD19-targeting CAR T cells.39 Next day she developed grade 2 CRS with a fever (39.3 °C) and was treated with anti-inflammatory medication. On Day 4, her cough worsened, and computed tomography (CT) revealed bilateral pleural effusion. Thoracentesis was performed, all symptoms had resolved by Day 9, and the pleural effusion was completely absorbed by Day 21. The investigators concluded that the localized CRS was caused by CAR T-cell trafficking into the pleural cavity and cytokine release in situ after direct interaction with lymphoma cells.
CAR T cell-induced cardiac tamponade
Acute pericardial effusion and cardiac tamponade associated with CAR T cell-induced CRS are very rare. A 65-year-old male with refractory DLBCL involving the pericardium was treated with axi-cel.40 On the day of the infusion, he developed grade 1 CRS with a fever of ≥38 °C and atrial fibrillation and was treated with tocilizumab and dexamethasone. Echocardiography revealed an acute pericardial effusion with signs of right ventricular heart failure due to cardiac tamponade, which appeared to be directly related to CAR T-cell expansion. Pericardiocentesis revealed a large number of lymphoma cells, with 73% of CAR T-cells among the lymphocytes. After pericardiocentesis, the patient’s hemodynamic status improved, with no recurrence of pericardial effusion. The patient died 50 days later due to disease relapse. This case highlights the importance of monitoring patients with pericardial DLBCL receiving CAR T cells for the risk of cardiac tamponade.
CAR T-cell infiltrates in critical locations
Bilateral retinal detachment
Localized complications affecting the retina and optic nerve associated with CD19-targeted CAR T-cell therapy were reported in a 13-year-old girl with high-risk B-cell ALL and CNS involvement.41 Following apheresis, the patient experienced a sudden decline in vision, which was attributed to bilateral leukemic infiltration of the optic nerve and retina. She received radiation therapy to the bilateral orbits, dexamethasone and chemotherapy, resulting in improved vision. However, upon admission for CAR T-cell therapy, the patient exhibited persistent bilateral leukemic infiltration of the optic nerve and retina, which worsened on Day 6 post-infusion. The examinations demonstrated bilateral retinal detachment, infiltrations, hemorrhages and leukocytosis in the cerebrospinal fluid (CSF), with 80% pleocytosis expressing T-cell-specific CD3. The local expansion of CAR T cells and cytokine release in the optic nerve and retina were hypothesized to cause retinal detachment. Intravitreal triamcinolone and orbital radiation markedly improved visual acuity. The patient achieved complete remission on Day 20 but experienced a loss of CAR T cells on Day 60 and CNS relapse, with sustained remission in the retina and optic nerve. After haploidentical peripheral blood stem cell transplantation, she remained in remission for 27 months after CAR T-cell therapy but subsequently developed cataracts as a complication of intravitreal triamcinolone, exacerbated by systemic steroids, local radiation and total body irradiation. This case highlights the potential risks associated with CAR T-cell therapy in patients with active retinal disease and the importance of recognizing and managing local inflammation to prevent vision loss.
Fulminant cardiotoxicity due to inflammation in the area of cardiac lymphoma infiltration
The severity of CRS-related cardiotoxicity may range from arrhythmia and left ventricular (LV) dysfunction to sudden cardiac death. A 44-year-old woman with relapsed DLBCL with CNS and cardiac involvement exhibited a response to salvage chemotherapy in terms of morphological improvement in the CNS.42 However, the disease progressed with infiltration of lymphoma cells in the pericardium, the right atrium and ventricular walls, the interatrial septum, the atrioventricular (AV) junction and encasement of the right coronary artery. Shortly after receiving CAR T-cell therapy with tisa-cel, the patient developed low-grade CRS with fever, tachycardia and hypotension followed by fulminant distributive shock and heart failure on Day 4. Despite receiving vasopressors, steroids and tocilizumab due to suspected higher-grade CRS, the patient’s condition continued to worsen, displaying intermittent right bundle branch block, supraventricular tachycardia and bradycardic atrial flutter with 3:1 conduction, which necessitated the placement of a temporary transvenous pacemaker on Day 7. In the following days, the patient exhibited persistent high-degree AV block alternating with atrial tachycardia, intermittent ventricular bigeminy and a concomitant increase in troponin T. After treatment with steroids and tocilizumab, perimyocardial lymphoma infiltration, edema and pericardial effusion decreased, biventricular function normalized, heart rhythm stabilized and troponin T levels started to decline. The transvenous pacemaker was left in place for 12 days and removed after a 6-day interval free of high-degree AV block or bradycardia. Unfortunately, five weeks after CAR T-cell infusion, the patient experienced CNS relapse and died after receiving palliative therapy. These results show that patients with cardiac lymphoma infiltration may be at a particular risk for severe cytokine-associated or cytokine-independent CAR T cell-mediated cardiac AEs. Prophylactic strategies, including the use of IL-6 receptor antagonists or steroids, are warranted.
