






Introduction
Nearly all non-small cell lung cancer (NSCLC) patients without driver alterations in the metastatic setting and an increasing number in the locally advanced setting undergo programmed cell death protein 1/programmed death-ligand 1 (PD-[L]1)-directed immunotherapy (IO). In the perioperative setting, most studies imposed a maximum duration of IO of one year (Table 1). In some studies on metastatic NSCLC, IO is administered for a maximum of two years, whereas in others, it was administered until tumor progression (Table 2). Clinicians are frequently confronted with the following question: Is there a benefit for patients undergoing an indefinite duration of IO, or is it safe to conclude treatment after this two-year period? Furthermore, if cessation is considered, which specific patient groups can safely discontinue treatment? Unfortunately, a definitive answer to these questions is currently elusive owing to the scarcity of data. Nonetheless, there is an urgent medical need to thoroughly investigate the optimal duration of IO in metastatic disease.
How many patients complete two full years of IO?
In the KEYNOTE-024 study, in which pembrolizumab was compared to platinum-doublet chemotherapy in PD-L1 positive (tumor proportion score [TPS] ≥50%) patients, there were 34 (22%) patients that completed the full two years of treatment.1
The pivotal KEYNOTE-189 study compared and proved a substantial overall survival (OS) benefit for platinum and pemetrexed with placebo versus platinum and pemetrexed with pembrolizumab in non-squamous NSCLC patients. Of the patients randomly assigned to pembrolizumab plus pemetrexed-platinum, 57 (13.9%) completed 35 cycles of pembrolizumab and received a median of 35 (range, 2–98) cycles of pemetrexed.2
Another landmark trial for NSCLC is the KEYNOTE-407 study, which compared platinum and paclitaxel and placebo versus platinum and paclitaxel plus pembrolizumab in squamous NSCLC. Among patients randomly assigned to pembrolizumab plus chemotherapy, 55 (19.8%) completed 35 cycles of pembrolizumab.3
In the KEYNOTE-010 trial, pembrolizumab improved OS versus docetaxel in patients with previously treated, advanced NSCLC with PD-L1 TPS ≥50% and ≥1%; 79 (11%) patients completed 35 cycles of pembrolizumab.4
The treatment duration in the CheckMate 9-LA study was also restricted to a maximum of two years. In this study, chemotherapy with or without dual checkpoint blockade (ipilimumab and nivolumab) was investigated in squamous cell carcinoma and adenocarcinoma. After two years, 14% (out of a total of 358) of patients completed the IO.5
What about toxicity?
In terms of safety, immune-related adverse events (irAEs) typically manifest within the initial weeks to months following the initiation of treatment.6–8 Notably, the combination of cytotoxic T-lymphocyte associated protein 4 (CTLA-4)- and PD-1-directed treatment results in an earlier onset of AEs compared to singular anti-PD(L)1-directed treatment. After the two-year mark, there was a notable decrease in the incidence of side effects (Figure 1).
_in_patients_receiving_ipilim.jpeg)
Interestingly, in a pooled analysis from IMpower130, IMpower132 and IMpower150, a better outcome with a longer OS can be observed in patients in the IO treatment arm receiving atezolizumab who had low-grade immune-related AEs (Common Terminology Criteria for Adverse Events [CTCAE] grade 1 and 2). The median OS was 25.7 months (95% CI: 23.9–29.1) in patients with irAEs versus 13.0 months (95% CI: 11.7–13.9) in those without irAEs (Figure 2). It has to be stated that grade 3 to 5 irAEs as potentially life-threatening events were not associated with a longer OS compared to patients with grade 1–2 or without irAEs, since they often lead to long-term immunosuppression that may antagonize the effect of IO.9
_status_in_patients_with_non-sm.jpeg)
Is it feasible to do a rechallenge on IO?
In the KEYNOTE-024 trial, among 12 patients that were subsequently rechallenged with IO, four patients had a partial response (PR) and six cases of stable disease (SD) again (Figure 3).1

In the KEYNOTE-010 trial, the OS rate at three years after completion (approximately five years from randomization) was 83.0%. A total of 21 patients received second-course pembrolizumab; 11 (52.4%) had an objective response, with another six patients presenting with SD (81% disease control rate) after starting the second course (Figure 4). It should also be noted that in the 5-year survival update, at data cut-off, 41 patients (43%) in the PD-L1 ≥50% group and 51 (35%) in the PD-L1 ≥1% group receiving pembrolizumab had an ongoing response without needing second-line treatment.4 The outcomes of patients with complete response (CR) or PR tended to be better than those with SD after cessation of immune checkpoint inhibitor (ICI) therapy at two years, although this conclusion was not based on randomized data. Similar results were obtained in a real-life study that analyzed survival in patients with advanced NSCLC who discontinued ICI monotherapy after at least 18 months in the setting of controlled disease.10 Duration of disease control after treatment discontinuation was correlated with tumor response at discontinuation: the 12-months progression-free survival (PFS) rate was 76% in patients with CR or PR compared with 22% in those with SD as the best response (p=0.0002).10

Nivolumab-retreatment in NSCLC patients who responded to prior IO and had an IO-free interval was prospectively investigated in the WJOG9616L study. In this trial, patients who had at least SD, CR or PR for at least six months undergoing IO and an IO-free interval of a minimum of 60 days were retreated with nivolumab. Among the 59 patients analyzed, the median ICI-free interval was 9.2 months. Nivolumab retreatment demonstrated only a very low overall response rate (ORR) of 8.5% (95% CI: 2.8–18.7) and median PFS of 2.6 months (95% CI: 1.6–2.8) while five responders had 11.1 months of median PFS, showing an only very limited efficacy of IO rechallenge in this cohort. ICI-free interval was the only predictive factor of PFS (HR: 2.02; p=0.02) (Figure 5).11

These conflicting findings do not definitively provide an answer regarding the feasibility of IO rechallenge after discontinuation of initial IO treatment. However, it is crucial to note that the described cohorts are entirely distinct. In cases in which a patient exhibited a positive response to IO treatment and completed the two-year course, a rechallenge may be considered feasible even in the event of progression following treatment completion. Once resistance is acquired, IO retreatment may have limited efficacy.
The role of targeting vascular endothelial growth factor (VEGF) in addition to PD-(L)1 to enhance the immune response may further improve the effect of IO therapy when performing a rechallenge. This concept was evaluated in the phase II Lung MAP S1800 trial. This study included patients with NSCLC who had been previously treated with IO and platinum-based chemotherapy. Patients were randomly assigned to receive ramucirumab plus pembrolizumab or the investigator’s choice of standard-of-care chemotherapy (docetaxel/ramucirumab, docetaxel, gemcitabine and pemetrexed). OS was significantly improved with VEGF targeting plus IO (HR: 0.69). The median OS was 14.5 months in the experimental arm and 11.6 months in the chemotherapy arm, with an OS benefit in most subgroups.12
Another interesting study addressing the question of IO treatment duration is an exploratory analysis of CheckMate 153 that evaluated continuous versus one-year fixed duration of nivolumab in pretreated NSCLC.13 In the continuous treatment arm, 89 of 127 patients were progression-free at one year and 85 of 125 patients were progression-free in the one-year treatment arm. This study showed a longer PFS in the continuous treatment arm compared to the fixed-duration arm (24.7 vs 9.4 months, HR: 0.56 [95% CI: 0.37–0.84]). Also mean OS from assignment was higher in the fixed-duration arm (not reached vs 28.8 months; HR: 0.62 [95% CI: 0.42–0.92]). This study demonstrates the benefit of continuing IO treatment for more than one year, especially when patients had a CR/PR at one year (Table 3).