CAR T-cell toxicities affecting neuronal structures and functions
Non-convulsive status epilepticus
In addition to common ICANS manifestations such as delirium, tremors and global aphasia, CAR T-cell infusion may lead to more severe neurotoxic effects, including non-convulsive status epilepticus (NCSE).43 In rare cases epileptic seizures following CAR T infusion can be highly refractory to medication, as exemplified by the 22-year-old woman with refractory DLBCL received axi-cel infusion reported by Reveron-Thornton et al.44 On Day 8, she displayed tachycardia, disorientation, naming difficulties, involuntary rapid low-amplitude asynchronous facial and upper extremity movements and a rapid decrease in the immune effector cell-associated encephalopathy (ICE) score. Grade III ICANS with grade I CRS was diagnosed. Treatment with tocilizumab, dexamethasone and prophylactic levetiracetam improved the ICE score; however, attention and word-finding deficits persisted. Continuous video electroencephalogram (cEEG) showed moderate diffuse slowing with rare generalized rhythmic delta activity (GRDA), indicating generalized encephalopathy without seizures (Figure 3A). On Day 11, the patient experienced multiple tonic-clonic seizures and was intubated due to hypoxic respiratory failure. Convulsive status epilepticus symptoms persisted despite administration of lorazepam, levetiracetam and phenobarbital but resolved after initiating a midazolam infusion drip. Broad-spectrum antimicrobials and methylprednisolone per the grade IV ICANS protocol were administered, leading to improved alertness with intermittent mental status fluctuations. On Day 17, her mental and neurological condition worsened. A cEEG showed sharply contoured 2.5–3 Hz continuous generalized periodic discharges (GPDs), consistent with generalized NCSE (Figure 3B), which persisted despite administration of lorazepam and phenobarbital but resolved after initiating a midazolam drip along with concurrent methylprednisolone and tocilizumab. Midazolam infusion was ceased on Day 19, resulting in improved mental status and a full ICE score by Day 24.
Seizures and GPDs have been attributed to CRS-induced thalamocortical hyperexcitability. This case underscores the challenges in managing refractory and the importance of prompt seizure identification and a multidisciplinary approach for effective symptom management.
_t-cell_infus.jpeg)
Bilateral facial nerve palsy
Bilateral facial nerve palsy is a rare neurological phenomenon associated with various systemic pathological conditions.45 A unique case of acute-onset bilateral simultaneous facial nerve palsy was described in a 76-year-old man who received anti-BCMA CAR T-cell therapy ciltacabtagene autoleucel (cilta-cel) for multiple myeloma.46 One week post-infusion the patient was diagnosed with grade 1 CRS. After two weeks, he developed rapidly progressive bilateral facial paresis, including the inability to close his eyes or eat without spilling food, dysarthria, and myalgia. Magnetic resonance imaging (MRI)/magnetic resonance angiography (MRA) findings indicated mild cranial nerve VII enhancement. The patient was empirically treated with acyclovir and dexamethasone, whereas levetiracetam was administered for suspected CNS involvement. On Day 21, the patient began to notice improvement in the symptoms of bilateral facial palsy and by Day 42, he completely recovered without showing further facial weakness or anisocoria. Although the exact mechanism of nerve palsy remains unclear, a higher relative concentration of T cells in the spinal fluid suggests a potential immune-mediated CAR T-cell toxicity, creating a complex neuroinflammatory environment and leading to neuropathy.
Diabetes insipidus and Guillain-Barré-like syndrome
Guillain-Barré syndrome (GBS) is a rare but serious immune-mediated neuropathy triggered by autoimmune damage to the peripheral nervous system causing numbness, tingling and muscle weakness that can progress to paralysis.47 A case of GBS and central diabetes insipidus (cDI) occurred in a middle-aged patient with high-grade B cell lymphoma with CNS involvement treated with tisa-cel.48 Within 24 hours post-infusion, he experienced grade 1 CRS, resolving with symptomatic treatment. On Days 5 and 6, the patient presented with House-Brackmann grade IV peripheral facial nerve palsy, discrete proximal limb motor weakness and grade 2 ICANS-associated disorientation. An MRI indicated gadolinium enhancement in the right facial nerve and possibly in the cauda equina, suggesting an immune-mediated etiology. Disorientation significantly improved with tocilizumab and dexamethasone treatment, whereas neuromuscular weakness worsened, resulting in incomplete quadriparesis and progressive impairment of respiratory muscle function and upper airway reflexes. Concurrent polyuria, along with decreased urine sodium concentration and osmolality, were consistent with cDI. CAR T cells were detected in the CSF, comprising 37% of mild lymphocytic pleocytosis. Weakness of the respiratory muscles necessitated mechanical ventilation and tracheostomy, while cDI was treated with desmopressin substitution. Suspected GBS based on clinical presentation and nerve conduction studies prompted the initiation of intravenous immunoglobulin therapy. Gradual but incomplete recovery of peripheral muscle function occurred over several months. This case emphasizes the potential risk of rare yet severe neurological adverse reactions, including acute GBS or cDI, in patients receiving CAR T-cell therapy.
Extensive myelitis with eosinophilic meningitis
An unusual case of extensive myelitis associated with eosinophilic pleocytosis occurred in a 52-year-old man with refractory mantle cell lymphoma treated with anti-CD19 CAR T cells.49 Starting from Day 1 post-CAR T-cell infusion, the patient experienced grade 1 CRS and was treated with antibiotics, tocilizumab and levetiracetam. By Day 3, the patient exhibited a complete and symmetrical lower limb motor deficit, areflexia, progressive lower limb anesthesia, saddle anesthesia and sphincter dysfunction. Examinations revealed extensive myelitis, infiltration of the cauda equina roots a lesion in front of the right lenticular nucleus and elements with 92% of eosinophilic polymorphonuclears in CSF. Following treatment with antibiotics, steroids and siltuximab, neurological symptoms stabilized, CSF cell infiltration decreased and MRI indicated reduced contrast enhancement throughout the spinal cord, with persistent extensive Short tau inversion recovery hypersignal. The neurological symptoms remained stable. Unfortunately, the patient died of an E. coli bloodstream infection on Day 11. This rare case of eosinophilic meningitis post-CAR T-cell therapy emphasizes the need for a more comprehensive understanding of ICANS pathogenic mechanisms.
Oropharyngeal and laryngeal dystonia
A 55-year-old female received CAR T-cell therapy with axi-cel for diffuse B-cell lymphoma (DBCL).50 Overnight she developed poor oral intake, mild hypotension and dizziness while standing which were managed conservatively with intravenous fluids and anti-emetics and resolved before discharge. Subsequently, she experienced an insidious progression of shortness of breath, dysphonia and intermittent stridor, prompting referral to a laryngologist. Examination revealed involuntary movement of the palate and pharynx with spasmodic adductor vocal-fold movement. Symptoms were limited to the oropharynx and larynx and resolved during sleep. Conservative treatments, including speech therapy, clonazepam, sertraline, omeprazole, gabapentin and antihistamines, were ineffective; however, bilateral vocal fold injections with botulinum toxin A improved voice quality and diminished laryngeal dystonia. After three months, an additional botulinum toxin A injection into the right vocal fold was required because of symptom recurrence. The patient was diagnosed as having adductor laryngeal breathing dystonia (ALBD). Although the investigators could not definitively prove the causation, they suggested a relationship between CAR T-cell infusion and ALBD.
Conclusions
Although CAR T-cell therapy has demonstrated efficacy in various types of hematological cancers, it can be associated with significant toxicity. In addition to the commonly reported and well-known side effects, there are also rare toxicities that target different organs and tissues. As the use of CAR T cells becomes more widespread, the list of rare side effects is growing, underscoring the need for a more comprehensive systematic description of these uncommon AEs, understanding their underlying mechanisms and developing prevention and management strategies to improve the clinical outcomes of the treatment. In the next issue of healthbook TIMES Oncology Hematology, rare CAR T-cell toxicities will be further discussed in the context of cardiovascular and hematopoietic complications, secondary malignant transformations and other rare side effects observed in clinical practice.
Conflict of interest
Prof. Antonia Müller has received honoraria for consultancy or expert opinion from Novartis, KITE/Gilead and Janssen, as well as honoraria for presentations and advisory board payments from Novartis, KITE/Gilead, Janssen and Celgene/BMS. These funding entities did not play a role in the development of the manuscript and did not influence its content in any way.
Funding
The author has declared that no financial support was received from any organization for the submitted work.
Author contributions
The author has created and approved the final manuscript.