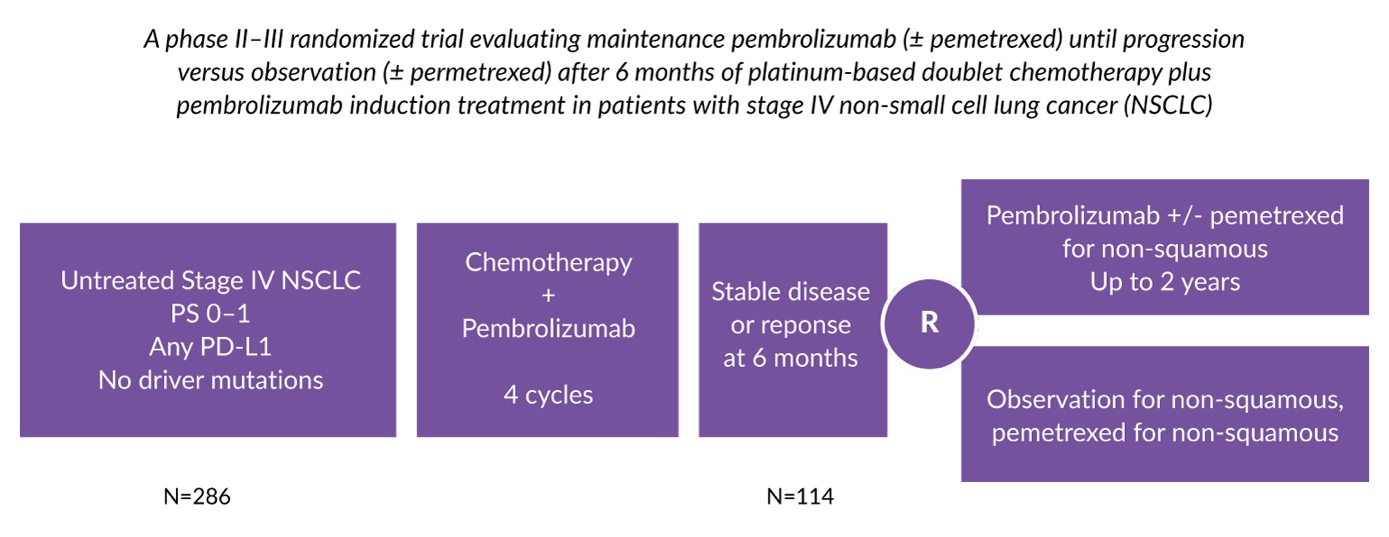
One trial that will try to answer the question of whether IO can be discontinued already after four cycles of chemotherapy and pembrolizumab in patients who have reached a response is IFCT-2103. In this trial, NSCLC patients will be randomized to observation (plus pemetrexed in non-squamous NSCLC) versus continuing pembrolizumab (plus pemetrexed in non-squamous NSCLC) up to two years (Figure 6).14

What role does ctDNA testing play in evaluating the duration of therapy?
Similar to its utility in other tumor types, circulating tumor DNA (ctDNA) proves to be valuable in guiding therapeutic decisions, particularly in cases with radiological response and can predict recurrence risk in the adjuvant setting in NSCLC.15–21 Hellmann et al. conducted a study involving 31 NSCLC patients with long-term benefit from immune checkpoint blockade therapy.22 All patients underwent ctDNA analysis prior to the initiation of therapy, with a subsequent measurement at a median of 26.7 months. In the analyzed group, 27 patients exhibited undetectable ctDNA, and of those, 25 (93%) remained progression-free. In contrast, all four patients with detectable ctDNA eventually experienced disease progression. This study underscores the potential of ctDNA surveillance in personalizing the duration of immune checkpoint blockade and facilitating early intervention in patients deemed at a high risk for progression (Figure 7).
_predicts_disease_progression_in_patients_with_non-small_cell.jpeg)
Conclusions
Until now, we are still trapped in the dark if it is reasonable to continue IO treatment for more than two years in the metastatic NSCLC setting. Further data evaluating the role of ctDNA measurements and positron emission tomography/computed tomography (PET/CT) scans are urgently needed. If PET/CT is performed (even though there is yet no clear evidence favoring it over conventional CT scans) after two years and shows no18F-fluorodeoxyglucose (FDG)-avid lesions, treatment discontinuation should be discussed with our patients on an individual basis. Patient preferences as well as regulatory limitations must be involved in decision-making. Furthermore, patients suffering from low-grade IO side effects may have better treatment outcomes, even if they received only a few cycles of IO treatment. Consequently, this patient population may have a lower risk of discontinuing therapy. Financial toxicity and late-occurring side effects of IO treatment favor discontinuation after two years. In patients with progressive disease after having stopped IO, reinduction of IO (with or without VEGF targeting) seems to be an effective option.
Conflict of interest
Dr Sebastian Kraus serves as principal investigator for Astra Zeneca, Daiichi Sankyo and GSK and has received advisory board payments from Roche, Janssen, Servier, Astra Zeneca and Sanofi, as well as travel grants from several pharmaceutical companies. Prof. Mathias Schmid serves as principal investigator for Roche and received advisory board payments and travel grants from several pharmaceutical companies. The funding entities and sponsors of the authors did not play a role in the development of the manuscript and did not influence its content in any way.
Funding
The authors have declared that no financial support has been received from any organization for the submitted work.
Author contributions
All authors contributed to and approved the final manuscript.